J. A. Olimov, F. I. Inoyatova, A. A. Abdukayumov, N. S. Nadjimutdinova, A. A. Musaev
Republican Specialized Scientific and Practical Medical Center of Pediatrics, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The aim of the study was to analyze in detail the causes of cochlear implantation complications, to determine the tactics of their elimination and the possibility of their prevention. Background. Cochlear implantation, as the only method of auditory and speech rehabilitation of patients with stage IV bilateral hearing loss or deafness, has existed for 40 years. One of the major complications is facial nerve palsy, which, according to literature, is relatively rare, ranging from 0.3% to 3.8%, according to various sources. Accordingly, the task of the surgeon performing this procedure is to maximally exclude postoperative complications and achieve a good result of auditory and speech rehabilitation. The authors describe three clinical case studies in this article. Conclusion. The incidence of iatrogenic impact on the facial nerve during cochlear implantation may be relatively high. This complication is facilitated by the presence of pathologic contents in the cells of the mastoid process and in the tympanic cavity. The presence of an inner ear anomaly with an atypical location of the facial nerve increases the risk of facial nerve injury during Cochlear implantation. However, detailed study of CT and MRI data and determination of surgical tactics taking into account all features of temporal bone structure can reduce the risk of postoperative complications.
Keywords:
Cochlear implantation, Facial nerve, Inner ear, Facial nerve palsy
Cite this paper: J. A. Olimov, F. I. Inoyatova, A. A. Abdukayumov, N. S. Nadjimutdinova, A. A. Musaev, Facial Nerve Injury as a Complication of Cochlear Implantation: Description of Three Clinical Cases, American Journal of Medicine and Medical Sciences, Vol. 15 No. 4, 2025, pp. 853-862. doi: 10.5923/j.ajmms.20251504.01.
1. Introduction
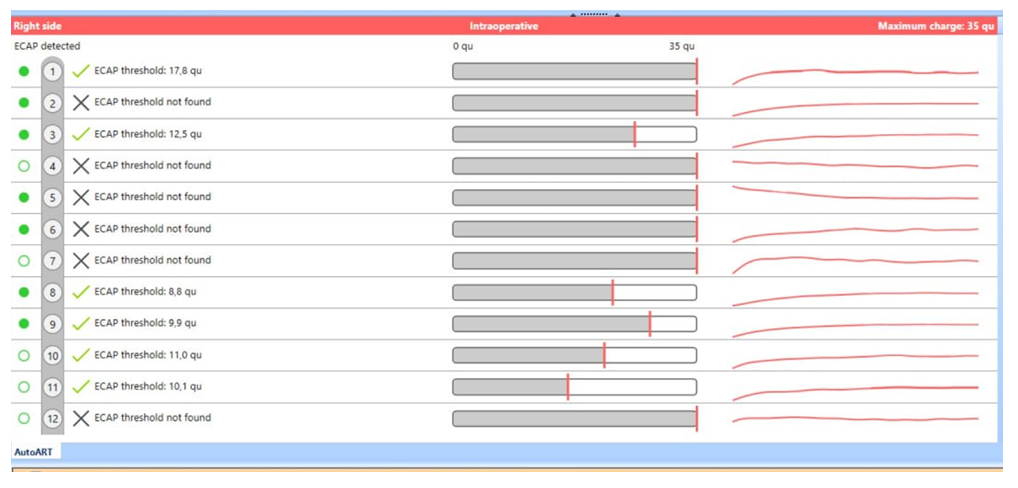
Cochlear implantation (CI), as the only method of auditory and speech rehabilitation of patients with stage IV bilateral hearing loss or deafness, has existed for 40 years. Currently, more than 324,000 Cochlear implantations have been performed worldwide [5]. However, with the undoubted advantage of restoring the ability to hear, CI, like other methods of medical rehabilitation, does not achieve the desired result in all cases. The complications that arise during its execution are largely responsible for this circumstance. Complications of CI vary within a fairly wide range according to different authors: 4,7%-40%. Causes of these complications are very different and are not clear in all cases, and moreover do not show a clear tendency to decrease [6]. Such a wide range of data scatter presented in the specialized literature on the subject under study indicates the absence of a unified classification and terminology. There is no doubt that to perform CI, especially with modernized surgical techniques, the operator is required to have serious training in otosurgery. It is explained by the fact that the surgical stage of CI combines the risks of complications associated both with any otiatric surgery and with its specificity - with the implantation of a foreign body in the peripheral part of the auditory analyzer. The probability of developing complications from CI depends on the complexity of the surgical procedure itself, the skill of the surgeon and his experience. Surgical injury caused during CI is iatrogenic and includes not only organ and tissue trauma, but also the consequences of the intervention and the severity of the postoperative period.It is important to know the risks associated with surgery, the peculiarities of the structure of the temporal bone and inner ear. Complications of CI are categorized into major and minor complications, often observed with anatomical anomalies of the middle and inner ear [7]. One of the major complications is facial nerve palsy, which, according to literature, is relatively rare, ranging from 0.3% to 3.8%, according to various sources [8-9]. Also, complications are directly related to the surgeon's skills and the hospital's clinical experience in performing cochlear implantation for various cases of anatomical anomaly, which are improved as experience is gained. In this case, the frequency of complications should be reduced or prevented intraoperatively.Accordingly, the goal of the surgeon performing CI is to maximize the exclusion of postoperative complications and a good result of auditory and speech rehabilitation.The methods for eliminating CI complications presented in the reviewed literature are largely descriptive in nature without detailing them and indicating the causes of these complications. There are no publications on the prevention of these complications.Thus, the lack of a tendency to reduce the number of CI complications, imperfect working classification, and the need to develop preventive measures at various stages of CI performance prompted a detailed analysis and description of three clinical cases of CI-related complications.The aim of the study was to analyze in detail the causes of cochlear implantation complications, to determine the tactics of their elimination and the possibility of their prevention. We present three clinical cases of facial nerve injury with palsy after cochlear implant surgery.Case 1: A 1.7-year-old child with a congenital bilateral anomaly of the inner ear, sensorineural hearing loss of the IV degree on both sides. Hearing thresholds according to Short-latency auditory evoked potentials (SAEPs)AD/AS - 85/90 dB. Magnetic resonance imaging and computed tomography (CT) revealed an anomaly of the inner ear - incomplete separation of the cochlea type I (IP I) on both sides. The operation was performed on the left side: a special electrode - compressed, 15 mm long - was installed. Intraoperative testing of the implant at telemetry showed the following: impedance was in the range of 5.66-9.23kOhm, auto-ART showed no nerve response, when the speech processor was connected no nerve response was revealed (Fig. 1, 2). 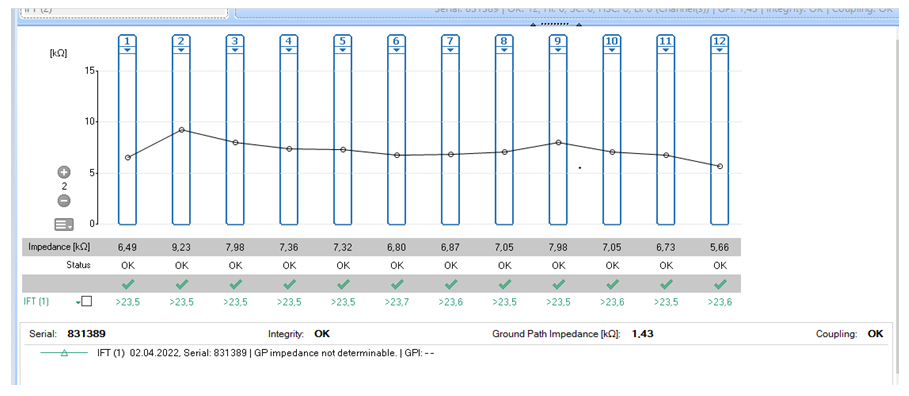 | Figure 1. Telemetry (Case 1: after surgery) |
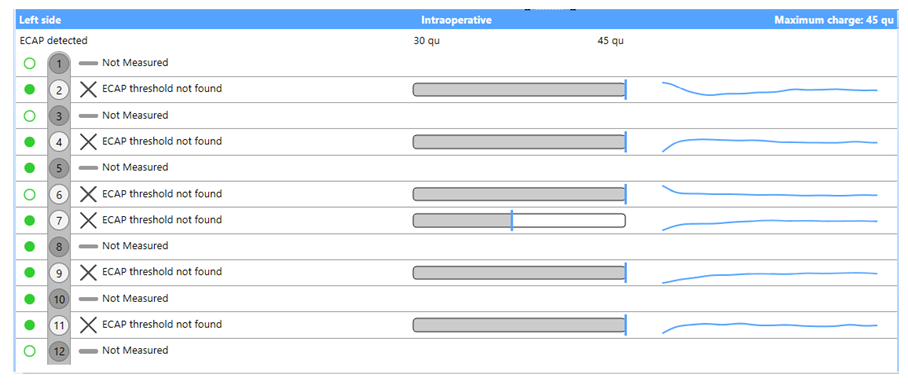 | Figure 2. Registration of auto-ART (Case 1: after surgery) |
Immediately after the surgery, the child had facial muscle dysfunction - facial nerve palsy on the left side: 5 points on the Yanagihara scale, grade V according to House-Brackmann. Postoperative temporal bone X-ray showed malpositioning of the electrode array in the cochlea. The electrode was located partially in both the antecubital region and in the projection of the apical part of the cochlea. The patient was conservatively treated with injectable prednisolone in gradually decreasing doses for 10 days. Examination after 2 months revealed that the signs of facial nerve palsy remained at the same level without positive dynamics (grade V according to House-Brackmann) (Photo 1). | Photo 1. Facial nerve palsy (case 1) after the first surgery |
Auto-ART dynamics revealed no nerve response at normal impedance. Due to the negative dynamics a computed tomography (CT) of temporal bones was performed and it showed that the electrode array passed through the canal of the facial nerve (in its tympanal segment) into the cavity of the vestibule of the inner ear, forming one turn (Fig. 3, 4).  | Figure 3. Implant electrode on the left side in the projection of the facial nerve canal (after the first surgery) |
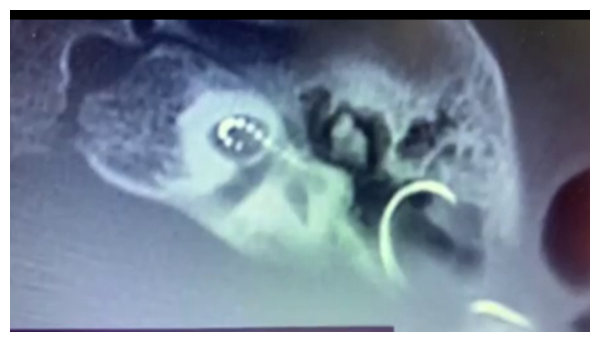 | Figure 4. Implant electrode on the left in the vestibule of the inner ear (after the first surgery) |
A repeated surgery was performed: revision showed facial nerve canal injury with its complete rupture and a defect of 0.7-1.0 cm of the implant electrode. Explantation and mobilization of the facial nerve with exposure from the bone canal from the knee to the level of the stylomastoid foramen was performed. Due to the large rupture of the nerve and the impossibility of matching its distal and proximal stump using the end-to-end anastomosis technique, its reconstruction was performed using an autograft of the sural nerve (suralis graft). A cochlear implantation was performed simultaneously in the right ear using a medium 24 mm electrode array; intraoperative testing of the implant (auto-ART monitoring) showed a neural response in 6 channels. CT scan revealed 2.5 turns of the electrode in the cochlea (Fig. 5). 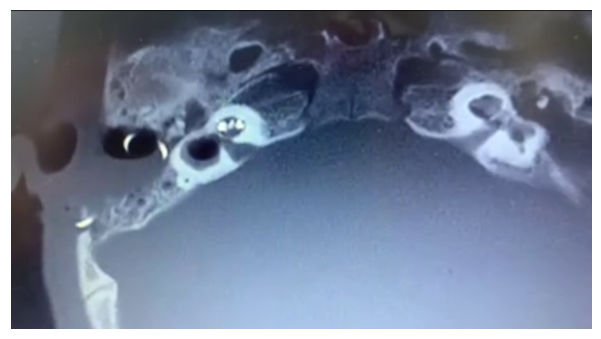 | Figure 5. The implant electrode on the right side is correctly positioned in 2.5 turns (after the second surgery) |
The postoperative period was uneventful. The function of the facial muscles on the right was normal, on the left 7 days after the operation according to the Yanagihara scale it was 8 points, grade V – according to House-Brackmann. One month after the operation, the patient was in a normal condition and the implant on the right was connected, when registering telemetry, the impedance was 5.23-8.46 kOhm; auto-ART: 6 channels were registered (Fig. 6, 7).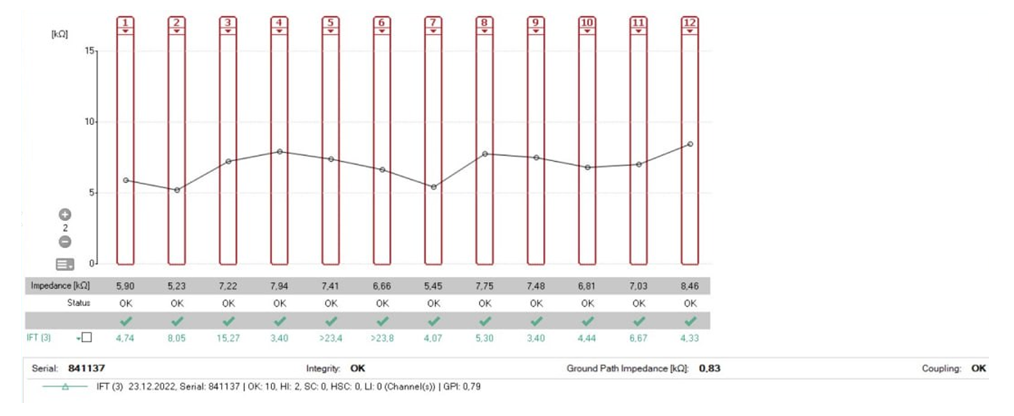 | Figure 6. Telemetry (Case 1: after the repeated surgery) |
 | Figure 7. Registration of auto-ART (Case1: after the repeated surgery) |
Positive dynamics of the mimic muscles function on the left side (improvement of facial muscle tone on the left side) was observed (Photo 2, 3).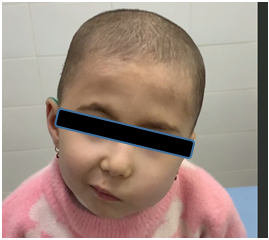 | Photo 2. Facial nerve palsy (case 1) 1 month after repeated surgery |
 | Photo 3. Facial nerve palsy (case 1) 1 month after repeated surgery |
Case 2: A 2.1-year-old child with congenital bilateral sensorineural hearing loss of grade IV on both sides. Hearing thresholds according to Short-latency auditory evoked potentials (SAEPs) AD/AS - 85/75 dB. Magnetic resonance imaging and computed tomography revealed the following: cochlea was of normal structure, presence of hyperplasia in the middle ear cavity. The surgery was performed on the right side: a standard electrode with a length of 31.2 mm was installed. Intraoperative features: high location of the facial nerve canal, granulations in the middle ear cavity, a cochleostomy was applied to install the electrode array. Intraoperative testing showed the following: telemetry - impedance between 4.92-7.55 kOhm, auto-ART revealed nerve response on 8 channels, channels 10-11-12 were out of the cochlea (Fig. 8, 9). 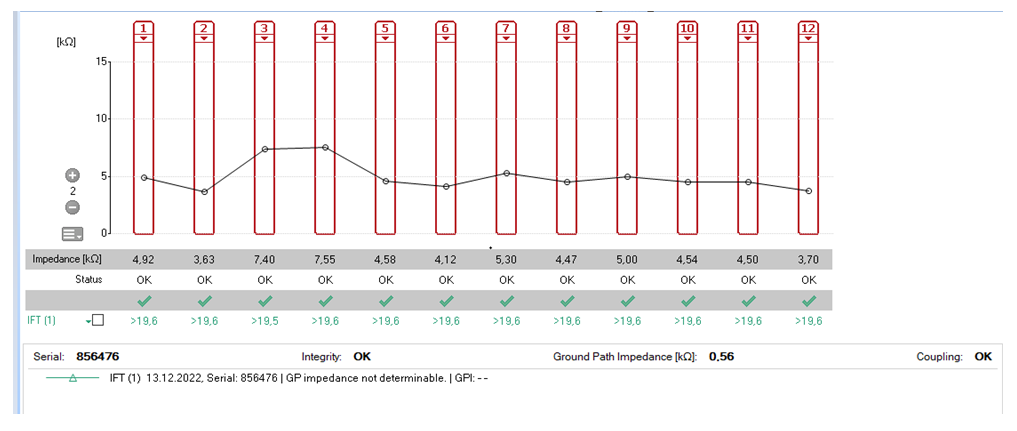 | Figure 8. Telemetry (Case 2: after the first surgery) |
 | Figure 9. Registration of auto-ART (Case 2: after the first surgery) |
Immediately after the surgery, the child had facial muscle dysfunction - facial nerve palsy on the left side: 0 points on the Yanagihara scale, grade VI according to House-Brackmann (Photo 4). | Photo 4. Case 2. Facial nerve palsy on the right side after the first surgery on day 5 |
Postoperative X-ray revealed 2 turns of the electrode in the cochlea, the electrode was partially outside the cochlea (Fig. 10).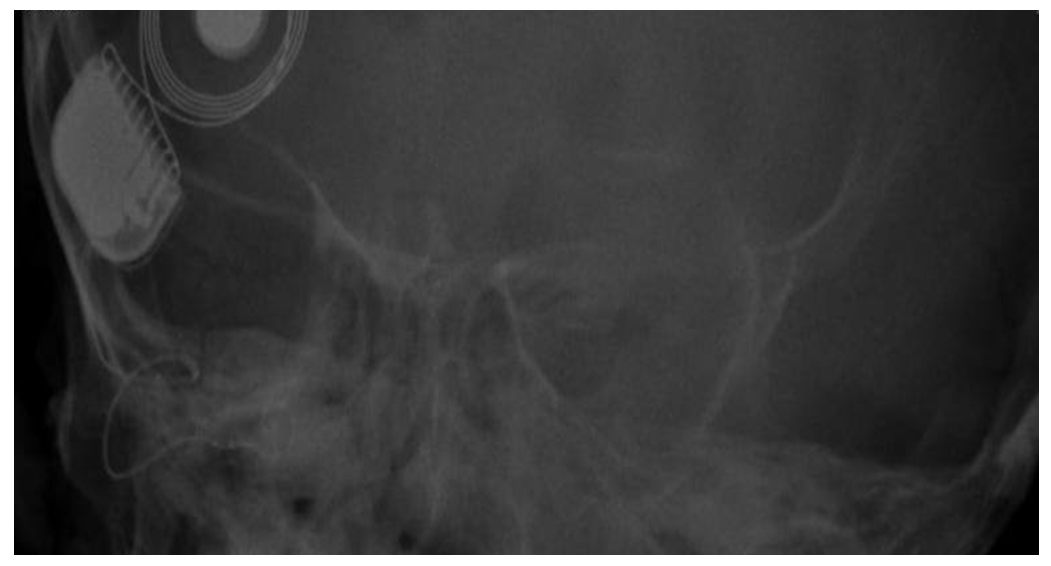 | Figure 10. X-ray of temporal bones - electrode array is visualized in the projection of the cochlea, partially - distal part outside the cochlea |
A repeated surgery was performed: revision showed injury of the facial nerve canal with its complete severance and a defect of 0.3 cm. The surgery - explantation, mobilization of the facial nerve with exposure from the bone canal from the second knee to the stylomastoid foramen was performed, the edges of the distal and proximal stumps of the nerve were matched, and its reconstruction was performed using the “end-to-end” technique. The facial nerve in the area of reconstruction was covered by the fascia of the temporal muscle with a flap of cartilage from the auricle. Reimplantation was performed on the right. Intraoperative testing with telemetry registered impedance of 3.33-5.08 kOhm; auto-ART monitoring revealed a neural response on 10 channels. 1 month after surgery, the patient was normal and the implant on the right was connected (Fig. 11, 12).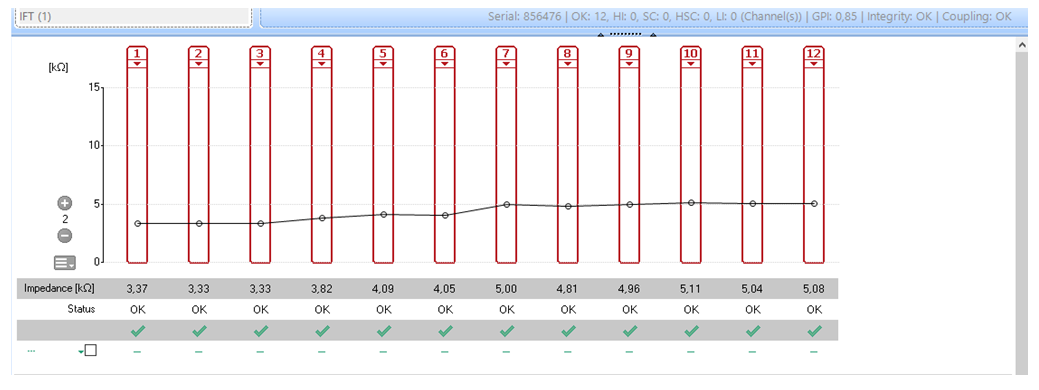 | Figure 11. Telemetry (Case 2 after the repeated surgery) |
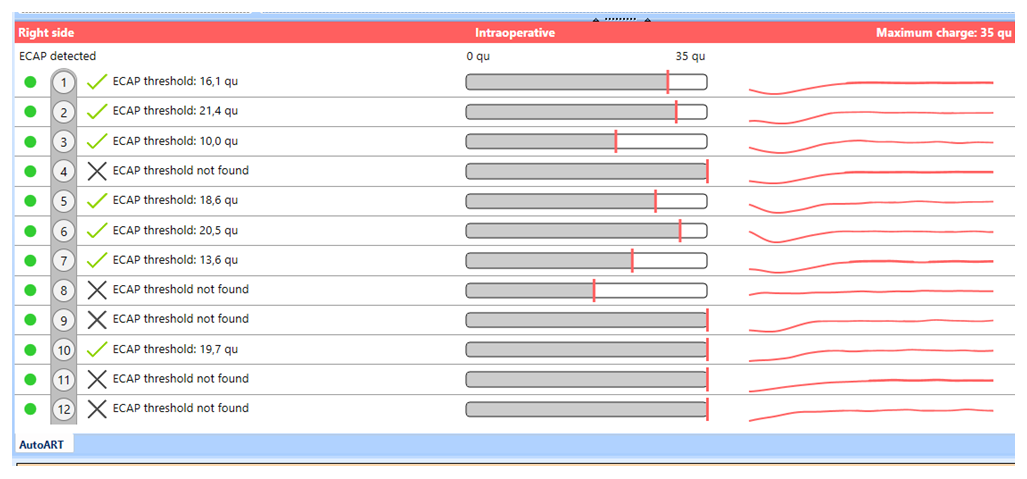 | Figure 12. Registration of auto-ART (Case 2 after the repeated surgery) |
CT scan revealed 2.5 turns of the electrode in the cochlea (Fig. 13). 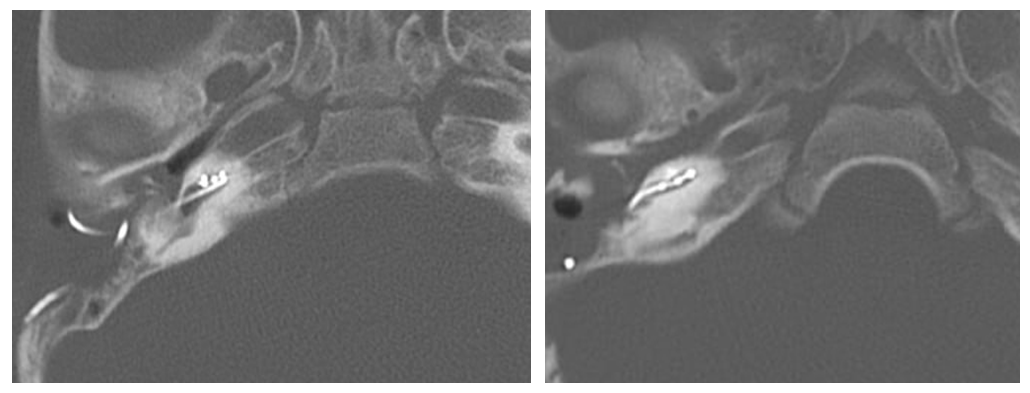 | Figure 13. The implant electrode on the right (after the repeated surgery) is correctly positioned 2.5 turns |
Postoperative diagnostics of facial nerve palsy after 7 days showed a Yanagihara scale score of 7, grade V - by House-Brackmann scale. Positive dynamics of the function of mimic muscles on the right side (improvement of facial muscle tone on the right side) was observed (Photo 5, 6). | Photo 5. Case 2: 1 month after repeated surgery |
 | Photo 6. Case 2: 6 months after repeated surgery |
Case 3: A 2.3-year-old child with congenital bilateral grade IV sensorineural hearing loss on both sides. Hearing thresholds according to Short-latency auditory evoked potentials (SAEPs) AD/AS - 85/85 dB. Magnetic resonance imaging and computed tomography data revealed the following: cochlea of normal structure, turned inward, high sinus location. The surgery was performed on the right side - intraoperatively there were difficulties with loss of landmarks and inability to determine the cochlear lumen with exposure of the carotid artery canal. Due to the impossibility of installing the implant on the right ear, the implant was placed on the opposite side (left): a standard electrode with a length of 31.2mm. Intraoperative features: high location of the facial nerve canal. Intraoperative testing with telemetry registered impedance of in the range of 3.39-8.82 kOhm, auto-ART revealed the presence of a nerve response on 9 channels (Fig. 14, 15). 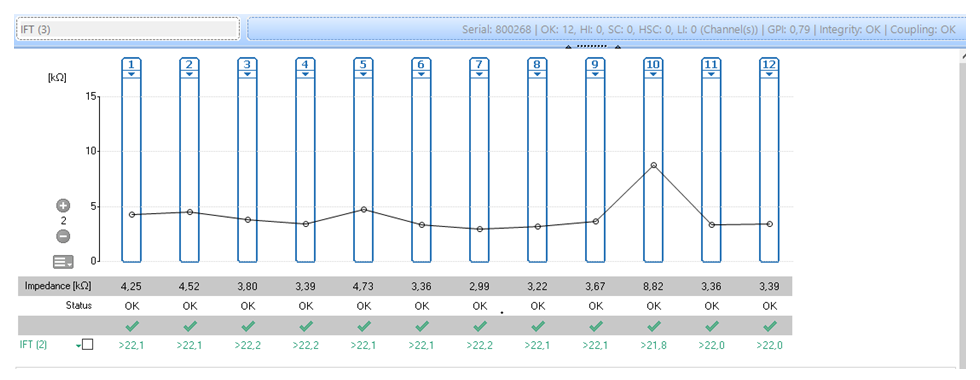 | Figure 14. Telemetry (Case 3: implant on the left) |
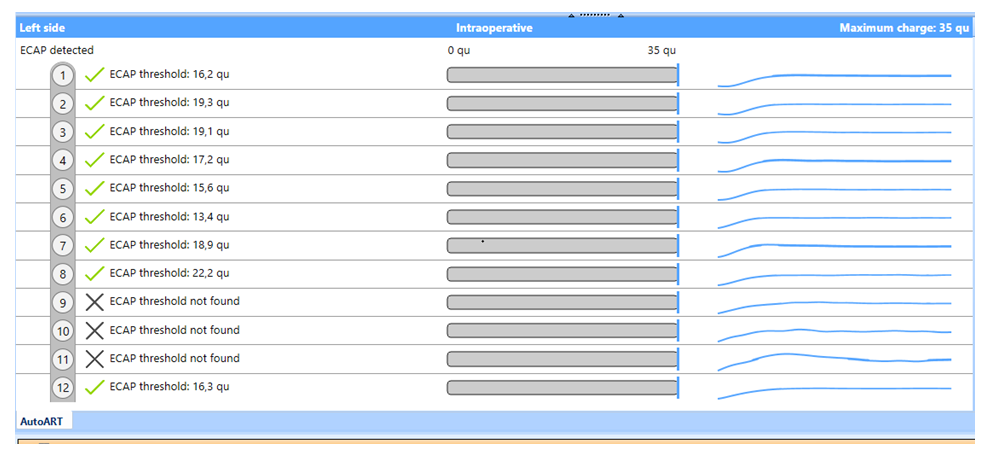 | Figure 15. Registration of auto-ART (Case 3: implant on the left) |
Postoperative computed tomography revealed 2.5 turns of the electrode in the cochlea on the left, a partially destroyed cochlea on the right, and a high location of the facial nerve canal.Immediately after the surgery, the child had facial muscle dysfunction - facial nerve palsy on the left side: 16 points on the Yanagihara scale, grade VI according to House-Brackmann scale. The patient underwent conservative treatment with injectable prednisolone in gradually decreasing doses for 10 days, and rehabilitation exercises for six months. Examination after 4 months revealed that the right facial nerve palsy persisted without improvement: on the Yanagihara scale - 22 points, grade V by House-Brackmann scale (Photo 7).  | Photo 7. Right facial nerve palsy (Case 3) 4 months after the first surgery |
Examination of the ear revealed on the right: perforation of the eardrum, development of purulent otitis media. Computer tomography revealed the presence of pathological contents in the middle ear cavity with the absence of part of the cochlea on the right, on the left – the correct placement of the implant with 2.5 turns of the electrode in the cochlea (Fig. 16). 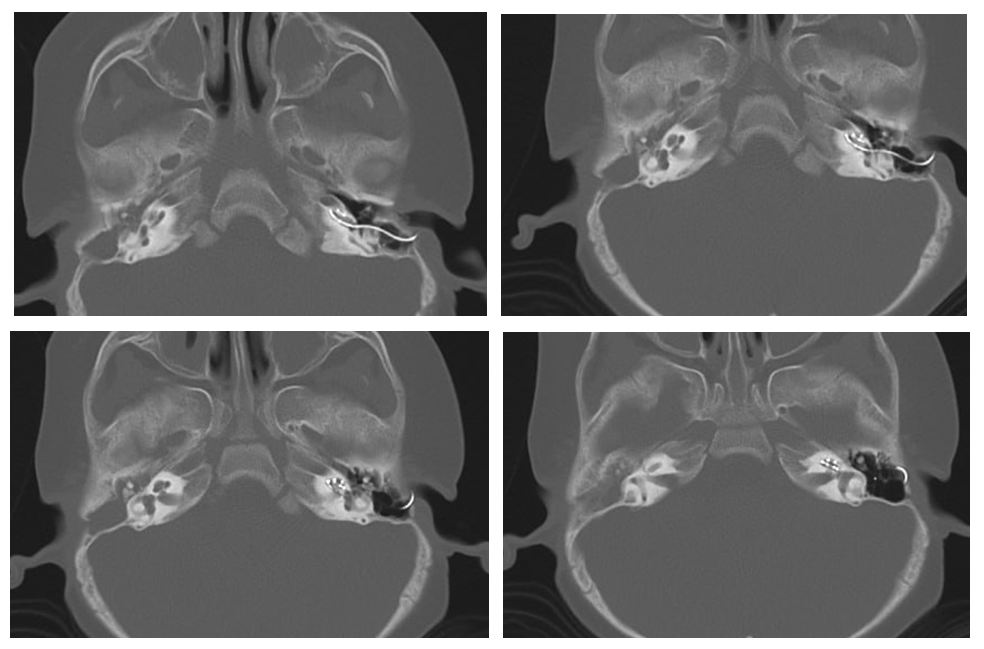 | Figure 16. CT-image of Case 3 after implantation on the left, on the right - revision of the cochlea |
A repeated surgery was performed on the right side - revision of the middle and inner ear. The following was observed intraoperatively: abundant granulation, in the tympanic region of the facial nerve canal a defect of the canal was determined through which a protrusion of the facial nerve was revealed with its partial injury and the formation of a neuroma of the facial nerve, exposure of the carotid artery canal was also revealed. The middle ear cavity was sanitized; the facial nerve was mobilized with release from the bone canal from the tympanic region to the mastoid region of the temporal bone with removal of the neuroma. The perforation of the eardrum is covered with flaps of cartilage of the auricle and periosteum of the temporal bone. 1 month after surgery the patient was in normal condition, in dynamics the function of mimic muscles on the right side has improved (improvement of facial muscle tone on the right side) (photo 8, 9). | Photo 8. Case 3: 1 month after the repeated surgery |
 | Photo 9. Case 3: 6 months after the repeated surgery |
2. Discussion
There are several known complications of cochlear implant surgery. The most disabling among the major complications is considered to be facial nerve palsy, which, however, is relatively rare. Iatrogenic facial nerve injury is one of the most dangerous complications of cochlear implantation. Intraoperative monitoring of the facial nerve is used during cochlear implantation as an additional method of prevention of its injury. In the absence of nerve monitoring, there is a theoretically higher risk of iatrogenic divergence of the fallopian canals with exposure of the facial nerve, especially in the area of its mastoid segment. However, according to Mandour MF et all. (2019) no additional risk of postoperative facial nerve palsy was found if the integrity of the neural membrane was preserved even in the absence of intraoperative monitoring. Moreover, the incidence of iatrogenic impact on the facial nerve was 0.73% when using intraoperative facial monitoring (p=0.99). In our cases, the damage was observed with a high level of otosurgical specialists: two specialists had experience in performing cochlear implants and operations on the middle and inner ear for more than 15 years. At the same time, we consider the presence of granulations in the cells of the mastoid process and in the tympanic cavity, increased bleeding during surgery to be contributing factors of such severe facial nerve injuries in the described cases. The most important factor, in our opinion, was the presence of a developmental anomaly of the inner ear with an atypical location of the facial nerve canal. In this case, the frequency during cochlear implantation can be relatively high. The frequency of iatrogenic effects with exposure of the facial nerve during CI was 46.58%. However, the incidence of postoperative facial nerve palsy was only 2.1%, and it decreased to 0.72% in cases without neural sheath injury. It was not significantly different from the 0.73% reported in the literature when intraoperative facial nerve monitoring was used (p=0,99). Different techniques of facial nerve reconstruction are used in case of significant defects. We applied a reconstruction technique when end-to-end matching was impossible using an autograft of the sural nerve (suralis graft). The sural nerve is a purely sensory nerve. Its main function is to provide sensation to the posterolateral surface of the distal third of the leg, the lateral surface of the foot, the heel and the ankle.
3. Conclusions
The incidence of iatrogenic effects on the facial nerve during cochlear implantation may be relatively high. This complication is facilitated by the presence of pathological contents in the cells of the mastoid process and in the tympanic cavity. The presence of an inner ear anomaly with atypical facial nerve location increases the risk of facial nerve injury when cochlear implantation is performed. However, a detailed study of CT and MRI data and determination of surgical tactics taking into account all features of temporal bone structure can reduce the risk of postoperative complications. Timely revision surgery using adequate technique of facial nerve reconstruction allows to obtain good results of its restoration.
Ethical Approval and Consent to Participate
The Research Ethics Board of our institution does not require review or approval of case reports. Our research was carried out in accordance with the World Medical Association Code of Ethics (Declaration of Helsinki).
Source of Funding
Each of the authors has reviewed and approved this manuscript. None of the authors has a conflict of interest, financial or otherwise. This manuscript is original, no part of it has been previously published and is not being considered for publication elsewhere. The corresponding author agrees to accept full responsibility for authorship at the submission and review stages of the manuscript.
Conflict of Interests’ Statement
The authors declare no conflict of interest.
ACKNOWLEDGEMENTS
The authors express their gratitude to the management of the Republican Specialized Scientific and Practical Medical Center of Pediatrics for the material provided for our study.
References
| [1] | Oguz Kadir Egilmez1 , M. Tayyar Kalcioglu2 1 COCHLEAR IMPLANT: INDICATIONS, CONTRAINDICATIONS AND COMPLICATIONS // Scripta Scientifica Medica, vol. 47, No 4, 2015, pp. 9-16 doi: https://journals.mu-varna.bg/index.php/ssm/article/view/1428/1460. |
| [2] | Brito R., Monteiro T. A. , Leal A. F., Tsuji R. K., Pinna M. H., Bento R. F. Surgical complications in 550 consecutive cochlear implantation // Brazilian Journ. of Otorhinolaryngology. 2012. N 78(3). P. 80–85. |
| [3] | Bhatia K, Gibbin KP, Nikolopoulos TP, O’Donoghue. Surgical complications and their management in a series of 300 consecutive pediatric cochlear implantations Otology & Neurotology 25(5): p 730-739, September 2004. |
| [4] | Jonas Jeppesen, Christian Emil Faber, 2013. Surgical complications following cochlear implantation in adults based on a proposed reporting consensus. Pages 1012-1021 | Received 16 Mar 2013, Accepted 05 Apr 2013, Published online: 14 Jun 2013. Acta Oto-Laryngologica. |
| [5] | Elfeky, A.E.M., Tantawy, A.A., Ibrahim, A.M. et al., 2021 Complications of cochlear implantation surgery in Zagazig University Hospitals. The Egyptian Journal of Otolaryngology volume 37, Article number: 71. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML