-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(11): 2833-2835
doi:10.5923/j.ajmms.20241411.34
Received: Oct. 13, 2024; Accepted: Nov. 11, 2024; Published: Nov. 13, 2024

Expert Evaluation of the Duration of Intracranial Hematomas by Methemoglobin Concentration in Hot Climates
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLA. I. Iskandarov1, R. J. Zharimbetov2
1Doctor of Medical Sciences, Professor, Director of the Republican Scientific and Practical Center for Forensic Medical Examination of the Ministry of Health of the Republic of Uzbekistan, Tashkent City, Uzbekistan
2Director of the Karakalpak Branch of the Republican Scientific and Practical Center for Forensic Medical Examination of the Ministry of Healthof the Republic of Uzbekistan, Nukus City, Uzbekistan
Correspondence to: A. I. Iskandarov, Doctor of Medical Sciences, Professor, Director of the Republican Scientific and Practical Center for Forensic Medical Examination of the Ministry of Health of the Republic of Uzbekistan, Tashkent City, Uzbekistan.
| Email: |  |
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article provides data from our own research of 76 corpses of persons who died from traumatic brain injury at various times of the body's survival from 3 hours to several weeks. To determine the limitation period of head trauma, a spectro-photometric method was used to determine the concentration of methemoglobin in blood clots during subdural, epidural, and intracerebral hemorrhages мет. It was found that as the body's survival time increases, the concentration of methemoglobin increases.
Keywords: Spectrophotometry, Methemoglobin, Traumatic brain injury, Subdural, Epidural and subarachnoid hemorrhages
Cite this paper: A. I. Iskandarov, R. J. Zharimbetov, Expert Evaluation of the Duration of Intracranial Hematomas by Methemoglobin Concentration in Hot Climates, American Journal of Medicine and Medical Sciences, Vol. 14 No. 11, 2024, pp. 2833-2835. doi: 10.5923/j.ajmms.20241411.34.
Article Outline
1. Introduction
- Mechanical injuries occupy a leading place among injuries in peacetime. The largest share among them is made up of craniocerebral injuries (CCI), which differ in a variety of morphology and clinical forms, are severe and often fatal. Traumatic brain injuries are usually the result of serious crimes against the health and life of the individual. In such cases, the investigating authorities must determine the place and time of the injury, the properties of the traumatic object, the conditions of injury, the extent and nature of the damage caused to health, etc. All these and other issues are of a special nature and are resolved within the framework of a forensic medical examination. Hence, the relevance of studying some forensic aspects of CCI becomes clear, in particular, determining the statute of limitations for head trauma. Conducting forensic medical examinations to determine the time of causing CCI causes the most difficulties, since at present there are no clear and specific recommendations for determining the prescription of head trauma. In this paper, we attempted to determine the timing of intracranial hemorrhages in CCI by applying forensic-chemical studies of blood clotting to quantify the concentration of methemoglobin.Methemoglobin (MetHb) is a physiological component of blood, performs protective functions, neutralizing endogenously formed hydrocyanic acid, сероhydrogen sulfide and other poisons. MetHb is slowly formed in the blood, but its excess is constantly restored and the blood content remains at a low level (V. V. Avchinnikov, 1967).Data on the concentration of MetHb in the blood of healthy individuals are very contradictory. According to L. E. Gden (1968), MetHb is detected in the blood of healthy people in 23-25% of cases. But the average concentration in the blood does not exceed 3-5%. Moreover, women have a higher concentration than men. According to M. Kiese (1954), MetHb formed in red blood cells during life MetHbunder the action of enzymes contained in red blood cells is reduced to hemoglobin. It was found that the MetHb content increases as red blood cells age. This is due to a direct change in the hemoglobin molecules. An increase in MetHb in the blood is possible in a variety of pathological conditions.As the time elapsed after death increases, the content of MetHb in cadaveric blood increases (N. B. Cherkavsky, 1960, 1964). An increase in ambient temperature accelerates the spontaneous formation of MetHb in the blood of the deceased, as well as the reduction and decomposition of MetHb. Thus, the identification of postmortem biochemical patterns is of interest both for determining the time of death and for assessing the prescription of CCI by studying intracranial hematomas. At the same time, special emphasis was placed on the influence of temperature conditions in our Republic of Uzbekistan when studying this problem. The aim of the study was to quantify the concentration of MetHb in blood clots of intracranial hematomas in CCI patients.
2. Materials and Methods
- The material for the study was the results of spectrophotometric studies of intracranial hemorrhages in 76 corpses of individuals who died from severe CCI at various times after the injury. There were 58 men (76.3%) and 18 women (23.7%) who suffered from CCI, respectively. Most of the victims were between the ages of 30 and 40. Autopsies were performed no later than 24 hours after death.Death occurred at various times after receiving a CCI, so we divided all the material into 7 groups:Group 1-death occurred within 3 hours.Group 2-death before 12 o'clock.Group 3 –death within 24 hours.Group 4-death before 48 hours.Group 5-death before 60 hours.Group 6-death before 72 hours.Group 7-death occurred after 3 days from CCI. To determine the concentration of methemoglobin in blood clots (intracranial hematomas), a spectrophotometric method was used. Spectrophotometry is based on measuring the attenuation of monochromatic light flux as a result of selective absorption of light by a solute.In addition to quantitative spectrophotometry, qualitative spectrophotometry is widely used, i.e. identification of solutes by the shape of the light absorption coefficient or the so-called absorption spector. To determine methemoglobin in intracranial hematomas, we took subdural and epidural hematomas and blood from the dura mater sinuses (for control) into sections. The hematoma was ground in a glass homogenizer to a homogeneous liquid state to prepare hemolysate. We used the cyanide method developed by M. S. Kushakovsky (1980), which has a fairly high sensitivity and accuracy. It has the following advantages: it is simple and affordable; it can also be used when other hemoglobins are present in the blood solution in addition to oxyhemoglobin (HbO2) and methemoglobin (MetHb). the repeatability of the results is very high. The error of a single determination did not exceed 0.2-0.3% of MetHb (acid medium) in the spectral region when cyanite was added. MetHb is convertedto cyanomethemoglobin.The dependence of methemoglobin concentration on injury time was determined by univariate linear regression analysis.
3. Results and Their Discussions
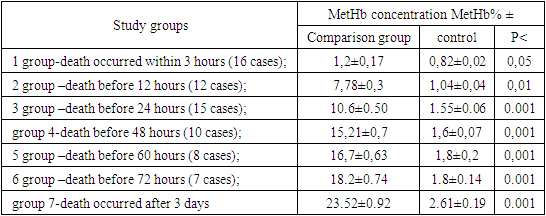
- The results of a spectrophotometric study obtained as a result of the difference in the concentration of MetHb from intracranial hemorrhages and the control group of blood from the upper sagittal sinus of the dura mater at different times of CCI were evaluated. The MetHb concentration was compared MetHbbetween the groups according to the 7 periods of post-traumatic hematoma development that we established. In the first group of victims who received CCI and died within 3 hours after the injury (16 cases), it was found that the concentration of MetHb in the studied hematomas ranged from 1.03-1.7, and the average value was 1.26-0.17%, compared with the control group (0.82±0.02) (P<0.05).In the second group (12 observations) of victims with a prescription for survival of the body after CCI up to 12 hours, the concentration of MetHb was 7.78±0.3% compared with the control group of 1.0±0.04% (P<0.01)In the third group (15 cases), where death after traumatic brain injury occurred within 24 hours, there was a noticeable increase in the concentration of MetHb to 10.6±0.80% compared to the control of 1.5±0.06% (P<0.01).In the fourth group (10 cases) of victims who received CCI with a survival period of up to 48 hours, the concentration of methemoglobin increased to 15.21±0.7% compared to the control group -1.6±0.07% (P<0.01).The fifth group of victims (8 cases) who received CCI and died after 2 days (up to 60 hours), the concentration of MetHb was 16.7+-0.63%. On average, compared with the control group -1.8±0.14% (P<0.01). In the sixth group (7 observations) of victims with a duration of experience after receiving CCI up to 3 days, the concentration of MetHb averaged 18.2±0.74% compared to the previous group..... - 1,8±0,14% (P<0.01).The seventh group (4 cases) of victims who received CCI and died in hospital after 3 or more daysMetHb , the average concentration of MetHb was 23.5±0.92% compared to the control group, where the concentration of MetHb was 2.61±0.19% (P<0.01).The generalized data of these studiesare presented in Table 1.
|
4. Conclusions
- 1. The immediate cause of death in craniocerebral injuries is the presence of intracranial hemorrhages, which lead to compression of the brain and disruption of vital body functions.2. As the survival time of the body increases after receiving a traumatic brain injury, the content of methemoglobin in the blood clots of intracranial hemorrhages increases. 3. The obtained spectrophotometric data can undoubtedly serve as an additional criterion for assessing the duration of a traumatic brain injury. 4. The spectrophotometric method for determining methemoglobin in blood coagulations in intracranial hemorrhages is the most promising method in the practice of forensic medicine.