-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2019; 9(3): 108-113
doi:10.5923/j.ajmms.20190903.08

Gender Association with Cardiopulmonary Resuscitation Skills in Hands-Only and Conventional CPR Training Techniques Programme
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAdedamola Olutoyin Onyeaso1, Chukwudi Ochi Onyeaso2
1Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Port Harcourt, Nigeria
2Department of Child Dental Health, Faculty of Dentistry College of Health Sciences, University of Port Harcourt / University of Port Harcourt Teaching Hospital, Port Harcourt, Nigeria
Correspondence to: Adedamola Olutoyin Onyeaso, Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Port Harcourt, Nigeria.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction: It is certain that the quality of bystander cardiopulmonary resuscitation (CPR) by the rescuer is crucial in the outcome of out-of-hospital cardiac arrest (OHCA) victims. The influence of gender on the quality of bystander CPR is still debatable. This study aimed at investigating the impact of gender on the quality of the bystander CPR practical skills in a group of Nigerian University students involving both the Hands-only and the Conventional CPR techniques. Material and Methods: A quasi-experimental study was conducted involving two cohort groups (Hands-only CPR and Conventional CPR) of 70 participants each who are undergraduate students in a Nigerian University. After the respective CPR trainings, each participant in each group was asked to carry out the CPR skills using manikins’ simulations of cardiac arrest scenario. They were all assessed by an American Heart Association (AHA)-certified instructor. The data was tested using both descriptive statistics and paired sample t-test and analysis of variance (ANOVA) with the statistical significance set at P < 0.05. Results: Both male and female participants had good CPR skills after their trainings. Neither male nor female gender showed any statistically significant association with any of the CPR skills (P > 0.05) within and between the CPR training groups. Conclusion/Recommendation: The gender of the participants did not show any statistically significant association with CPR skills. There is need for further related studies on factors that could influence the quality of bystander CPR by Nigerian lay rescuers.
Keywords: Gender, Association, Hands-only and Conventional bystander CPR, Nigeria
Cite this paper: Adedamola Olutoyin Onyeaso, Chukwudi Ochi Onyeaso, Gender Association with Cardiopulmonary Resuscitation Skills in Hands-Only and Conventional CPR Training Techniques Programme, American Journal of Medicine and Medical Sciences, Vol. 9 No. 3, 2019, pp. 108-113. doi: 10.5923/j.ajmms.20190903.08.
Article Outline
1. Introduction
- It is not uncertain that the quality of bystander cardiopulmonary resuscitation (CPR) is crucial in the outcome of such procedure in out-of-hospital cardiac arrest (OHCA) victims. However, there is still on-going research debate on the influence of gender factor on the overall quality of bystander cardiopulmonary resuscitation (CPR) based on different reports [1-6]. Meanwhile, poor quality bystander CPR can have far reaching negative impact on the victims [2, 3], and Amacher et al [3] found important gender differences [2, 3].The public health challenge of out-of-hospital cardiac arrest (OHCA) is in the increase globally [7-12]. Knowing that emergency situations needing bystander CPR do not have any respect for who is the bystander before it occurs, effective bystander becomes central in effective management of OHCA.Therefore, more information on this gender factor among laypersons is expected to guide the need or otherwise for any adjustment in CPR education and training of potential bystander CPR providers. Meanwhile, Sopka et al [13] reported superior external chest compression (ECC) skills among female participants in a female-only group in a gender-segregated CPR training groups where they had no distraction than in a combined (male and female) group.Hitherto, there are only few related reports from Nigeria [14-17]. Although the Nigerian Government has not done much in promoting the awareness and the need for bystander CPR services in the country, it is known that the public health challenge of OHCA is not limited to the developed economies of the world but equally affects the developing ones [7-12]. In fact, Dahan et al [7] has recently reported that victims of OHCA in low socio-economic status neighbourhoods were less likely to receive bystander CPR.In our attempt to provide more data on this subject, this study aimed at investigating the impact of gender on the quality of the bystander CPR practical skills in a group of Nigerian University students involving both the Hands-only and the Conventional CPR techniques. We hypothesised that: (1) there would be no statistically significant gender differences in the CPR skills acquired by the participants after the CPR trainings in the two separate groups; (2) there would be no statistically significant gender differences in the CPR skills acquired by the participants after the CPR trainings when the separate groups are compared; and (3) the male participants would not have statistically significantly better chest compression skill than their female counterparts.
2. Materials and Methods
- A quasi-experimental study was conducted involving two cohort groups (Hands-only CPR and Conventional CPR) of 70 participants each who are undergraduate students admitted in 2016 into the Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Nigeria. This study took place in March 2018. The researchers generated and tested the following null hypotheses: Ho1: There would be no statistically significant gender differences in the CPR skills acquired by the participants after the CPR trainings in the two separate groupsHo2: There would be no statistically significant gender differences in the CPR skills acquired by the participants after the CPR trainings when the separate groups are comparedHo3: The male participants would not have statistically significantly better chest compression skills than their female counterparts
2.1. Stage 1 (Pre-training)
- An assessment sheet, containing a section for the demographic data of the participants and a section having the four (4) CPR skills domains for the assessment of the skills for the conventional CPR group and three (3) domains for the hands-only CPR group, was used. The scenario of victims of cardiac arrest was simulated using the manikins and the participants were asked to carry out bystander CPR skills to show how they could help the victims. Their CPR skills were evaluated using modified AHA Evaluation Guide involving four components – (1) Scene Safety & Call for Help (SS), (2) Chest Compressions (CC), (3) Airway & Rescue Breaths (RB) and (4) Cycle / min & Placement of victim in the correct Recovery Position (RP) for the conventional CPR group while item 3 (Airway & Rescue Breaths) was excluded in the hands-only CPR group (Appendix). Their pre-training skills were understandably too poor and were left out in this report.
2.2. Stage 2 (Post-training)
- Teaching was carried out for 60 minutes using the American Heart Association (AHA) CPR Guideline which is available online. After the teaching on cardiopulmonary resuscitation (CPR) and practical trainings of the participants using the manikins for their hands-on sessions, each of them was asked again to carry out the CPR skills on the manikins unassisted as in the pre-training stage while the same principal researcher scored all of them in both the conventional and hands-only groups. The process of training them on hands-on and the re-assessment took another 4 hours.
2.3. Determination of Poor and Good CPR Skills
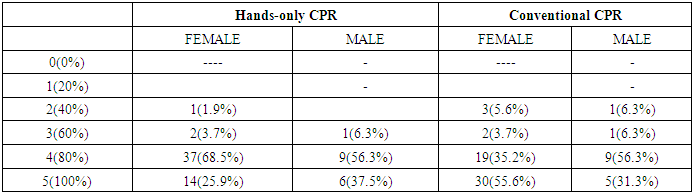
- None of the participants had received any form of CPR training before this study and they generally had very poor pre-training CPR knowledge and skills. Therefore, this report is based on their post-training CPR skills only. For each of the four (4) or three (3) domains of the CPR skills, 50% was considered acceptable and any score less than that was considered as poor CPR skills.
2.4. Statistical Analysis
- The data was collated and statistically analyzed using the Statistical Package for Social Sciences (SPSS). Descriptive statistics (frequencies, means) as well as the Paired T-tests and one-way ANOVA were used in the analysis with P-value set at 0.05.
3. Results
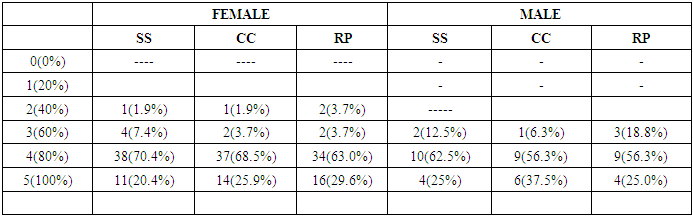
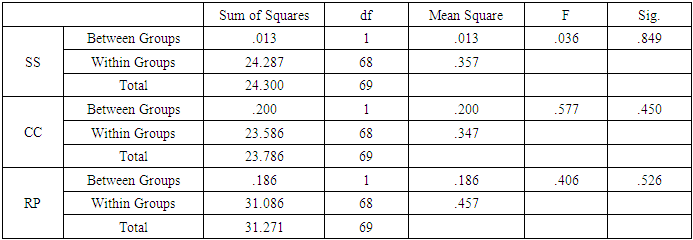
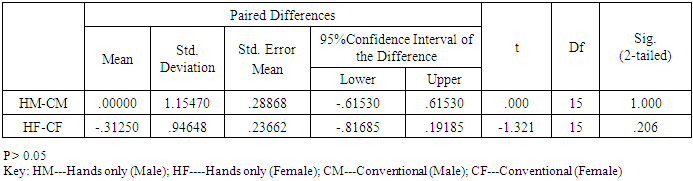
- Both groups (Hands-only CPR and Conventional CPR) had 54 (77.1%) females and 16 (22.9%) males each with the mean ages of 21.26 + 2.92 (SD) and 21.17 + 2.59 (SD) for Hands-only and Conventional CPR training groups, respectively.Participants and one-way analysis of variance (ANOVA), respectively. Tables 1a and 1b provide the descriptive data on gender and hands-only CPR post-training skills of the ANOVA shows no statistically significant difference in any of the CPR skills in relation to any gender (P > 0.05). This shows the acceptance of the first null hypothesis in relation to the hands-only CPR group.
|
|
|
|
|
|
|
4. Discussion
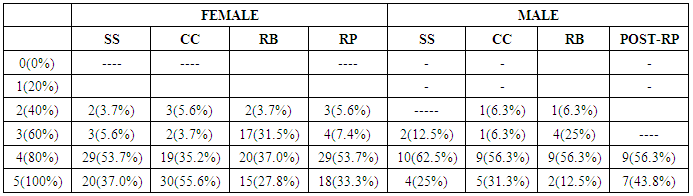
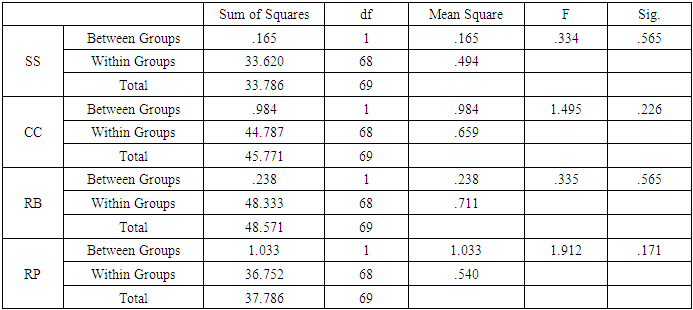
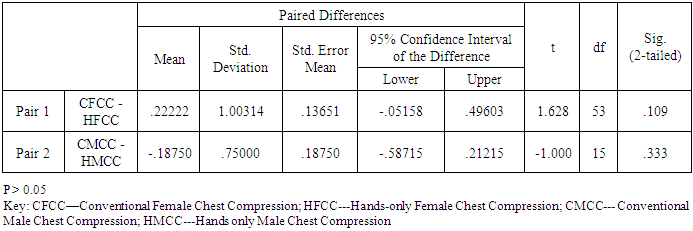
- This present Nigerian comparative study that assessed the association of gender with bystander cardiopulmonary resuscitation (CPR) skills in two CPR training techniques (Hands-only CPR and Conventional CPR) has neither revealed any statistically significant gender difference in relation to any of the CPR skills within each group nor between the groups. This means that no association was found between gender and CPR skills. Jaafar et al [1] reported no significant association between gender and the chest compression (CC) depth as well as between gender and ventilation while the females were only significantly faster than males in chest compression (CC). Meanwhile, Lopez-Gonalez et al [4] reported that the sex differences they noted during the CPR skill practice of their participants disappeared when controlling for age, body mass index (BMI) and cardio respiratory fitness. In conclusion, indicators of exertion during CPR are higher in women than in men, but these sex differences are because of BMI and differences in physical fitness conditions.The findings of the present study are consistent with earlier Nigerian studies [15, 17]. This means that for both secondary school students (younger population) and University students (the older Nigerian population) gender has not shown any statistically significant associations with the ability to carry out quality bystander cardiopulmonary resuscitation skills. In addition, it seems that even the CPR training method (whether the conventional or the hands-only) has not affected the ability of these Nigerian population to carry out CPR skills after training. Researchers at the University of Basel and University Hospital Basel did show that female resuscitation team performed cardiopulmonary resuscitation less efficiently than their male counterparts [3]. The female-only teams also showed less leadership communication compared with the male-only teams. According to the same report, even in mixed teams, women made significantly fewer clear leadership statements than men. The study suggested the need for action in the training of young female physicians because it was carried out among medical students [3].Our present Nigerian study did not have female-only or male-only teams but both sexes were combined during the training. Also, the report of Amacher et al [3] said that in comparison with male-only teams, the female groups showed less hands-on time and took longer overall to start the CPR, as well as the female-only teams showing less leadership communication compared with the male-only teams In addition, their study [3] reported that even in mixed teams, women made significantly fewer clear leadership statements. Meanwhile, this Nigerian study did not observe this as both the female and male gave similar clear communication skills. However, it must be noted that this Nigerian study did not have equal number of male and female participants. Concerning chest compression, our present study found no statistically significant difference in the sexes within the groups as well as between the participants in the two groups. According to Mpotos et al [18] and Odegaard et al [19], the quality of chest compression is paramount to sustain circulatory support and to restore heart beat and that this quality is influenced by rescuer’s fatigue and often associated with a poorer chest compression when CPR lasts for a longer period. In a study by Sopka et al [13], where some female and male participants were segregated outside the standard group having both sexes together involving participants of similar mean age with the present Nigerian study, it was shown that resuscitation training in gender-segregated groups has an effect on individual performance with superior external chest compression (ECC) skills in the female-only learning groups. They concluded that female participants could improve their skills by a more suitable learning environment, while male participants in the standard group felt less distracted by their peers than male participants in the male-only group. In a recent systematic review by Finke et al [20], female students demonstrated higher motivation to attend CPR-training, to respond to cardiac arrest, reach more people in the role of a multiplier and need to be individually addressed in intensified practical training. According to the study [20], male students achieve a more sufficient chest compression depth and higher CC-fraction and could benefit from individual motivation.Meanwhile, Rad and Rad [21] reported a significant relationship between the sex of the subjects and the number of performed compressions. Their results also showed that the majority of female nurses performed fewer effective compressions than their male counterparts. However, their study showed generally sufficiently deep compressions on the manikins like the participants in our present Nigerian study In the study by Russo et al [22], the rate of compressions provided by female subjects was faster but they were less strong compared to those provided by the male colleagues. In studies by Rad and Rad [21] and Russo et al [22] it was claimed that the female subjects were shorter in height, lighter in weight, and less strong in physique compared to the male counterparts. Our present Nigerian study did not assess the impact of the weight and height of the participants.For both genders, Tsegaye et al [23] reported that factors that contributed to the participants in the study practising CPR included lack of training, inadequate information, poor exposure, lack of confidence and lack of willingness. Strengths and Limitations of the StudyIn addition to having a study population with fair representation of Nigerian students based on the Admission Policy into Federal Universities in Nigeria, the assessment of the CPR skills of the participants was a very objective one which contributes to the reliability of the data.Also, this study has added information on the previous related studies mentions earlier because this study is the first ever from Nigeria to report on gender related CPR skills involving both hands-only CPR and the conventional CPR technique. However, the extrapolation of the results of this present study should be done with caution considering the fact that not all the 36 states in Nigeria were represented in the data.Also, this study did not have equal number of male and female participants which is anyway the true reflection of the male to female ratio in the entire class, and did not assess their heights and weights. More importantly, the present Nigerian study was done on manikins and not real patients.
5. Conclusions
- This Nigerian study has revealed no statistically significant association of gender with cardiopulmonary resuscitation (CPR) skills of the participants within and between both cohort groups.
6. Recommendations
- Further studies should be conducted in Nigeria to explore other factors including height and weight that could influence the provision of bystander CPR for victims of out-of-hospital cardiac arrest (OHCA) in preparation for the possible incorporation of bystander CPR training into the Nigerian schools curricula.