-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Surgical Research
2013; 2(4): 34-36
doi:10.5923/j.surgery.20130204.02
Type Iv-A Choledochal Cyst-A Case Report
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJeetendar Paryani, Gunvant H. Rathod, Rakesh A. Makwana, Ravi P. Gadani, Rajesh K. Patel
Department of Surgery Civil Hospital Ahmedabad, Gujarat
Correspondence to: Jeetendar Paryani, Department of Surgery Civil Hospital Ahmedabad, Gujarat.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Choledochal cyst is a congenital cystic dilatation of the bile tract; it can beextrahepatic, intrahepatic biliary radicles, or both. It is a rare condition occurring more commonly in the developing countries (100 times more common in Japan) than in the west and these congenital lesions have a female bias (4 times more commonly than in males). We report a very rare case of Type IV-A (abnormally large-size) in a 15- year’s old girl. She presented to the outpatient clinic with a history of recurrent pain and jaundice with fever for 2 months. The preoperative diagnosis was huge choledochal cyst about 20*10 *11 cm in size. The patient made complete recovery after cyst-excision with Roux-en-Y hepaticojejunostomy. Early suspicion of this rare disease is important because surgical treatment is the only way to avoid the dramatic complications of this disease. In the case report we discuss the history, clinical features, investigations, complications and treatment of this large size choledochal cyst.
Keywords: Choledochal Cyst, Rare, Large, Type IV A
Cite this paper: Jeetendar Paryani, Gunvant H. Rathod, Rakesh A. Makwana, Ravi P. Gadani, Rajesh K. Patel, Type Iv-A Choledochal Cyst-A Case Report, International Journal of Surgical Research, Vol. 2 No. 4, 2013, pp. 34-36. doi: 10.5923/j.surgery.20130204.02.
1. Introduction
- Choledochal cyst is an aneurysmal dilatation of the bile ductinvolving the extrahepatic biliary radicles, the intrahepatic biliary radicles, or both.It is a rare condition occurring more commonly in the developing countries (I00 times more common in Japan) than in the west[1, 2, 3]. These congenital lesions have a female bias occurring in 4 times more commonly than in males[1, 2, 3, 4]. Presentation with the classic triad of pain, jaundice, and an abdominal mass occurs rarely that is only in 6% of the cases[1, 3, 4].Todani in 1977 classified choledochal cystsinto 5 types based on site of the cyst or dilatation[5]. Type IV-A is characterized by multiple dilatations of both--the intrahepatic and extrahepatic biliary tree whereas type IV-B is characterized by multiple dilatations of only the extrahepatic bile ducts. We describe a case of an unusal size of type IV-A choledochal cyst which showed massive cystic dilatation of the common bile duct (CBD).
2. History
- A 15 year-old previously healthy girl was admitted into Civil Hospital of Ahmedabad, Gujarat with the complaints of recurrent pain and jaundice with fever for 2 months.A sudden severe localized pain first appeared about two months back. It was associated with high-grade, intermittent fever with chills and severe vomiting. It subsided by taking antipyretics within 3 days.She noticed a lump on her right upper abdomen, which had been gradually increasing in size for last 2 weeks. She developed yellow coloration of sclera and urine, which was relieved intermittently with the relief of episode of fever and abdominal pain. Thereafter she had several episodes of sudden, dull aching,localized right upper abdominal pain persisting for few hoursand relieved spontaneously.
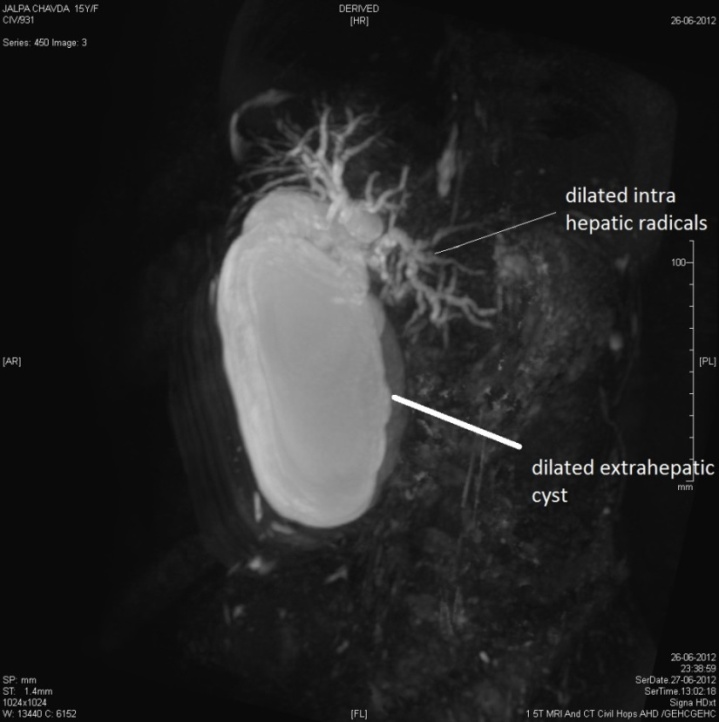 | Figure 1. 3d Reconstruction of Mrcp |
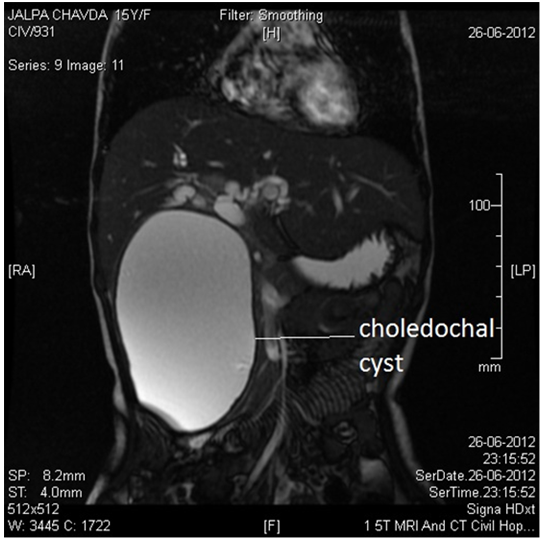 | Figure 2. Coronal section of MRCP |
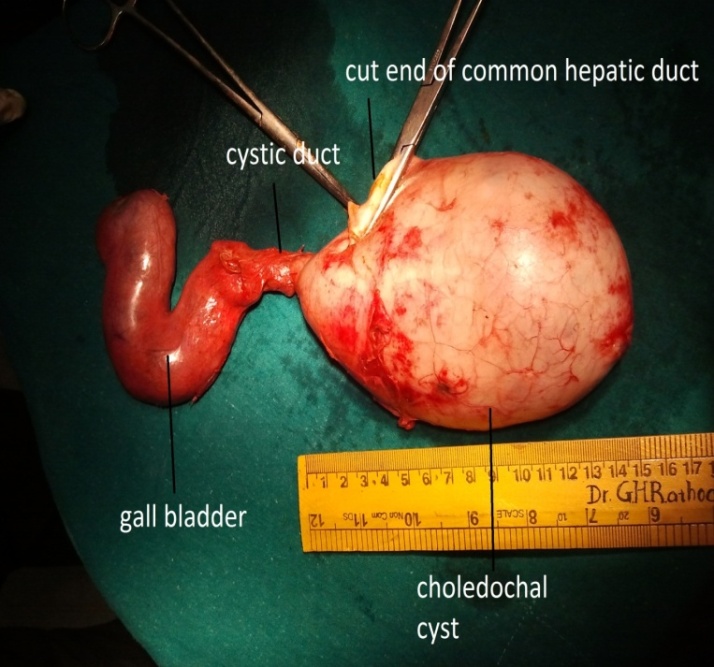 | Figure 3. The specimen |
3. Discussion
- Choledochal cysts are congenital conditions involving cystic dilatation of bile ducts which may be due to the anomalous junction of the common bile duct (CBD) with the pancreatic duct which was first brought to light by Kozumi and Komanda in 1916[6]. But not until Babbit in 1969 was this accepted universally[7]. An anomalous pancreatic bile duct junction (APBJ) is defined as the junction of the pancreatic duct with the CBD 1cm or more proximal to where the CBD reaches the ampulla of Vater. The APBJ causes pancreatic secretions and enzymes to become activated which results in inflammation and weakening of the bile duct wall. Severe damage may results in complete denuding of the CBD mucosa.Several types of choledochal cysts are recognized. Type I is the most common variety (80-90%) involving fusiform dilatation of a portion or entire CBD. Type II is isolated diverticulum protruding from the CBD.Type III or Choledochocele arises from dilatation of duodenal portion of CBD or where pancreatic duct meets.Type IV-A is characterized by multiple dilatations of the intrahepatic and extrahepatic biliary tree whereas type IV-B has multiple dilatations involving only the extrahepatic bile ducts.Type V or Caroli’s disease involves cystic dilatation of intrahepatic biliary ducts. The size of choledochal cyst varies, and rarely exceeds 9 cm (in our case 11cm)[8].The classical presentation of choledochal cyst in children is jaundice, abdominal mass and abdominal pain[1, 3, 4],but very few patients (6%) present with classical triad as our patient presented[7]. The most common presentation is jaundice followed by pain and mass whereas in adults most common presentation is abdominal pain[3].Transabdominal ultrasound—a widely available, cheap, easily reproducible investigation is the bestinitialinvestigation for biliary tract. Our patient was initially screened with ultrasound abdomen for the jaundice and abdominal lump which was suspicious of type IV-A choledochalcyst. MRCP is the gold standard imaging for evaluation of choledochal cyst. In our case MRCP confirmed the presence of huge Choledochal cyst with intrahepatic as well extrahepatic components.If untreated choleodochal cyst produces liver damage, which progress to biliary cirrhosis and portal hypertension with all its manifestations[9]. Also it may cause other life threatening events like pancreatitis and cholangitis. Not only that the patient is also at very high risk for having cholangiocarcinoma. Fortunately our patient was diagonosed at very early age and none of these complications occurred.Once diagnosed the choledochal cyst is treated surgically. Careful identification and protection of the orifice of the pancreatic are mandatory. Surgical treatment of the choledochal cyst is complete cyst excision followed by bilioenteric anastomosis.Type I cysts are resected and bilary apparatus is reconstructed byhepatico-jejunostomy with a Roux-en-Y segment of jejunum.Type II cyst can be usually resected with the defect in the C.B.D primarily suture over a T-tube which is brought out through a separate incision in the duct.Type III cyst is approached through the duodenum by either a trans-duodenal sphincteroplasty or endoscopicsphincterotomy[10].Rest of the types constitutes a difficult management problem. Patient with type IV-A,choledochal cyst are best treated with extra hepatic cyst excision and bilioenteric anastomosis which significantly reduces the chances of cholangiocarcinoma.If only left lobe is involved, then left hepatectomy may be done. The bilioenteric anastomosis is achieved using Roux-en-Y hepatico-jejunostomy. In our patient the dilated intrahepatic ducts were not localized to left lobe thus not been amenable to partial hepatectomy. Therefore decision to do extra hepatic cyst resection and bilioenteric anastomosis was done.In conclusion, the classical presentations of choledochal cysts are quite rare. Also the occurrence of such large cyst of type IV-A is very uncommon.Initial screening can be done by means of ultrasound abdomen. If it is suggestive of such lesions, MRCP should be done as it is gold standard for evaluation abnormal biliary tract anatomy. Surgical treatment by means of cyst excision is done by incorporate partial hepatectomy.The prognosis for most patients with cysts of the extra hepatic bile duct, appropriately resected and reconstructed is excellent. Post-operative occurrence of stricture is about 3%[3].