-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2023; 13(9): 1187-1189
doi:10.5923/j.ajmms.20231309.01
Received: Aug. 9, 2023; Accepted: Aug. 30, 2023; Published: Sep. 12, 2023

Features of Gender Differences in Patients with Migraine
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBahtigul Holmuratova, Nilufar Rashidova, Gulnora Rakhmatullayeva, Khanifa Khalimova, Dilshoda Akramova
Department of Neurology and Medical Psychology, Tashkent Medical Academy, Uzbekistan
Correspondence to: Bahtigul Holmuratova, Department of Neurology and Medical Psychology, Tashkent Medical Academy, Uzbekistan.
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

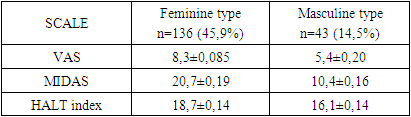
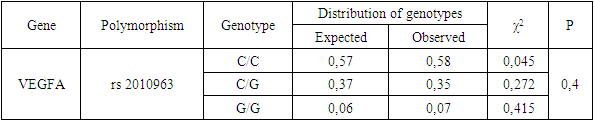
Background: Among the primary headaches migraine is the most common. The clinical symptoms of this disease are different between men and women. In this difference, the gender characteristics of the male and female are very important. This review aims to determine gender differences among migraine patients. Methods: 178 patients with migraine were registered using visual analogue (VAS) scale, MIDAS scale and HALT index. A molecular genetic study was also carried out with the study of the C634G gene of VEGF. Gender types of patients were identified by Sandra Bem’s schema. Results: The intensity of headaches according to the VAS in patients with the feminine type was 8,3 ± 0,085, patients with the masculine type experienced slightly less intense pain – 5,4 ± 0,20. Evaluation of the daily activity of patients with migraine according to the MIDAS revealed intense headaches in patients with the feminine type, which highly disrupted the daily activity of patients - 20,7 ± 0,19. The average score for the HALT index in patients with the feminine type was 18,7±0,14. For the C634G polymorphism of the VEGF gene, the distribution of actual genotypes in the group of patients and the control sample corresponded to that expected at RCM equilibrium (p>0,05). Conclusion: The presence of the unfavorable 634G allele of the VEGF gene in the genotype contributes to more frequent detection of the feminine type. The highest scores of MIDAS are observed in patients with the feminine type.
Keywords: Migraine, Headaches, Gender, Gene, Attack, Primary headache, Features, Pain, Patients, Feminine, Masculine
Cite this paper: Bahtigul Holmuratova, Nilufar Rashidova, Gulnora Rakhmatullayeva, Khanifa Khalimova, Dilshoda Akramova, Features of Gender Differences in Patients with Migraine, American Journal of Medicine and Medical Sciences, Vol. 13 No. 9, 2023, pp. 1187-1189. doi: 10.5923/j.ajmms.20231309.01.
1. Introduction
- Currently, gender differences in patients with migraine (M) are relevant [1]. At the same time, the term "gender" is usually used to refer to such personality characteristics as masculinity (“masculinity”) and femininity (“femininity”), due to the influences of the socio-cultural environment, i.e. stereotypes, ideas existing in society about which personal qualities (psycho-behavioral pattern) correspond to the male and which female [2,4,5]. Consequently, people are committed to traditional gender roles to varying degrees [3]. Differences between men and women in certain reactions, including responses to pain stimulation, are largely due not only to the biological characteristics of men and women, but also to different degrees of severity of masculinity and femininity in them. It has been shown that persons with low femininity and masculinity are more common in different types of primary headaches [7,8]. In addition, migraine patients are more common in women (both men and women). However, despite certain attempts to study the influence of sex and gender differences on the characteristics of headache, many questions remain unanswered, since the identification of gender characteristics allows us to refine the prognosis of migraine headaches [9,10].
2. Methods
- 179 patients with migraine (M) were examined. We prospectively enrolled consecutive patients diagnosed with M and diagnosis was based on the ICHD-3 [1]. All examined patients underwent clinical and neurological examination, including scales: the visual analogue VAS scale, the quality of life of patients with migraine using the MIDAS scale, and the calculation of days lost due to headache using the HALT scale. A molecular genetic study was also carried out with the study of the C634G gene of VEGF.
3. Results
- The results of calculating the intensity of headache according to the VAS scale and the associated decrease in the quality of life of patients according to the MIDAS scale, and the days lost due to headache according to the HALT index showed in Table 1.
|
|
|
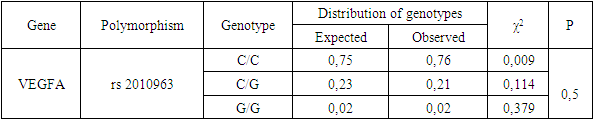
 , which indicates a moderate genetic diversity of this polymorphism.In the population sample, hexp and hobs corresponded to the values of 0.23 and 0.21, which corresponds to the low gene diversity of the population for this polymorphism.In the main and control samples, the coefficient of the relative deviation of the observed heterozygosity from the expected C634G polymorphism of the VEGFA gene turned out to be negative, i.e. D<0 (D=-0.05 and -0.04, respectively), which indicates a lack of heterozygotes, the level of which corresponds to moderate (Table 4).
, which indicates a moderate genetic diversity of this polymorphism.In the population sample, hexp and hobs corresponded to the values of 0.23 and 0.21, which corresponds to the low gene diversity of the population for this polymorphism.In the main and control samples, the coefficient of the relative deviation of the observed heterozygosity from the expected C634G polymorphism of the VEGFA gene turned out to be negative, i.e. D<0 (D=-0.05 and -0.04, respectively), which indicates a lack of heterozygotes, the level of which corresponds to moderate (Table 4).
|

4. Discussion
- In this article, the gender types of migraine were studied. Particularly the effect of gender has been studied and has been found to be of considerable value in the clinical course of migraine. The feminine type plays a central role here, but it is assumed that this is only part of the mechanism. Some therapeutic strategies have been developed based on this knowledge. However, there is currently no evidence to support gender-specific treatment strategies for migraine. There are some limitations to be considered. This study was clinic-based and the data cannot estimate the prevalence of M in the general population. The findings require further study and cannot be extrapolated to the general population directly.
5. Conclusions
- Thus, the presence of the unfavorable 634G allele of the VEGF gene in the genotype contributes to more frequent detection of the feminine type. At the same time, the highest scores in patients with migraine according to the MIDAS are observed in patients with the feminine type, therefore, the higher the scores of the HALT index, which indicates severe impairments in the quality of life of the examined patients, requiring medical treatment.