-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2016; 6(1A): 19-24
doi:10.5923/s.sports.201601.04

Heath-Related Physical Fitness in School Children and Adolescents
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLFlávio Roberto Pelicer1, Kazuo Kawano Nagamine1, Marco Antonio Faria1, Vinicius de Lima Freitas1, Cassiano Merussi Neiva2, Dalton Müller Pessôa Filho2, Emmanuel Gomes Ciolac2, Carlos Eduardo Lopes Verardi2
1College of Medicine of São José do Rio Preto (FAMERP), Brazil
2Department of Physical Education, College of Sciences, Bauru Campus, São Paulo State University (UNESP), Brazil
Correspondence to: Carlos Eduardo Lopes Verardi, Department of Physical Education, College of Sciences, Bauru Campus, São Paulo State University (UNESP), Brazil.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Physical inactivity and obesity has shown to increase in children and adolescents in the past decades. Thus, to analyze physical activity levels in school children and adolescents is crucial for implementing health promotion programs. Our aims was to analyze the health-related physical fitness in school children and adolescents, and to compare according to chronologic age, gender and reference values. 648 school children and adolescents aged 7 to 16 years performed the PROESP-BR physical fitness testing battery, which includes measures of anthropometry (height, body mass and estimate of body fat percentage), flexibility (sit and reach test), cardiorespiratory fitness (9 min walking/running test), and muscle endurance and strength (1 min push up test). The average health-related physical fitness were lower than the PROESP-BR healthy normative levels for children and adolescents of all ages. Girls showed lower levels of cardiorespiratory fitness, and muscle endurance and strength than boys (P < 0.05). However, flexibility was lower in boys than girls (P < 0.05). Girls also showed higher percentage of body fat than boys (P < 0.05). School children and adolescents showed low levels of health-related physical fitness, whereas girls showed lower levels than boys. This results suggests that interventions programs focused in improving health-related physical fitness are welcome in this population.
Keywords: Adolescents, Anthropometry, Cardiorespiratory Fitness, Children, Flexibility, Muscle Endurance and Strength
Cite this paper: Flávio Roberto Pelicer, Kazuo Kawano Nagamine, Marco Antonio Faria, Vinicius de Lima Freitas, Cassiano Merussi Neiva, Dalton Müller Pessôa Filho, Emmanuel Gomes Ciolac, Carlos Eduardo Lopes Verardi, Heath-Related Physical Fitness in School Children and Adolescents, International Journal of Sports Science, Vol. 6 No. 1A, 2016, pp. 19-24. doi: 10.5923/s.sports.201601.04.
Article Outline
1. Introduction
- The increasing of industrialization and the progress of people social-economic status that occurred in the last decades modified the feeding behavior patterns worldwide, which contributed to alarming overweight and obesity levels [1]. In 2008, more than 1.4 billion of adults were overweighed, and 11% of them were obese. In 2012, more than 40 million of children below 5 years old were overweighed worldwide [2]. From 1980 to 2013, the prevalence of overweight and obesity increased 27.5% and 47.1% in adults and children, respectively [3]. In developing countries, the prevalence of overweight and obesity in children increased from 8.1% and 8.4% (1980) to 12.9% and 13.4% (2013) in boys and girls, respectively [3]. It is important to note that no country worldwide reported reduction in the overweight or obesity prevalence during this period [3].The obesity epidemic has shown to be associated with increased levels of calorie intake, lower levels of daily living physical activity and sedentary life style [4]. The reduction of physical activity levels and the increased sedentary life style are associated with the increasing time spent using computers and watching television [5], which results in reduced health-related physical fitness, higher risk for cardiometabolic diseases (i.e.: hypertension and type 2 diabetes) [5]. Psychosocial problems such as depression, low self-esteem, and decreased cognitive function and academic performance are also associated with a sedentary life style [6]. To assess the physical inactivity prevalence and the health-related physical fitness in school children and adolescents are necessary to develop programs focused in promoting a healthy life style, including the regular practice of physical activity and the improvement of dietary habits as important strategies to counteract overweight/obesity and its associated diseases [7]. The benefits of a higher levels of health-related physical fitness include a lower incidence of risk factors for chronic diseases, reduced central and total body fat, improved physical and mental health, and increased academic performance [8]. Thus, the health-related physical fitness assessment may help to identify possible risks for health problems, by comparing with normative values.The purpose of present study was a) to analyze the health-related physical fitness of school children and adolescents, comparing the results by age and gender, and b) to classify their health-related physical fitness performance according to the PROESP-BR normative values.
2. Methods
2.1. Population and Study Design
- The present research is a cross-sectional study that investigated 648 children and adolescents (328 boys), aged 7 to 16 years (11 ± 2.6 years old), students of public and private schools (2nd to 9th elementary school grade) from José Bonifácio – SP, Brazil. The children and adolescents had their health-related physical fitness evaluated with the PROESP-BR physical fitness testing battery, which includes measures of anthropometry (height, body mass and estimate of body fat percentage), flexibility (sit and reach test), cardiorespiratory fitness (9 min walking/running test), and muscle endurance and strength (1 min push up test). The results were compared between gender and among age groups, as well as classified according to the normative values. The present research was approved by the Ethical Committee of the São José do Rio Preto Medical School (protocol nº 5799/2010). The legal guardians of children and adolescents read a detailed description of the protocol and provided their written informed consent prior to study participation.The PROESP-BR health-related physical fitness testing battery [9] was used to assess children and adolescents performance. The PROESP-BR is a nationwide observatory of growth, motor development and nutritional status indicators in 7 to 17 years old Brazilians. Its aim is to describe, monitor and analyze the behavior of body growth, physical fitness, nutritional status and lifestyle of school age Brazilians [9]. The children and adolescents included in the study had their anthropometry, flexibility, cardiorespiratory fitness, and muscle endurance and strength assessed by a trained exercise science professional, and all tests were performed in the same day. The assessment started by the height (0.1 cm precision) and body mass (0.1 kg precision) measurement in an electronic scale with stadiometer (Filizola Inc., Brazil) with the subjects without shoes and wearing minimal clothes. Body mass index (BMI) was than calculated by the weight (Kg) divided by the squared height (m)2 and classified according to the PROESP-BR normative values [9]. Tricipital and subscapularis skinfolds were then measured (Cescorf skinfold caliper) in triplicate in the right side, and the average of the three measures was calculated. The body fat percentage was estimated using the equation proposed by Boileau, Lohman and Slaughter [10] and classified according to the normative values proposed by Deurenberg, Pieters and Hautuast [11]. The participants then had the flexibility assessed with the sit and reach test, which was performed in triplicate, being registered the higher value reached. The testing battery continued with muscular endurance and strength assessment, which was performed by the 1 min push-up test, being registered the number of push-ups preformed in 1 min. Finally, the cardiorespiratory fitness was performed around the sports field of the respective schools, with the measures defined and marked with cones, where students ran and / or walked for 9 min, and with the distance covered being register in meters.
2.2. Statistical Analyzes
- Data are presented as absolute and frequencies, percentages, mean ± standard deviation and/or median (interquartile ranges). The Kolmogorov-Smirnov test was performed to ensure a Gaussian distribution of the data. The data with non-parametric distribution was compared between groups by the test U of Mann-Whitney. The data with parametric distribution was compared between groups by the non-paired Student’s t test. The significance was set at P < 0.05. The software Graph Pad Instat 3.0 and Prisma 6.01 were used for statistical analyzes.
3. Results
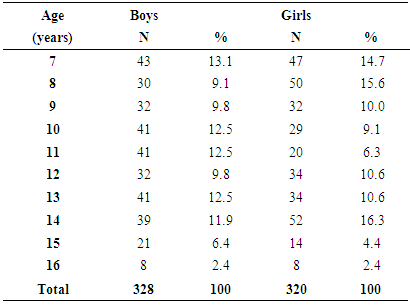
- The age and gender distribution of the population studied are presented in Table 1.
|
|
|
|
4. Discussion
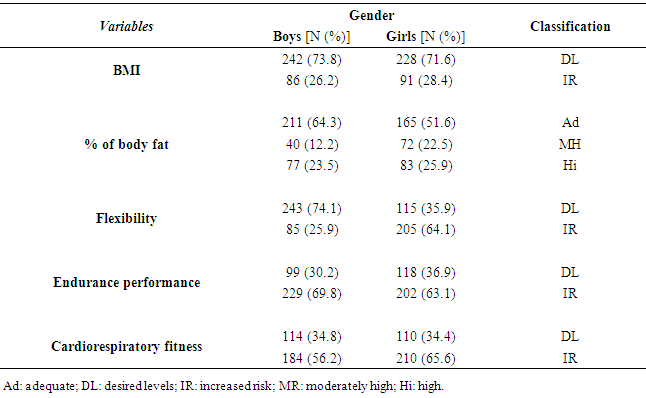
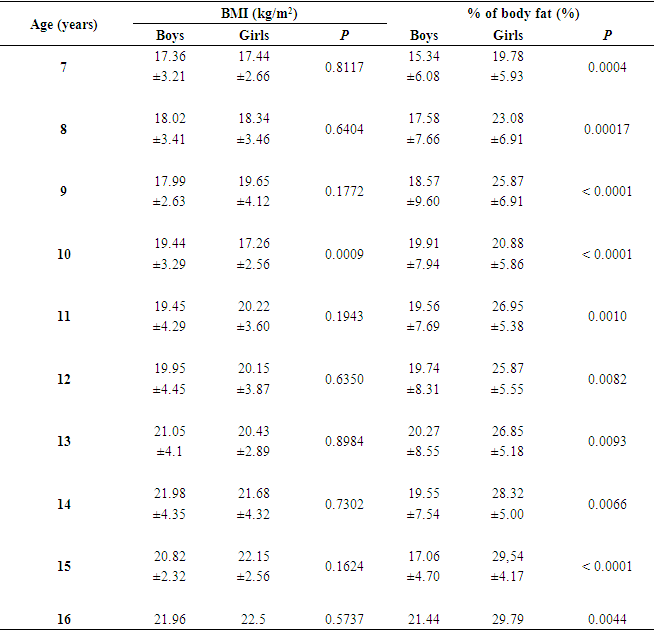
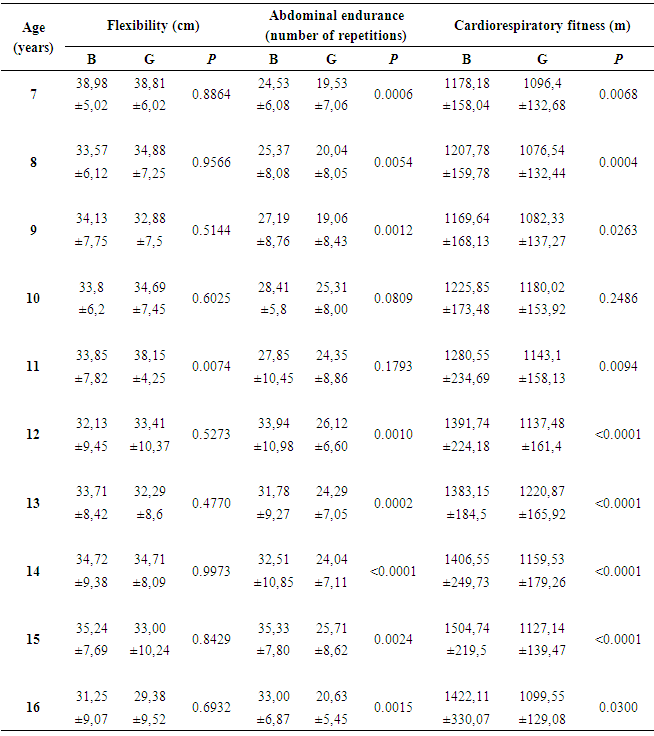
- The health-related benefits of healthy dietary behaviors and increased physical activity levels for children and adolescents has been previously shown [7]. Studies analyzing the health-related physical fitness in children and adolescents may give important information for adopting public policies focused in promoting healthy habits as the physical exercise practice. In this context, the study of health levels in a specific population, focused in primary prevention and health promotion, should look at biological and social variables that are presented. The aim of the present study was to analyze and compare the health related physical fitness in girls and boys aged 7 to 16 years, as well as to classify them according to the normative values of the PROESP-BR health-related physical fitness testing battery [9], which has shown satisfactory results the Brazilian school age population [12]. The results showed that 26.2% of boys and 28.4% of girls were overweight or obese according to their BMI, which can be associated to social and behavior factors. Similar founds were found in percentage of body fat that also showed moderately high levels in boys (35.5%) and girls (48.4%) [13]. The increased prevalence of overweight in children and adolescents should be treated from a public health perspective [13]. Girls aged > 5 or 6 years have body fat levels higher than boys [14]. In this context, a healthy percentage of body fat should be between 10.01% to 20% in boys, and 15.01% to 25% in girls [11]. Boys with body fat levels higher than 25% and girls with body fat levels higher than 35% are at high risk for cardiovascular risk factors [15]. Body fat levels higher than 30% and 35% for boys and girls, respectively, are the cutoff point for obesity [15]. The higher body fat levels in girls is due to a higher adipocyte diameter, mainly after the 11th year of life (16). Since that body fat represents an additional weight that should be carried during weight bearing activities, the higher body fat reduces the performance to weight bearing physical activities in girls when compared to boys [16]. Although the flexibility was not significantly different between girls and boys of almost all ages (excepted for the higher flexibility found in girls aged 11 years), the boys presented higher flexibility levels than girls, according to the PROESP-BR normative values [9]. These results are against the results of a previous study showing higher flexibility levels in girls of almost ages when compared to boys [17]. Low flexibility levels in children and adolescents are associated to low back pain and postural deviation, as well as higher back pain complaints in adulthood [18]. Although girls generally has higher flexibility levels than boys mainly during adolescence growth and sexual maturation [14], it was not found in the present study. Moreover, the present results showed that the flexibility of girls appears to decrease with the advance of age (Table 4). Since that the physical activity levels of girls are generally lower than boys [19], the higher levels of inadequate flexibility according to normative values found in girls than boys may be attributed, at least in part, for this reduced physical activity pattern. However, future results should better investigate this hypothesis. The muscle endurance performance was at healthy levels only in 7 to 9 years old boys, and in 7 and 8 years old girls. Almost all girls aged 9 to 16 years and boys aged 10 to 16 years had their muscle endurance performance classified as high risk according to the PROESP-BR normative values [9]. Since that reduced muscle endurance may result in joint and postural disorders, as well as in higher incidence of musculoskeletal injury [20], the results of present study may have important implications. When compared between genders, boys showed higher muscle endurance performance than girls in almost all ages (exception for the 10th and 11th year of life), which is accordance with the results of previous studies [7, 19]. Since that an optimal growth and development of musculoskeletal system occurs when tension with progressive workload are given to the musculoskeletal system [21], a resistance exercise program supervised by an exercise specialist, using equipments adequate to the children/adolescent height, and with a progressive workload increase may be suggested for the present population. The reduced cardiorespiratory fitness found in boys and girls of all ages groups in the present study are in accordance with results of previous studies [7, 17]. In the present study, only boys aged 8 to 10 years and girls aged 7 to 10 years showed healthy cardiorespiratory fitness levels. This finding is alarming, because low cardiorespiratory fitness levels are associated to increased risk for developing cardiovascular and metabolic diseases [22]. To obtain the healthy benefits of exercise, it is suggested to participate in conditioning program containing aerobic and resistance exercises [23]. In this context, the schools have an important role in promoting physical activity in children and adolescents, specially by the physical education classes. The students were also generally involved in physical activity during the class break, as well as walking or riding a bike to go to and come back from the school. However, there is an alarming increase in physical inactivity as we advance in the 21th century. In this context, to counteract this sedentary scenario, the schools should review its role on children /adolescents' health, increasing the opportunity of performing physical activities, and increasing the students awareness about benefits of regular practice of physical activity [24]. Parents and friends also have a social influence on the physical activity practice of children and adolescents, whereas physically actives are the model and offer a greater social support. The higher is the social support by parents and friends, the higher is the physical activity levels of children and adolescents. In this context, interventions for increasing physical activity compliance should stimulate the parents' and friends' participations, especially in adolescents, to facilitate and create opportunities for joint physical activities practices [25]. These programs should also be performed in public health policies, by increasing the participation of exercise specialists and physical education professionals.The limitations of the present study includes the lack biological maturation status of subjects analyzed. Its cross-sectional design is also a limitation because it does not allow identify causality among the variables. Besides the limitations, the present study suggests the implementation of health programs that promotes the regular practice of physical exercise and sports by children and adolescents.
5. Conclusions
- The present results showed that a high percentage of children and adolescents have reduced health-related physical fitness. These results suggests the implementation of public policies to promote the regular practice of physical activity and, consequently, to increase the physical fitness and to reduce the risk for developing diseases. Moreover, since girls appears to have lower health-related fitness than boys, future researches are necessary to identify biological and behavioral factors that may affect the low performance found in girls.