-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2014; 4(6A): 49-55
doi:10.5923/s.sports.201401.07
The Epidemiology of UK University Football Injuries within the 2011-2012 Season
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLDaniel Marr1, Simon Coleman1, Carla Mccabe2
1Institute of Sport, Physical Education and Health Sciences, University of Edinburgh, Edinburgh, United Kingdom
2Ulster Sports Academy, University of Ulster, Jordanstown, United Kingdom
Correspondence to: Carla Mccabe, Ulster Sports Academy, University of Ulster, Jordanstown, United Kingdom.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Although football is one of the most popular sports worldwide, there have been very few studies on injuries suffered at university level. The aim of this study was to collate a wide range of epidemiological findings representative of the injuries suffered by those who play football at this level; while also comparing those injuries suffered between males and females. An electronic retrospective questionnaire was completed by 183 British University level footballers (males n=99, females n=84) who had sustained an injury during the 2011-12 season. The dominant lower limb (ankle: 29.5%, knee: 19.7%) was found as the most common site of injury occurrence with sprains (36. 6%) and muscle strains (23%) reported as the most common types of injury. University players are most often exposed to risk of injury in the autumnal period (20%), whilst playing a competitive match (58.5%) on a grass surface (66.1%) and the severity of injury is high (44.8%). Males reported more groin/thigh and muscle strain injuries compared to females. This study provides a landscape of information in relation to UK university football injuries. There is a need for an injury surveillance initiative to be implemented prospectively involving team doctors and a database of players’ medical records. This, in combination with the results found in this study, will help produce a better evidence base of the epidemiology of injuries at this level which will pave the way for producing preventative strategies that aim to improve the safety of university football participation.
Keywords: Football, Injury, Epidemiology, University
Cite this paper: Daniel Marr, Simon Coleman, Carla Mccabe, The Epidemiology of UK University Football Injuries within the 2011-2012 Season, International Journal of Sports Science, Vol. 4 No. 6A, 2014, pp. 49-55. doi: 10.5923/s.sports.201401.07.
Article Outline
1. Introduction
- Football is one of the most popular global sports with evidence suggesting that approximately 4% of the population (270 million people) participate within the sport, either in a playing or refereeing capacity [1]. During the period 2000-2006 participation within the registered men’s game increased by 21% at both senior and youth level to 34.2 million, while women’s participation increased by 54% to 4.1 million [1]. Because football is associated with high levels of injury [2-6], it is important to understand the epidemiology of football injuries concomitant with the growth of participation so to minimise and ultimately prevent injury risks where possible. Van Mechelen, Hlobil and Kemper [7] suggested that there are 4 key stages in sports injury prevention: 1) collect information regarding the injuries; 2) identify the variables likely to increase injury occurrence; 3) introduce a preventative strategy and 4) evaluate the effectiveness/ usefulness of the preventative strategy. Research groups including the FIFA Medical Assessment and Research Centre (F-MARC), the English Football Association (FA) and the Oslo Sports Rehabilitation Centre [8] have all used this method to assess the incidence of injuries in football, with the aim of reducing injuries and improving the safety of the sport. Epidemiological studies are an effective method of measuring injury rates and reviewing the factors that influence injury – hence addressing Van Mechelen et al.’s [7] first 2 key stages of injury prevention as detailed previously. The majority of epidemiological studies in relation to football injuries have investigated male elite players [2-4, 6, 9-11], male youth team players [5, 12-14], female senior players [15] and female youth players [16]. These studies have provided a landscape of knowledge in relation to the injury characteristics associated with the aforementioned populations. Within a local demography, the governing body for university sport within the United Kingdom (UK) ‘British University and Colleges Sports’ (BUCS) reported within its most recent annual review [17] that participation in university sport is expanding each year, with one in every four students taking part in regular physical activity. Of the 4712 BUCS sports teams, the highest participation is in football consisting of 153 institutions (457 male teams; 157 female teams), with hockey reported to be the second most popular sport consisting of 130 institutions (267 male teams; 273 female teams). However injury characteristics associated with UK university football is currently lacking. Therefore as university football participation increases, it is important to identify the factors associated with injury so that an evidence based approach can be developed to enhance injury awareness and introduce preventative strategies as detailed by Van Mechelen et al. [7].This study aims to examine a range of epidemiological injury characteristics associated with UK university football participation including male and female players during the 2011-2012 football season. Such information will be useful for players and coaches in terms of providing an insight into the injury risks associated with UK university football and as a consequence, play a fundamental role in shaping future preventive strategies in order to maintain healthy participation.
2. Methods
- The BUCS website was referenced to acquire the names of all football teams currently involved in the BUCS leagues, of which 801 university football teams were identified (606 male & 195 female teams) [17]. Thereafter an independent database was created containing contact details for each football team with the aim to voluntarily recruit university football players who had previously sustained an injury within the 2011-2012 season. In doing so, skill level or gender was not restricted in order to obtain a broad representation of university football injury rates across all levels of participation.An online retrospective injury questionnaire (surveymonkey.com, California, Palo Alto, USA) [18] was distributed electronically to each football team during the period December 2012-February 2013. The internet was used to distribute the questionnaire due to its higher response rate compared to more traditional paper based methods of data collection [19], thereby increasing the potential sample size and power of the study. Moreover Facebook was also used to promote completion of the questionnaire as it is regarded the most popular social network site used by British students [20].As previously mentioned, only players who had sustained an injury during the 2011-12 football season were required to complete the survey. The definition of sustaining an injury for the purposes of this study was one which forced the player off the football field during a match, or caused them to stop/miss training. Absence through illness or injuries sustained outside football participation was not included [2, 5]. If players were injured more than once throughout the 2011-2012 season, they were asked to answer the questionnaire based solely on their most recent injury in order to reduce the impact of recall bias [21] and thus complete the retrospective questionnaire more accurately. Ethical approval was obtained from the University Ethics Committee.
2.1. Survey Content
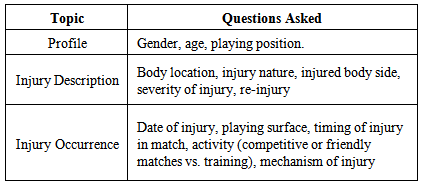
- Development of the survey was based on previous injury questionnaires detailed in the literature [2, 5, 22]. In particular, Hawkins and Fuller’s [2] questionnaire measuring injury incidence in professional and youth football which contains a mixture of open and closed questions and has been proven to obtain a high response rate in the past was adapted within the current study (Table 1). Moreover, after conducting pilot work the survey content was modified to provide the participant with various clearly defined options per question in order to avoid injury misdiagnosis.
|
2.2. Data Collection & Analysis
- The questionnaire was distributed to each football team using an URL link and where possible to each team’s Facebook page. Prior to completing the questionnaire, participants were required to accept the ‘tick box’ statement which was used to confirm their voluntary consent and that each participant was over 16 years old as suggested by the University Ethics Committee. Four weeks after the questionnaire was distributed, an electronic reminder was sent to clubs in order to maximise the response rate. Following two months of data collection, the responses were filtered, coded and exported to IBM Statistical Package for Social Sciences (SPSS, version 21) for further analysis. All data were non-parametric, nominal and arranged into categories by frequency counts. Pearson’s chi-squared (X2) one sample and cross tabulation tests were used to determine statistical significance (p<0.05) [23]. Comparisons were made using cross-tabulation methods and the expected frequencies were adjusted accordingly.
3. Results
3.1. Profile
- 329 previously injured participants responded to the questionnaire, with some excluded due to completing the survey inadequately and reporting injuries in the wrong time-frame. A total of 183 responses were available for analysis, which included 99 male injuries (54%) and 84 female injuries (46%) from 51 different university institutions. 99.5% of respondents were between 18-25 years old.It was found that playing position had a significant effect on injury rate (p<0.001) with defenders identified as the most commonly injured footballers (38.8%) followed by midfielders (37.7%), strikers (20.8%) and goalkeepers (7.7%). There was no significant difference found between males and females relating to playing position.
3.2. Injury Description
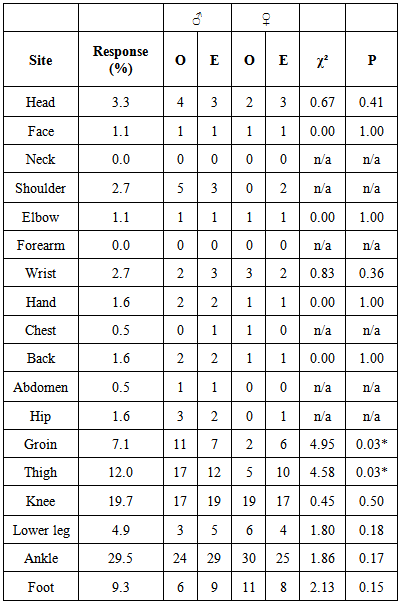
- Body location was identified as a significant factor effecting injury rate (p<0.001). Specifically it was found that the ankle joint (29.5%), knee joint (19.7%) and the thigh (12.0%) incurred more injuries than all other body locations (Table 2). Moreover it found that males reported significantly more groin (p=0.03) and thigh (p=0.03) injuries compared to females (Table 2).
|
|
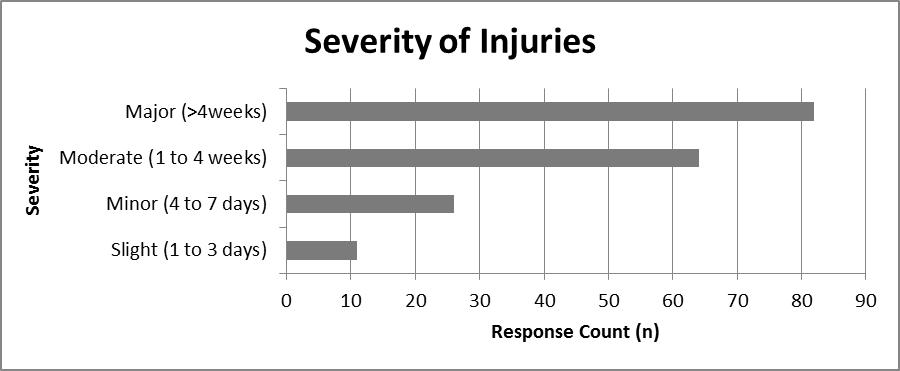 | Figure 1. Severity of injury incurred for university football players during the 2011-2012 season |
3.3. Injury Occurrence
- The month which players sustained an injury had a significant effect on injury rate (p<0.001). Figure 2 illustrates that most injuries occurred in October (20.2%) followed by November (18%) and September (10.5%). Gender had no significant effect on when players sustained an injury.
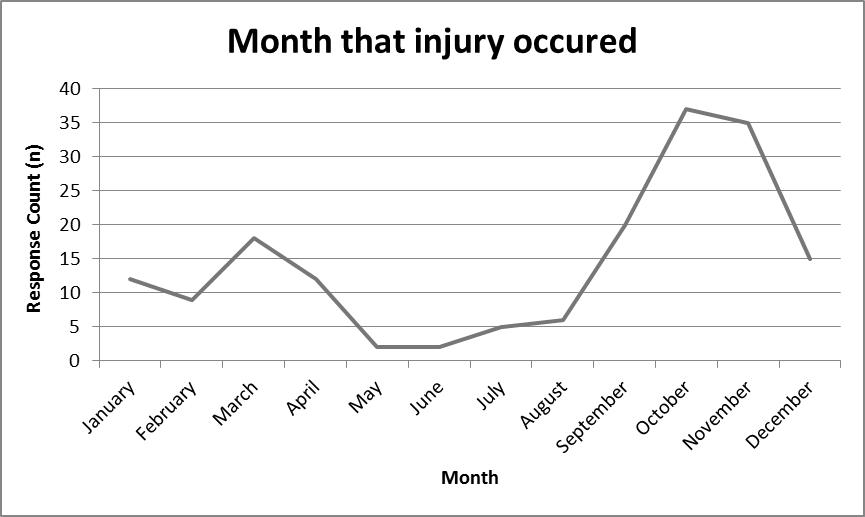 | Figure 2. Month that injury occurred for university football players during the 2011-2012 season |
4. Discussion
4.1. Profile
- The finding that UK university football defenders were injured most often followed by midfielders, strikers and goalkeepers respectively is in agreement with previous studies involving both male/female professional and youth players [2, 13, 24-25]. Researchers have proposed that defenders tend to be injured most commonly due to the nature of their role in terms of defending the high risk goal area and repeatedly challenging opposition players [13, 25]. Therefore it is recommended that an injury preventative strategy is developed within UK university football to address the imbalance of risk associated with player position and rate of injury.
4.2. Injury Description
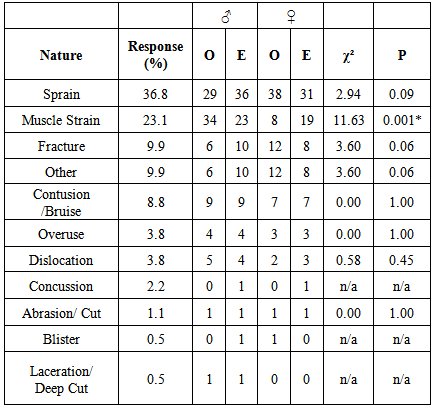
- Body Location and Nature of InjuryThe dominant lower limb (ankle: 29.5%, knee: 19.7%, thigh: 12.0%) was found to be the most commonly injured body location amongst UK university level footballers, with sprains (36.6%), muscle strains (23%), fractures (9.8%) and contusions (8.7%) reported as the most common nature of injury. These findings are consistent with research studies that investigated injury characteristics within professional and academy youth football players [3-4, 14, 16] suggesting university players present similar injury descriptors. However one notable difference between previous studies is the higher proportion of reported fractures compared to contusions. Due to the data acquired through a retrospective questionnaire, requiring subjective judgement by the players, it is possible that players may have disregarded a minor ‘bruise’ injury, instead choosing to answer the questionnaire based around a more severe injury suffered, such as a fracture. Nickel et al. [26] expressed similar concerns when obtaining injury characteristics associated with kitesurfing, concluding that retrospective studies are not the best choice for evaluating sport-specific injury rates. This problem has been avoided in previous studies by using a team doctor or player’s medical records to document all injuries incurred [3, 10]. However due to restrictions of confidentiality, budget, time and the majority of UK university football teams not having a team doctor; this study did not have access to these resources, potentially resulting in under-reporting of certain injuries or possible misdiagnosis. It is suggested that formally documenting injuries associated with university sport is placed firmly on the performance agenda in order to obtain accurate injury characteristics and risks which would aid in the development of a bespoke preventative strategy for that particular sport. Severity of InjuriesThis study reported that UK university football players incurred more major (44.8%) injuries in terms of severity compared to moderate (35%), minor (14.2%) and slight (6%) injuries. These findings conflict with previous studies that cited minor severity injuries are most common across professional and youth football populations [6, 10, 13]. As discussed previously, this may be due to under-reporting of more minor injuries. However, it is also probable that elite football players have better medical support and advice than those at university level due to enhanced resources. This enables professional players to take the appropriate steps to prevent more severe injuries occurring, by addressing potential issues including pre-season screening to detect any predisposition to injury, sufficient rehabilitation time, full-time medical staff including physiotherapists/sports massage therapists/doctors, pre-match warm up and recovery techniques, in addition to nutritional and lifestyle support mechanisms. This study suggests that university footballers within the UK may be at a higher risk of severe injuries than elite footballers and therefore it is important that steps are taken to minimise this risk. One-Off Injury vs. Re-injuryPlayers reported more one-off injuries (66.1%) than re-injuries (31.1%) which is consistent with previous elite level studies [6, 9, 27]. In conjunction with the severity of injury data, it appears that university players may be more exposed to one-off detrimental injuries, further reiterating the need for improved injury reporting and further research. This study found that the incidence of re-injury within UK University footballers was quite high compared to elite footballers (31.1% vs. 12-30%) [6, 9, 27] suggesting that university football players should be offered better medical advice and more thorough rehabilitation methods to ensure a full recovery. One way to reduce the rate of re-injuries could be through initial treatment awareness, such as the effectiveness of PRICE (Protection, Rest, Ice, Compression, and Elevation), use of prophylactic taping [2], and allowing players to achieve a full rehabilitation status that is not compromised by the students’ willingness to play due to player shortage or poor rotation policies.
4.3. Injury Occurrence
- Month that Injury OccurredThe finding that UK university players are injured most often in the autumnal months, peaking in October following summer break is consistent with previous studies conducted across other skills levels [2-3]. It is speculated that university players lose physical conditioning and fitness during the summer teaching vacation period similar to that reported by White et al. [28] in relation to professional football players within their summer break, resulting in more injuries when they return to competitive play in the autumnal period. It is also plausible that there are more fixtures at this time, due to a lower likelihood of matches being cancelled due to adverse weather conditions and as a result more matches tend to expose players to a higher risk of injury [4]. Injuries peaking immediately after summer break, may suggest that pre-season training techniques for university footballers need to be reviewed, to ensure that players are fit and conditioned for the start of the season.The Effect of Playing Surface on InjuriesThe finding that more injuries occur on grass rather than an artificial playing surface is in contrast to previous studies that reported no significant differences regarding the overall incidence of injuries on each surface [29-31]. It is speculated that the majority of university matches and training sessions are played on grass due resource issues such as lower availability of 4G/3G and AstroTurf pitches and as a consequence obtain injuries on this surface.Timing of Injury in the HalfThe timing of when match injuries occurred in each half was not significant in the study which conflicts with elite level studies reporting most injuries occurring in the last 15 minutes of each half, mainly due to player fatigue [2, 3, 15]. The opposing findings may be due to the different fitness levels of university players, different match intensities, or alternatively due to the players struggling to remember when their injury occurred over a year ago (since data was obtained via a retrospective questionnaire). However, this study suggests coaches and players should be conscious of the fact that UK university footballers are exposed to injury risk during all periods of a match and be prepared to address this trend. Activity in which injury occurredThis study is in agreement with previous research that has documented higher incidences of injury occurrence within a competitive match environment compared to training [2, 3, 4, 11]. This may have been expected considering an enhanced competitive atmosphere of matches. Alternatively, it may be speculated that university football training sessions do not reflect the same challenging and aggressive environment that is typically observed within competitive matches, and as a consequence presenting a higher risk of incurring an injury. Perhaps the inclusion of routines or practices within training that more accurately reflect a competitive environment may prepare players better for match situations.
4.4. Male vs. Female Responses
- Overall it was found that gender is not a factor in relation to the number of reported injuries, suggesting that both male and female UK university players are exposed to similar risks through their sporting participation. However, the finding that males are more susceptible to groin, thigh and muscle strain injuries compared to female players is in agreement with previous studies conducted on professional/youth populations [2, 3, 6, 8, 11, 32-33]. These injuries are typically linked to sports that involve quick acceleration and sudden changes in direction [34], suggesting that the men’s game is perhaps characterised by a higher intensity. Similarly Hagglund et al. [15] reported that male footballers tend to have more training sessions per week and competitive matches compared to females resulting in an increased injury risk due to fatigued muscles [35]. The literature also details that males are more susceptible to groin injuries relative to their female counterparts due to abdominal wall deficiency [36] and an imbalanced hip abduction to hip adductor strength ratio [37], suggesting that the role of the torso muscles in stabilising the pelvis such that the abductors and adductors can work explosively (and not get strained) is inhibited. Holmich et al. [38] reported that when athletes incorporate specific hip and abdominal strength training, the pain surrounding the locality is significantly reduced, suggesting that male UK university players should adapt similar preventative measures. Previous studies comparing gender injuries have found females to be more susceptible to knee injuries than males, particularly in relation to ligament damage [39-40]. Although this study did not concur with existent literature, it was observed that despite lacking in statistical significance, females do have a tendency to experience more ligament sprains compared with UK male footballers. Perhaps with a larger sample size significance may have been found, therefore stating that UK university female footballers are not at risk of ligament injury should be interpreted cautiously.
4.5. Strengths and Limitations of the Study
- The unique aspect about this study was researching the factors that contribute to injury rates within UK university football which has not been investigated previously. In doing so, a large amount of data was collected from various universities ranging throughout the UK providing a broad landscape of injury factors associated with this population. The major limiting factor of this study was that the amount each participant played football both in training and matches was not recorded. This information is useful in determining each player’s exposure to injury risk and to calculate the incidence of injury. It is important to take exposure to risk into account as each team most probably has different training times, number of competitive matches, supplementary training regimes, rotation of players etc. For example, most recently Clausen et al. [41] reported that adolescent female football players with a low participation (≤1h/wk) had a significantly higher injury risk compared with players participating more frequently. However, whilst this information is a key factor for epidemiological injury studies, because this study was retrospective in design, obtaining this data would have been extremely difficult for players to recall solely from memory. Data obtained in this study was via a retrospective self-report questionnaire which requires motivation to complete and challenges the player’s ability to recall previous events. Having access to medical injury records documented by team doctors/sports clinicians would have avoided these issues. However it is not common place that university football teams have access to these resources. In the future it is hoped that university football players’ participation is promoted through the support of a medical network team.
5. Conclusions
- Characteristics of injuries suffered at university level are very similar to those at elite/professional and youth levels. The dominant lower limb is most commonly affected and muscle strains/sprains are the most prevalent type of injury. University players are most often exposed to risk of injury in the autumnal period, experience more one-off injuries on a grass surface and the severity of injury high. Despite the limitations associated with obtaining data via a retrospective questionnaire, this study provides the first landscape of information in relation to UK university football injuries. Consequently there is a need for an injury surveillance initiative to be implemented prospectively involving all BUCS teams over a prolonged period of time, including team doctors and a database of players’ medical records. This will further help produce a better evidence base of the epidemiology of injuries at this level and thus pave the way for developing a preventative strategy to be introduced and ultimately improve safety whilst also promoting healthy sports participation at a university level.