-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Clinical Medicine and Diagnostics
p-ISSN: 2163-1433 e-ISSN: 2163-1441
2014; 4(1A): 21-26
doi:10.5923/s.cmd.201401.04
Marginal and Internal Crown Fit Evaluation of CAD/CAM versus Press-Laboratory All-Ceramic Crown
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMohammed M. Beyari
Department of Oral Maxillofacial, Oral Rehabilitation and Prosthetic Dentistry, Umm Alqura University, Faculty of Dentistry, Makkah, 21955, Saudi Arabia
Correspondence to: Mohammed M. Beyari, Department of Oral Maxillofacial, Oral Rehabilitation and Prosthetic Dentistry, Umm Alqura University, Faculty of Dentistry, Makkah, 21955, Saudi Arabia.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
The aim of this article is to evaluate marginal and internal fit between the all-ceramic crowns manufactured by the conventional press-dental laboratory and CAD/CAM systems. Methods: Tooth #14 was prepared per standard specification to receive an all-ceramic crown restoration. Forty-five prep tooth #14 were duplicated and randomly divided into three groups (n=15). All-ceramic CAD/CAM system (Group 1) was fabricated with the E4D CAD/CAM system according to the manufacturer's instructions. For press-dental laboratory made crowns, impressions were taken on the region area with two-step impression techniques with light and putty consistency VPS. Impressions were sent to two independent dental laboratories (Groups 2 and 3) for fabricating the monolithic press lithium disilicate crown. All crowns were cemented using Multilink® Automix (Ivoclar Vivadent) under constant pressure of 100N. Samples were embedded in acrylic and sectioned buccolingually. Sections were evaluated under digital stereo microscope and measured on three locations per buccal and lingual side of section: marginal-edge, mid-axial wall, and cusp-tip. One measurement was made on the occlusal table. Statistical analysis was accomplished with Kruskal-Wallis one-way ANOVA and significance was predetermined at p<.05. Results: No significant difference was found at the buccal and lingual margins in all groups. However, there was significance difference found for cement thickness in midaxial, cusp, and occlusal locations within the group. Conclusions: Based on the statistical results there was no statistical difference in marginal fit of all-ceramic crowns made by CAD/CAM system or dental laboratory press ceramic.
Keywords: CAD/CAM, Dental crown, Dental laboratory, Dental cement, Marginal adaptation
Cite this paper: Mohammed M. Beyari, Marginal and Internal Crown Fit Evaluation of CAD/CAM versus Press-Laboratory All-Ceramic Crown, Clinical Medicine and Diagnostics, Vol. 4 No. 1A, 2014, pp. 21-26. doi: 10.5923/s.cmd.201401.04.
Article Outline
1. Introduction
- Digital Computer Aided Design and Computer Aided Manufacturing (CAD/CAM) is a 3-dimensional scanning technology being utilized in dentistry to increase productivity and patient satisfaction. CAD/CAM technology in dentistry is quickly rising in popularity. It has been developed to eliminate the need for the traditional impression-taking, model-pouring, and laboratory-shipping steps of fabricating crowns. Optical imaging of the dentition replaces the use of conventional impression materials, and in-office mills are capable of milling an all-ceramic crown within a half-hour. CAD/CAM technology has become increasingly popular as an in-office procedure as the amount of time and money saved appeals to clinicians while the idea of fewer office visits appeals to patients. Dental clinicians strive for techniques that will take a minimum amount of time, be financially sound, and, most importantly, produce restorations with minimal marginal gaps [1]. In the past, there has been criticism of the CAD/CAM technology and its ability to create an acceptable marginal fit with restorations [2]. Since that time, however, the technology has rapidly evolved and chairside restorations have become a clinical reality [3] in which clinicians feel more confident placing an office milled crown.CAD/CAM technology has advanced greatly in recent years, which has lead to its use in many dental offices, and CAD/CAM techniques can be used in conjunction with either laboratory or chairside manufacturing [4]. CAD/CAM techniques offer the benefit of intraoral data acquisition with “optical impressions” [5] which can help reduce errors associated with conventional impression techniques [4]. Though chairside CAD/CAM technology has advanced, there are still questions regarding the marginal accuracy and internal fit of crowns produced with this technology when compared to conventional impression and laboratory produced crowns. The advantages of rapid in-office crown production are clear for both patient and provider, but the accuracy of CAD/CAM crowns has not been well documented.One of the main criticisms of office based CAD/CAM crowns is the concern that they do not fit as well as crowns manufactured in a dental laboratory. Acceptable adaptation of a crown can determine the longevity of the crown [6]. Poor marginal fit has been associated with marginal discoloration, dissolution of cement, microleakage, increased plaque retention, and secondary decay [7, 8]. This study compared the accuracy of the marginal and internal fit between laboratory produced and office produced monolithic ceramic crowns. Information regarding the comparison of these measurements is scarce [9] but is of interest to clinicians when determining the success of CAD/CAM generated crowns. The purpose of the study was to compare the in vitro marginal fit of all-ceramic crowns produced using the in-office CAD/CAM system with the fits of all-ceramic crowns produced by two independent dental laboratories. The null hypothesis was that there would be no difference in marginal fit between the methods of manufacturing.
2. Methods and Materials
2.1. Preparation of the Master Model
- Tooth #14 was prepared per standard specifications to receive an all-ceramic crown restoration on a Dentoform Typodont (Model type: D85SDP-200 Kilgore international Inc, MI). The preparation had a well-defined 3600 circumferential shoulder gingival margin, a 2 mm occlusal reduction, rounded internal angles, and 13° total occlusal convergence (Figure 1).
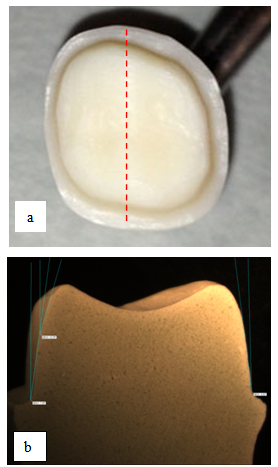 | Figure 1. a. Images of the tooth #14 preparation. b. The replicated tooth was sectioned in buccolingually direction. The total occlusal convergence was measured using the analysis software |
2.2. Fabrication of All-ceramic Crown
2.2.1. CAD/CAM System
- Each duplicated tooth was placed in a full-dentate typodont and scanned with E4D handheld digital laser scanner according to the E4D software’s specifications. The operator was trained at the learning facility provided by the D4D company (Richardson, Texas). The 3D crown design was calculated and generated from the database’s software based on the images captured during a scanning procedure. Additionally, any adjustments made to the design within the software were noted to ensure consistency. The completed crown design data was transmitted wirelessly to the E4D milling unit which was loaded with IPSe.max® CAD LT A1/C14 all-ceramic block (Ivoclar Vivadent).
2.2.2. Conventional Dental Laboratory System
- The prepared typodont tooth was placed in full-dentate typodont. A total of thirty impressions were taken on the posterior left region area utilizing double arch impression techniques and a triple-bite tray with light and putty consistency VPS impression material (Imprint™ 3, 3M ESPE). This impression technique has been well described in literature [10, 11]. The impressions were sent to two dental laboratories to fabricate the monolithic press ceramic crowns. Initial laboratory procedures for the crown followed traditional methods for cast crowns, including sterilization, model fabrication, trimming, sealing, marking of the margin, and waxing up of the tooth. The investing procedure for lithium disilicate crowns differs from traditional casting methods and manufacturer’s instructions were followed. Ivoclar IPS e.max Press LT ingots (Low Translucency) were utilized and natural glaze was used with no additional staining or layering procedures.
2.3. Crown Cementation and Analysis
- The crowns were cemented using Multilink®Automix (Ivoclar Vivadent) under constant pressure of 100N and all of the remaining cement was cleaned prior to the curing. All samples were then stored in distilled water for 24 hours at 37ºC. For sectioning, samples were embedded in clear acrylic resin and sectioned buccolingually in a consistent plane using the root indentations as guidance (Isomet 1000, Buehler). Sections were measured under digital stereo microscope with 0.8X objective (Olympus SZX16) using OmniMet software (Buehler) on three different points per buccal and lingual side of section: marginal-edge, mid-axial wall, and cusp-tip. One measurement was made on the occlusal table.
2.3.1. Measurement Landmark
- The measurement landmarks were defined in the following way (Figure. 2):
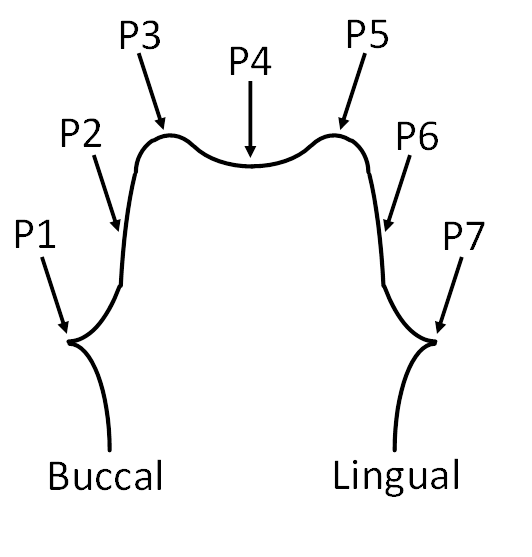 | Figure 2. Illustration images of the measurement landmarks: P1 and P7: Margin, P2 and P6: Mid-axial, P3 and P5: The junction of the axio-occlusal walls, and P4: Occlusal Plateau |
2.4. RESULTS
- Table 1 shows the means and standard deviations of marginal discrepancies and internal gaps in each group measured at all landmarks. The lingual (P7) and buccal (P1) marginal discrepancy width showed no significant differences between the in-office CAD/CAM systems with all-ceramic crowns produced by two independent dental laboratories. There were no significant differences in internal gap width (P2, P4 and P6) between in-office CAD/CAM system with all-ceramic crowns produced by two independent dental laboratories was significantly different. However, the internal gap width at P3 and P5 of CAD/CAM crowns showed significantly smaller gaps than all-ceramic crowns produced by two independent dental laboratories.
|

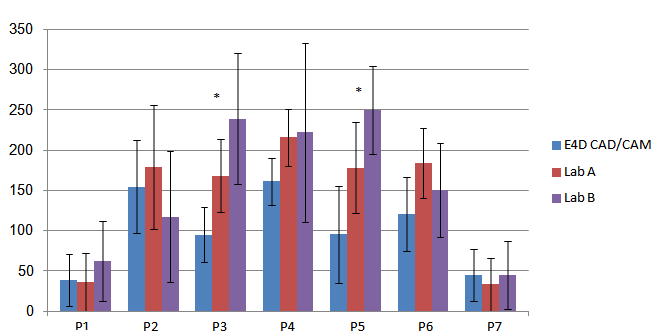 | Figure 3. The mean values and standard deviations of the marginal and internal widths measured at all landmarks.*P<0.05 |
2.5. Discussion
- In this study, no significant difference was found in marginal gap measurements between the chair side CAD/CAM manufactured crowns and the dental laboratory manufactured crowns. The literature is scarce in studies that have compared the gap measurements of laboratory processed lithium disilicate crowns and chair side processed crowns. This study compared these processes by comparing crowns manufactured in two different laboratories and chair side. Both laboratories were unaware of the fact that their crowns were part of a study and the CAD/CAM operator was experienced with using the technology. This study used a digital stereo microscope to measure the marginal gaps, as has been done in previous studies [13, 14]. Additionally, a shoulder preparation was used for the crown preparation, although many studies show that either a chamfer or a shoulder finish line can accomplish clinically acceptable margins [15, 16].The main measurement of interest for this study was marginal fit. Good adaptation has been found to be critical for the longevity of a crown [6]. Poor marginal fit can lead to secondary caries, microleakage, marginal discoloration, and dissolution of cement [7, 8]. Because marginal fit plays such an important role in the clinical outcome of a crown, clinicians will reject crowns that they do not feel are well adapted. Studying this parameter is important in determining whether or not CAD/CAM chair side crowns are an acceptable alternative to laboratory processed crowns.In the literature the clinically acceptable size of marginal gap varies. Some studies have found <120µm acceptable [17], while others found anywhere from 50-100 µm to be acceptable [18, 19]. In this study each of the investigated crown manufacturing procedures had an average of <63 µm at the marginal measurements and no statistically significant difference in marginal fit was found between crowns manufactured at the two laboratories and the CAD/CAM generated crowns. The average measurements were well below the maximum clinically acceptable 120 µm, and the majority of the measurements were beneath 50 µm with only the marginal fit on the lingual of Lab B being above 50 µm. The internal fit of the crowns was also studied. While internal fit has not been found to be as clinically relevant as marginal fit [20-24], it is still of interest as it may affect the durability of the crown [25]. Proper internal adaptation is also important as it facilitates the seating of the crown while allowing for both retention and resistance [26]. In the majority of the measurements, with the mid-axial measurement of the lingual (P2) as the exception, the CAD/CAM group had smaller internal fit measurements. The p-values for the P3 and P5 measurements were highly significant (P<.0001) with the CAD/CAM technique producing significantly smaller average measurements than either of the laboratory processed crowns. This is most likely due to the spacer that was placed during the laboratory process in these areas to prevent sharp internal angles of the crown, especially at P3 and P5, which could potentially lead to fractures or cracks of the lithium disilicate material. While the literature is somewhat sparse in comparing laboratory processed pressed ceramics to CAD/CAM crowns [9], there is literature supporting the finding of clinically acceptable marginal fit of CAD/CAM restorations of various types. In one study which compared laboratory made CAD/CAM crowns the marginal gap for each experimental crown met the clinically acceptable level [27]. Some studies have been done on composite crowns manufactured with a CAD/CAM system that have found that the marginal accuracy was clinically acceptable [16, 28]. Studies have also compared in-office CAD/CAM generated copings and those generated in a private laboratory and found that the accuracy of fit of the CAD/CAM copings was acceptable [8]. One study that compared laboratory processed pressed ceramic onlays to chairside CAD/CAM onlays found that both systems exhibited a clinically acceptable gap width of less than 100 μm [9]. Clinical studies are also of interest and one such study found that CAD/CAM chair side produced lithium disilicate crowns performed well after two years of clinical service [29].The results of this study add to the literature concerning the clinical acceptability of the marginal fit of chairside manufactured CAD/CAM crowns. If CAD/CAM technology is utilized correctly, as it was in this controlled study with an experienced operator, it is clinically accurate with adequate marginal fit.One limitation of this study was that by sectioning the samples and using a digital stereo microscope only a limited amount of data points could be observed. In future studies, with the advantage of better technology, 3-D scanning could allow for better measurements. Our department is moving forward in this direction. Another potential study could look at the longevity of the crowns under masticatory type function, comparing the difference in longevity of the crowns that may potentially arise due to the difference in internal fit, especially at the P3 and P5 measurements.
3. Conclusions
- In this study, we evaluated the in vitro accuracy of marginal and internal fit of all-ceramic crowns produced using the E4D in-office CAD/CAM system and all-ceramic crowns produced by two independent dental laboratories. Within the limitations of this study, all-ceramic crowns produced using the E4D chair side CAD/CAM system had in vitro marginal fits that were not significantly different than marginal fits of all-ceramic crowns produced by two independent dental laboratories.