-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2023; 13(9): 1190-1194
doi:10.5923/j.ajmms.20231309.02
Received: Aug. 13, 2023; Accepted: Sep. 1, 2023; Published: Sep. 12, 2023

The Efficiency of Using "Moisture air" in the Treatment of Deep Burn of the Hand and Fingers
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLXakimov Erkin Abduxalilovich1, Daminov Feruz Asatullaevich1, Nekbaev Xasan Sayfulloevich2, Xayitov Laziz Milionerovich1, 2
1Samarkand State Medical University, Uzbekistan
2Samarkand Branch of the Republican Scientific Center for Emergency Medicine, Uzbekistan
Correspondence to: Xakimov Erkin Abduxalilovich, Samarkand State Medical University, Uzbekistan.
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

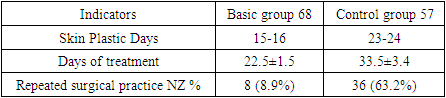
Introduction. Evaluation of the effectiveness of the humid-air environment and dermazin ointment in the treatment of deep burns of the palms and fingers and early skin autodermoplasty. Purpose. Evaluation of the effectiveness of the moist-air environment in the treatment of deep burns of the palms and fingers and early skin autodermoplasty. Materials and Styles. In 2020-2022, 125 patients who were treated with deep burns of the palms and fingers were divided into 2 groups and the results of treatment were studied in the combustiology department of the Samarkand branch of the Republican Scientific Center for Emergency Medicine. 68 (54.4%) patients of the main group were treated with humid-air environment. 57 (46.6%) patients in the control group were treated with traditional methods of treatment. The age of the patients ranged from 7 months to 73 years, the average age was 23±3.0 years. Results. With deep burns of the palms and fingers of the main group, treated with a moist-air environment, due to unfavorable conditions for the survival and reproduction of microorganisms in the burn wound, the regeneration process is accelerated, the recovery period of the skin layer is delayed, and the treatment is delayed. days decreased to 10-12 days. In patients of the control group, the granulation process proceeded slowly, postoperative complications (keloid scars, contractures, pigmentary changes) amounted to 63.2%. There was a decrease in these complications to 8.9% in those treated in the main group. Conclusion. In the treatment of deep burns of the palms and fingers, the use of a “moist-air environment” is highly effective. This method of treatment not only allows for early plastic surgery of the skin and accelerates the granulation process, accelerates wound healing, but also reduces complications. after skin plastic surgery by 2.5 times, and treatment days are 10-12 days, the use of argan also led to a decrease in pain and negative emotions during daily dressing and wound care.
Keywords: Deep burns of the palms and fingers, Humid environment, Autodermoplasty
Cite this paper: Xakimov Erkin Abduxalilovich, Daminov Feruz Asatullaevich, Nekbaev Xasan Sayfulloevich, Xayitov Laziz Milionerovich, The Efficiency of Using "Moisture air" in the Treatment of Deep Burn of the Hand and Fingers, American Journal of Medicine and Medical Sciences, Vol. 13 No. 9, 2023, pp. 1190-1194. doi: 10.5923/j.ajmms.20231309.02.
Article Outline
1. Introduction
- At present, it is important to rely on high technologies in the treatment and diagnosis of diseases, the use of modern equipment, early detection of diseases, low cost and short days of patient recovery [1].But it can be noted that the problems of some pathologies have not lost their relevance. Cases of deep burns of the palms and fingers, post-burn complications (contractures, keloid scars, pigmentary changes, impaired aesthetics of the palm and fingers) account for 35% of burn injuries. Among children, this figure is higher [2].55% of burns in young children occur mainly on the palm and fingers. These burn injuries are mainly caused by the use of household heating equipment, hot water containers (thermoses), as well as the use of sandals to heat the house during the winter months in mountainous areas, including sandals that cause deep burns to the feet, hands, head and face [3].30% burns of the feet, 30% of the palms and fingers, 35-40% of the head and face due to falling on sandals. Sandalwood burns are always characterized by deep skin burns. This means that the coals from sandalwood fire have a high temperature of 400 to 800 degrees [4].In the elderly, in many cases, burns of the palms and fingers are observed, mainly from open flames and hot bodies [5].The treatment of deep burns of the palms and fingers remains one of the urgent problems of modern combustiology. The healing process of a burn injury is long, deforming contractures of the palm and fingers occur in 25-50% of cases [6,7].The healing period of deep burns of the palms and fingers is 1-1.5 months. During this period, a thick black scab appears on the wound, and during the inflammatory period, the wound is purulent. The effectiveness of the humid-air environment in deep burn wounds lies in the fact that it is important to maintain the permeability of the vessels that feed the skin at the bottom of the wound [8,9,10].During the cleaning of the wound, granulations appear in the wound after necrotomy, necrotomy in surgical practice. After that, a free skin graft (autodermoplasty) is performed surgically. Humidity of the air is explained by the fact that the separation of necrotic tissues is painless, and bleeding from the wound during surgery is not observed [11].
2. Objective
- To evaluate the effectiveness of the "humid-air environment" in the treatment of deep burns of the palms and fingers and early skin autodermoplasty.
3. Materials and Methods
- In 2020-2022, 125 patients who were treated with deep burns of the hands and fingers were divided into 2 groups and the results of treatment were studied in the Combustology department of the Samarkand branch of the Republican Scientific Center for Emergency Medicine. In the treatment of 68 (54.4%) patients of the main group, a “moist-air environment” was used, a schematic representation of which is shown in Fig. 1.
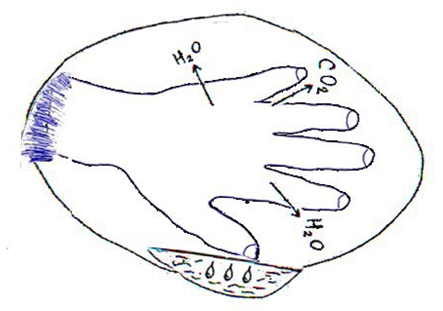 | Figure 1. Schematic representation of the humid-air (greenhouse) environment |
 | Figure 2. Creating a "moist air environment" |
 | Figure 3. Exposure to the "humid-air environment" on the first day after the burn injury |
 | Figure 4. Jarohat granulation_14th day |
 | Figure 5. Free skin grafting (autodermoplasty) |
 | Figure 6. Free skin grafting (autodermoplasty) inner surface of the palm |
 | Figure 7. Free skin grafting (autodermoplasty) on the outer surface of the palm |
 | Figure 8. After surgery 3rd day |
4. Results
- In the main group, a "humid-air environment" was created by wearing an aseptic dressing with betadine on the wounds of the palms and fingers of the treated patients from the first hour. After a certain time, a dark yellowish exudative fluid began to stand out. During the day, 500-1000 ml of fluid was released from the wound in elderly patients. Dry necrosis in the wound was prevented in the “moist-air environment”, and tissue blood supply was prevented by deepening the wound. At the same time, patients practically did not complain about pain in the wound.The bandage on the wound was opened once a day. The dressing change was painless due to the "moist atmosphere" and the dressing was easily separated from the wound. On the 2nd day thick yellowish fibrins appeared on the wound. Fibrins adhered to the dressing and separated with each dressing change. Painless excision of necrotic skin tissues was performed with light movements at each dressing change. The fluid released from the wound decreased by 10-15% per day, became darker and thicker. Biochemical analysis of the obtained liquid exudate content of total protein decreased from 55 g/l to 25-30 g/l after 6-7 days. In addition, potassium-sodium-chlorine electrolytes were found in the liquid.Electrolytes showed 3-4 times less than in the blood test. Thus, the "moist-air environment" applied to the treated patients of the main group caused the appearance of granulations in the wound on the 10-15th day, contributed to the cleansing of the wound in a short time, and in patients of the main group, skin grafting was performed on the 16-17th day. This amounted to treatment days of patients of the main group 22.5±1.5 days. Patients in the control group were treated for 32.5±3.4 days.
 | Figure 9. 18-day status before discharge |
 | Figure 10. Result 1 month after surgery |
 | Figure 11. Contracture II degree in a treated patient in the control group |
 | Figure 12. III degree contracture in a treated patient in the control group |
|
5. Conclusions
- The results of these studies and analysis show that the use of "humid-air environment" is highly effective in the treatment of deep burns of the palms and fingers, and this method of treatment not only allows for early surgical skin grafting, but also reduces its duration, but also accelerates wound healing, has a positive effect on reducing complications after the procedure. It also causes a decrease in pain and negative emotions during daily dressing and treatment of wounds, which occupies a special place in the practice of treating burn patients.
Conflict of Interest
- The authors declare no conflicts of interest or special funding for the current study.