-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Surgical Research
2013; 2(4): 37-41
doi:10.5923/j.surgery.20130204.03
Routinevs Day-Care Surgery in Case of Unilateral Inguinal Hernia in Public Hospital Setting
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJeetendar Paryani, Gunvant H. Rathod, Rakesh A. Makwana, Ravi P. Gadani, Rajesh K. Patel
Department of Surgery, Civil Hospital Ahmedabad, Gujarat
Correspondence to: Jeetendar Paryani, Department of Surgery, Civil Hospital Ahmedabad, Gujarat.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Day-care surgery is defined as planned investigations or procedures on patients who are admitted and discharged home on the day of their surgery. In this prospective and observational study on 100 patients --50 day-care + 50 routine-care patientswho underwent treatment of unilateral inguinal hernia at Civil Hospital and B. J. medical college, Ahmedabad. Weaim to study and compare the immediate and long-term post-operative complication and patients’ satisfaction between the two procedures (day-care and routine-care) to assess the feasibility of day-care surgeries in government institutes. In the study, 2 out of 50 (4%) day-care surgery patients had to be kept for more than 23 hours. Only 1 out of 50 patients (2%) was readmitted. The readmission rate of 2% is at par with 2-3% recommended by Royal College of Surgeons. The immediate post-operative and at the end of 7th post-operative day complications were infact lower than routine-care surgery. Majority of patients (94%) were satisfied from the surgery and preferred day-care surgery to routine-care. Also, the success rate, complication rate and patient satisfaction were comparable with specialized day surgical unit treating for inguinal hernia. From our study, we may conclude that even with the shortcomings of the public health care setup of developing nation, the day-care hernia repair can be done without any major immediate or long term complication ascompared to routine-care surgery.
Keywords: Day-care Surgery, Public Hospitals, Unilateral Inguinal Hernia
Cite this paper: Jeetendar Paryani, Gunvant H. Rathod, Rakesh A. Makwana, Ravi P. Gadani, Rajesh K. Patel, Routinevs Day-Care Surgery in Case of Unilateral Inguinal Hernia in Public Hospital Setting, International Journal of Surgical Research, Vol. 2 No. 4, 2013, pp. 37-41. doi: 10.5923/j.surgery.20130204.03.
Article Outline
1. Introduction
- Day-care surgery is defined as planned investigations or procedures on patients who are admitted and discharged home on the day of their surgery but who require some facilities and time for recovery[1]. In most countries this means that the patient spends a few hours in hospital and does not stay overnight. However in USA and a few other countries, it includes patients who may spend up to 23 hours in hospital. In this study, the 23 hours criterion is followed.Day-care surgery is not a new concept; infact theearliest report is in 1909 by a Glosgow surgeonJames Nichol[2], but the concept did not become popular till 1960 when first hospital based ambulatory unit was developed[3]. In the day-care, the patients and the procedures are selected in such a way so as to cause minimal harm or disturbance to the patient and his life. One has to be very careful and judicious in selecting the appropriate procedure and patients as otherwise it can lead to major complications. All the preparations and facilities required in a major surgery should be met with in a day-care procedure.Inguinal hernias occur in about 15% of adult men and hernioplasty is the most common surgical procedure performed by general surgeons[4]. The repair of inguinal hernia provides a major surgicalworkload which is the reason for us to choose inguinal hernias repair for this study.As the concept of day-care surgery is yet to flourish in India, especially in Government setups, care needs to be exercised in explaining the patients this ‘new’ concept. The concept is not very popular in the setup because of many factors. First and foremost is the reluctance of the caregivers to provide such service to the patients. Day-surgery is an innovative approach to surgical health care and, as inall innovative situations; there may be initial resistance to change[5].Secondly, the large number of patients received in the outdoor department makes it difficult for doctors to segregate the patients suitable for day-care surgery and provide counseling and directions to the patients needed for day-care surgery.The patient factors play an important role in the day-care. Patients need to becounseled thoroughly for the service and foretold about the instructions for the same. Due to false belief of the patients that beingunder supervision (routine-care surgery) in hospital is better, it is difficult to convince the patients in Government setups to go for day-care surgery.Such factors lead to underuse of day-care surgery in government institutions.Also the lack of specialist day surgery unit and lack of support infrastructure-- shortfall of presence of General Practitioners (GP) nearby, absence of caretaker of the patient at the home, distance from the hospitals etc. affect the day-care surgery.However, day-care surgery in public health care setup is the need of the hour. In a government / public hospital with tremendous workload in surgical departments, day procedures help in making indoors beds free for the admissions of other patients who need to be hospitalized. In the long run it is cost effective to both the hospitals and the patients.In addition, ‘a day procedure’, makes it look like a ‘minor’ surgery to the patient; therefore reduces the anxiety of the surgery. Being a day procedure, it reduces hospital stay and hence reduces the chance of hospital acquired infections. The recovery after day-care surgery is faster in familiar surroundings, which is very important for recovery of patients of older age group and children. Day-care surgeryalso leads to early resumption of day to day work for working population. In this study, we show that day-care surgery is possible and successful even with above mentioned shortcomings. This study makes an effort to prove that the day-surgery for Inguinal hernia can be done in public health care setup safely and successfully without any specialist day- surgery units.
2. Methods
2.1. Data Collection
- In the present study, 50 cases of day-care and 50 cases of routine-care surgeries were studied at the Civil Hospital and B.J Medical College Ahmedabad. It is a tertiary referral center catering to referrals from entire state of Gujarat, Madhya Pradesh and Rajasthan. All patients admitted to Civil Hospital, Ahmedabad who underwent an operation for treatment of unilateral inguinal hernia during the period from May 2008 to March 2013 were eligible. In the study the day-care surgery was defined as the surgery in which the patient was discharged within 23 hours of admission. A proforma was made to record the details of the patient and the surgery, thus closely following the patient pre, intra and post operatively. Various complications, the number of patients requiring unplanned admissions or re-admission, patient satisfaction were emphasized upon.Patients were asked what they would prefer if they develop hernia on the contralateral side and what they would recommend to friends and relatives. Patient satisfaction was measured in terms of percentage of patients recommending day care surgery for both situations.For day-care surgeries, the patient selection criteria included presence of a responsible escort and access to a telephone. Patients were counseled during the outdoor department and explained the procedure of day-care surgery.They were given a contact number to contact in case of any doubt. Also their contact number was noted and instructions were given to them on the phone in case of need. They were operated under local, spinal or general anaesthesia as decided by an anesthesiologist, keeping in mind that the patient will be preferably discharged on the evening of surgery.For day-care surgeries, the patient discharge criteria included vital signs for atleast one hour, patient orientation to time, place and person, able to tolerate fluids, to void and to walk, and minimal nausea, vomiting and pain. Prolonged stay was defined as duration of hospital stay exceeding 23 hours. Patients were given instructions to call if there was any discomfort and return to the hospital in case of any distress. Patients were followed up of seventh day after surgery. Patient requiring to be admitted before this duration were defined as readmission. All other patients were termed to have successful surgery.
2.2. Analysis of Data
- Data was analyzed to study the variables such as age, type of surgery, day-care vs.routine-care, duration of stay, type of anesthesia, post-operative complications—immediately and at the end of post-operative day (POD) 7, and patient’s satisfaction.The above variables were compared in two groups: day-caresurgery (group A) and routine-care surgery (group B). Comparisons also have been drawn against previous studies on day-care surgeries. Chi-square (χ2) and student-t testswere used to compare variables and tests were considered significant when P-Value < 0.05.
3. Results
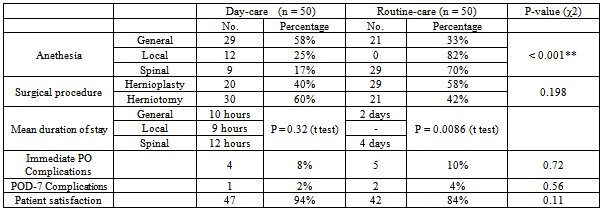
- A total number of 100 patients--50 day-care and 50 routine-care were operated for unilateral inguinal hernia in the age group 1 year to 70 years in day-care surgery group and 1 to 78 in routine-care surgery group.The mean and median ages in group day-carewere 23.39±3.64 and 11years respectively andin group routine-care were 27.55±3.62 and 20years respectively. The mean ages were not significantly different (t stat = 0.811, p = 0.41) in two groups which showsmean age was comparable in two groups.Hernioplasty procedure compared to herniotomy was done on lower percentage of patients in day-care (Figure 1). Herniotomy is more commonly done in children where mesh is not required and procedure is short and simpler. However, percentage of patients undergoing harniotomy/hernioplasty were not significantly different in two groups (χ2stat= 1.659, p = 0.198) (Table 1). Hence in the study both the groups were comparable procedure wise also.Out of 50 day-care surgeries, 29 (57.5%) were carried out under General anaesthesia, 12 (25.0%) were under Local anaesthesia, and 9 (17.5%) were carried out under Spinal anaesthesia. While, out of 50 routine-care surgeries, 21 (42.5%) were under General anaesthesia, 29 (57.5%) under Spinal anaesthesia, and no patient was given Local anaesthesia. The percentages of the type of anaesthesia under the two groups were significantly different (χ2stat = 20.257), p < 0.001) (Table 1). Day-care surgeries done under Local anesthesia were associated with the least mean duration of stay (10 hours), whereas those done under Spinal anesthesia were associated with the highest mean duration of stay (12 hours). The mean duration of stay was not significantly different in three types of anesthesia (t stat = 0.84, p =0.32). Routine-care surgeries done under General anethesia were associated with the shorter mean duration of stay (2 days) compared to the surgeries done under Spinal anethesia (4 days) which was significantly different in both types of anesthesia.(t stat = 2.84, p = 0.0086) (Table 1).Under the day-care surgeries, 4 patients had minor immediate post-operative complications out of which 3 suffered from anaesthesia-related complications (urinary retention and vomiting & nausea) and 1 suffered from surgery-related complication (pain). Whereas, under the routine-care surgeries, 5 patients had immediate post-operative complications out of which 3 had urinary retention, 1 had pain and 1 had vomiting and nausea. Number of immediate complications in two groups did not differ significantly (χ2 stat = 0.122, p = 0.72) (Table 1). As shown in the Figure 2,2 out of 50 (4%) day-care surgery patients had to be kept for more than 23 hours (prolonged stay). Only 1 out of 50 patients (2%) was readmitted. The readmission rate of 2% is at par with 2-3% recommended by Royal College of Surgeons.
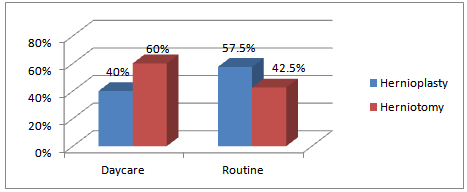 | Figure 1. Comparison of Surgical Procedure |
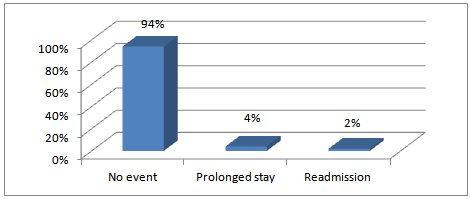 | Figure 2. Prolonged & Readmission rates for Day-care surgeries |
|
4. Discussion
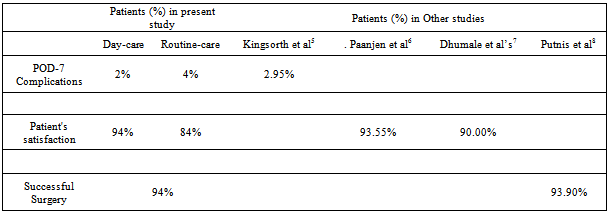
- Inguinal hernia surgery forms a substantial proportion of the general surgical workload. Inguinal hernia repair is ideally suited to day surgery and increasing numbers of procedures are being performed in this setting[6]. This reduces the inconvenience and risk to the patient associated with in-patient (routine-care) hospital stay and also substantially reduces the cost associated with the surgery[7].In the present study, the upper age was limited to 70 years in day-care surgeries so as to avoid major complications in the older patients. However, in the study by N. Mishra et al, patients’ age ranged between 1 month and 90 years, and in the study by E. O. Oje et al, age ranged between 1 week and 100 years[8]. Similar to our results, in both of these studies, there were no major post-operative complications. Hence, day-care surgery may be suitable for all age groups ranging from 1 week to 100 years.The Surgeries done under General and Spinal anesthesia are associated with longer stay as compared to those done under Local anesthesia. Hence normally in day-care surgeries, Local anaesthesiais the preferred mode of anaesthesia. It also avoids the complications of General anaesthesia such as post-operative nausea and vomiting (PONV), drowsiness etc. and the complications of Spinal anaesthesia like urinary retention. However patients of pediatric age group are operated under General anaesthesia. In our study also, majority of day-care surgery patients were operated under Local/General anaesthesia and only 9 out of 50 patients were operated under Spinal anaesthesia.In the present study, 1 patient out of 50 developed recurrent urinary retention and had to be readmitted. Other than urinary retention, there was no anaesthesia related complication causing readmission. In the study by T. Naresh Row et al, one patient out of 75 required readmission due to excessive drowsiness and four patients had urinary retention for which urinary catheterization was necessary[9]. They were discharged home with catheter. In our study, none of the patients were discharged with catheter or drain.In this study, only 2% patients under the day-care surgeries had complications on post-operative day-7 compared to 4% under the routine-care surgery and 2.95% under the study by Kingsorth et al.[10]. However, their follow-up time was very long-- > 2 years) (Table 2). 94% patients in our study had a satisfactory experience with day-care surgery, whereas only 84% patients had a satisfactory experience with routine-care surgery. Paanjen et al. reported the similar rate of patient satisfaction (93.55%), whereas Dhumale et al reported only 90% patients satisfaction rate (Table 2)[11, 12]. Surgery was successful in 94% of patients in the present study, same as success rate reported by Putnis et al (Table 2)[13].Much has been said about the requirement of specialized day-care surgery unit for continuing this strategy. The special setup which includes a surgical consultant, dedicated staff and operation theatres for day-care surgery sure streamlines the procedure and allows for greater satisfaction for the patients. But, often the lack of these units in public health care setup has been used as reason for denying patients the benefits of day-care surgery.However, we show in our study that day-care surgeries done in general surgical unit without any specialized unit did achieve high patient satisfaction and low complication rate compared to routine-care surgeries, suggesting that day-care surgeries can be performed successfully in public health care setup without day-care unit or surrounding specialized support infrastructure.
|
5. Conclusions
- Even with the shortcomings of the public health care setup of developing nation, day-care surgery for unilateral hernia repair in patients can be managed without significant complications as compared to routine-care surgery. Results are comparable to standardized day-care units also.Looking at the advantages of reduction of hospital stay and greater satisfaction, day-care hernia should be promoted. Day-care surgery could be expanded in government setups for inguinal hernia and many other surgeries.