-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Biomedical Engineering
p-ISSN: 2163-1050 e-ISSN: 2163-1077
2013; 3(6A): 15-21
doi:10.5923/s.ajbe.201310.03
Quality in Computorized Tomography – From Image Acquisition to Dose, Concepts, Myths and Definitions
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAntónio Fernando Lagem Abrantes 1, Luís Pedro Vieira Ribeiro 2, Rui Pedro Pereira Almeida 3, João Pedro Pinheiro 4, Kevin Barros Azevedo 5, Carlos Alberto da Silva 6
1PhD, Member of the Research Center of Sociologic Studies of Lisbon´s Nova University (Cesnova), Professor and Member of the Center for Health Studies (CES) of Algarve´s University Health School (ESSUAlg), Director of the Radiology Department and professor at ESSUAlg, Algarve, Portugal
2PhD, Member of the Research Center of Sports and Physical Activity (CIDAF) of Coimbra University, Professor and Member of the Center for Health Studies (CES) of Algarve´s University Health School (ESSUAlg), Algarve, Portugal
3Post-graduate, Member of the Center for Health Studies (CES), PhD Student at Beira Interior University, Professor and Member of the Center for Health Studies (CES) of Algarve´s University Health School (ESSUAlg), Algarve, Portugal
4Post-graduate, MSc student at the National Public Health School, Professor of the Radiology Department at Algarve´s University Health School (ESSUAlg), Algarve, Portugal
5Post-graduate, Member of the Center for Health Studies (CES), PhD Student at Cranfield University, Professor of the Radiology Department at Algarve´s University Health School (ESSUAlg), Algarve, Portugal
6PhD, Member of the Research Center of Sociologic Studies of Lisbon´s Nova University (Cesnova), Professor and Director of the School of Social Sciences of Évora´s University
Correspondence to: Luís Pedro Vieira Ribeiro , PhD, Member of the Research Center of Sports and Physical Activity (CIDAF) of Coimbra University, Professor and Member of the Center for Health Studies (CES) of Algarve´s University Health School (ESSUAlg), Algarve, Portugal.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
With this review article, we intend to demonstrate the importance of Computerized Tomography (CT) in healthcare quality and safety. The concept of safety in CT is wider than for general healthcare. Safe healthcare provided using CT must include diagnostic image quality and reliability, as this is the only way to ensure diagnostic accuracy. The images must be acquired with the most adequate protocols available and with the lowest achievable radiation dose. In this article we will focus primarily on the concepts of dose, since this variable strongly affects the image quality and the consequent diagnostic accuracy. In methodological terms, 73 papers and 6 catalogues issued by the manufacturers of CT equipment, that included the keywords low dose, ultra-low dose and dose reduction were analysed. After review of these articles we found that about 82% are chest exams, namely the lungs. The remaining were subdivided mainly by studies of the sinuses, heart and bone segments. After this review we selected the only 10 articles that present the keywords and simultaneously quantify the dose reduction. Given the lack of precision associated with these terms, introduced mainly by commercial catalogues of different equipment brands, we intend to demonstrate that the concepts low dose and ultra-low dose are wrapped in unclear marketing strategies, without a strict and unambiguous definition of what is the effective dose. We propose that these concepts should be clearly defined and a precise indication of the effective dose reduction value should be compared to the default value (standard diagnostic dose) by exam region. Therefore, it is demonstrated that there is no concrete definition of what low dose or ultra-low dose are. These slogans cannot be used until they are not holistically defined, as well as the correspondent dose reduction value.
Keywords: Dose, Low-Dose, Ultra-Low-Dose, Computed Tomography, Image Quality
Cite this paper: António Fernando Lagem Abrantes , Luís Pedro Vieira Ribeiro , Rui Pedro Pereira Almeida , João Pedro Pinheiro , Kevin Barros Azevedo , Carlos Alberto da Silva , Quality in Computorized Tomography – From Image Acquisition to Dose, Concepts, Myths and Definitions, American Journal of Biomedical Engineering, Vol. 3 No. 6A, 2013, pp. 15-21. doi: 10.5923/s.ajbe.201310.03.
Article Outline
1. Introduction
- The preoccupation of healthcare institutions about quality, as led to a progressive implementation of management systems and procedures focused on achieving higher quality standards. A healthcare quality service is one that proves able to meet customer expectations[1]. In healthcare, quality intends to be a possible target of measurement and not just a definition of good. It is more of an ongoing effort to improve, than a degree of pre-defined excellence. In relation to healthcare services, there were major changes in recent years. The increasing demand, particularly in the case of CT, meant that radiology departments had to invest effectively in their quality and not focus only on the quality of image acquisition and interpretation. This "holistic department quality" gives greater relevance to the mood and atmosphere perceived by the patient, than to the processes within the department. This concept of quality can be perverse when analyzed by the actual competitive perspective, especially focused in increasing profits through increasing the number of exams, the volume size of the acquisition or the reduction of collimation, since these are the factors that most influence negatively the dose in CT. When we discuss radiology, especially CT, we are referring to a diagnostic tool that is responsible for much of the artificial irradiation of populations. CT corresponds to about 25% of the annual average exposure in the U.S. (2006) and 50% of the exposure in terms of medical exams[2]. For this reason, CT is subject to strict monitoring of radiological protection, existing legislation to limit and reduce dose levels resulting from CT examinations[3]. Surveillance and safety measures, as well as the diagnostic reference levels (DRL´s), relate to amounts of radiation by examination or procedure. However, the introduction of concepts such as ultra-low-dose and low-dose are abstract and turn out to be purely qualitative, serving above all, in most cases, as marketing strategies. Such concepts do not effectively materialize the quantitative aspects of radiological exposure, fundamental to account for irradiation and absorbed dose. After reviewing 73 articles that address the concepts of reduction in dose, low dose and ultra-low dose, only 4 of them (Neroladaki et al[4], Bacher et al[5], Schuncke et al[6] and Bulla et al[7], although differing between them, point in fact an effective value of dose reduction.In this context and according to the available literature, some questions remain unanswered as we move forward. So what are we talking about when we refer to procedures, tests and equipment using ultra low-dose or low-dose? A CT equipment built under the concept of low-dose; uses this feature on all procedures or just part of them? What is the difference between low-dose and ultra-low dose? What measurable values (CTDI vol and DLP) are we talking about?
2. Methods
- The present study is a literature review. The research criteria established were the use of peer review papers and catalogues of CT equipment, published since January 2000. The research was guided by the following terms: Dose Reduction, Low Dose and Ultra Low Dose.After analysing the 73 documents defined above, we selected the ones that mention explicitly, in absolute or percentage value, the level of dose reduction associated to the equipment, reconstruction algorithms or protocols used in the exam.
3. Computerised Tomography – Image Quality, Acquisition and Dose
- In a way, radiology strongly reflects the technical, economic development and training policies of a country. These in turn are determined by the political environment, socio-economic status and level of urban and rural development of each country[8]. However, countries with more and better CT equipment have higher average levels of exposure, due to the greater number of examinations performed[9]. Presently, ionizing radiation from CT is the largest source of medical exposure per capita in industrialized countries (Fig. 1)[10; 11].
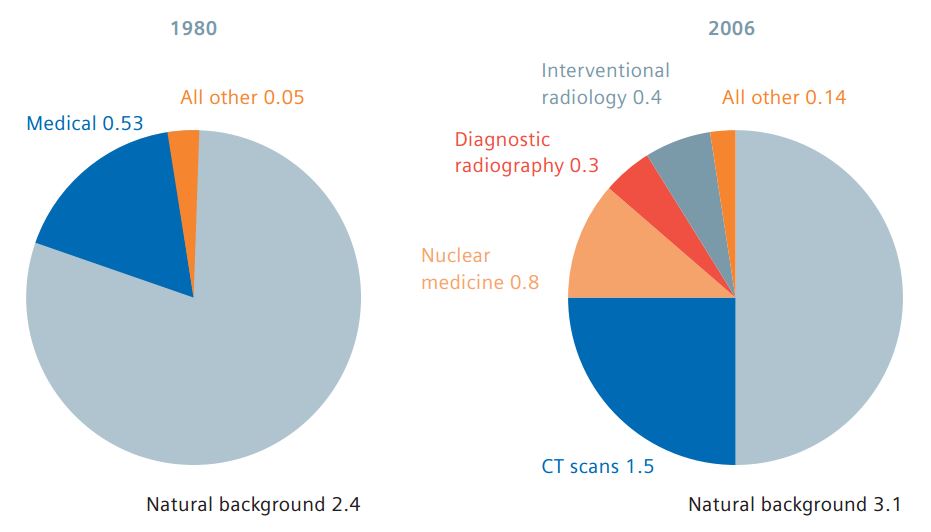 | Figure 1. Distribution and development of annual per capita dose in mSv to the population from 1980 to 2006 in the USA as an example for the development in industrialized countries |
|
|
- In summary, we intend to improve the diagnostic capacity with the lowest possible dose. Recent clinical data have shown that the algorithm IRIS using three iterations provide a similar picture quality than normal CT of the chest with a dose reduction of about 35% when compared with filtered back projection (FBP)[5]. In a study of the chest performed with a Ultra-Low Dose protocol, resulted in an exposure of 0.16 ± 0.006 mSv, values next dose of a PA and Lateral Chest X-Ray (CXR)[5], which is reported between 0, 05 and 0.24 mSv in the literature[6-17]. This corresponds to a dose reduction of 98.6% in comparison with the standard diagnostic CT dose and 94% in comparison with the low-dose CT. Regarding the study of the sinuses, by reducing the current output / time at 20%, 40% and 60% were obtained dose reductions of up to 60% compared to the initial protocol. The best image quality, according to the researchers, was verified with a dose reduction of 20%[7]. The image quality produced by these protocols is subjective because there are few studies on the subject. As we know, low-dose CT reduces radiation exposure, but decreases the signal to noise ratio and consequently the diagnostic capabilities[18]. However, the results regarding the quality of the image look promising. In this study, we found that the use of MBIR provides even greater noise reduction, compared with only ASIR. The noise reduction of 12%, 28% and 79% was achieved by ASIR-40-80 and ASIR MBIR, respectively, which is in agreement with the results published recently by other researchers[19]. As a result, the Iterative reconstruction techniques lead to a significant increase in image quality, reducing its noise, even in cases where the contrast-to-noise ratio is very low. As a result, CT scans can be performed with a significantly lower dose, remaining however the diagnostic image quality[16]. In the past two years, several studies have examined the effects on patient dose and image noise of various iterative reconstruction methods. All showed significant reductions in radiation dose (up to 40% -50% in some cases)[20, 21, 22]. A study which was analysed in the algorithm SAFIRE body scans (abdomen), showed a dose reduction by 50% while preserving image quality[22]. With doses of radiation constant, SAFIRE (Sinogram Affirmed Iterative Reconstruction) can reduce image noise by 35% and improve the noise contrast in 50%[23]. When we move away from marketing strategies, the concepts of low dose and ultra-low dose become nonspecific and undefined. From the healthcare point of view, especially CT, along with the traditional concepts of quality in healthcare, we have to add image quality and patient safety[24]. Image quality is not a clear issue nor is it consistent among specialists, raising questions as: to which extent CT image provides information for establishing a diagnosis? When an image is no longer suitable for diagnostic?When analysing image quality in CT, we are interested in the same level of consistency and to what extent it actually rigorously corresponds to the patient. Many factors influence a CT image (the representation of an object in digitized form). To assess what concerns us, if the image represents the actual anatomy, we mainly consider two main features: the detectability of resolution or low contrast resolution and detail that is, the high contrast resolution. The high contrast resolution is the level of detail that is visible in the picture. For example, two thin lines are very close to an object, will they be identified on the image as two separate lines? The low contrast resolution is the system's ability to distinguish objects with similar densities. For example, consider an object (i.e. small tumor) which has almost the same density as the tissue around it. Will this object be detectable on the image?[25]. We are in the field of healthcare safety. So what is safety in TC? Is this concept only related to radiation protection and dose reduction? Clearly not! Safety in TC, as in other imaging methods that use radiation, must be broader than the generalist definitions of Patient Safety[24].We need to ensure that the level of noise that we accept for a particular study is balanced. On one hand we need guarantees that we do not lose any detail in the image that would allow us to establish the diagnostic, and secondly, to respect scrupulously the ALARP principle (as low as reasonably practicable). We must also combine the issues of noise with the radioprotective capacity of dose modulation software, as it reduces dose according to the pattern of noise for a certain image or anatomical region. Typically, this noise level is defined by the type of exam. The results obtained in a study published in 2012 for abdominal exams performed on a 6 slice CT, showed that the radiation dose received in these tests also depends on some of the patient´s characteristics, being important to adjust the acquisition parameters to patient’s dimensions. An effective method is the use of automatic exposure control (AEC) which allows reducing, or varying, the tube current according to the size of the patient. In the case of children, this method is not sufficient and there should be special attention due to their increased radiosensitivity, using paediatric protocols and taking into account all the precautions and principles of radiation protection. In some types of CT scans, it is possible to make the image acquisition with lower dose to the patient, which leads to increased image noise. This increase in noise is acceptable as long as images continue to enable an efficient clinical diagnosis.[26].
4. Discussion
- After reviewing the literature, we found no description that quantifies dose reduction with the concepts low dose and ultra-low dose. It is necessary to establish a clear and unambiguous quantitative definition of these concepts. We know only that each contains a reduced level of dose administered to the patient for the same (or similar) CT Scan. With the exception of four articles[5, 6, 7, and 17], there is no quantitative mention of how much dose reduction each concept provides in relation to the previous protocols used.All major manufacturers of CT provide meaningful tools to reduce the radiation dose. Not many users take advantage of the capabilities of their equipment to reduce the dose, due to lack of familiarity and knowledge of how such tools work[16]. We also know that each tool can be used individually, but when combined, have a synergistic effect in reducing the radiation dose[16].In addition to all the tools available, we cannot forget what has been observed between 2006 and 2008: a decrease in dose on chest CT, always using the same equipment. As noted above, this dose reduction occurred without any change in equipment, which emphasizes the importance of acquisition protocols, combined with techniques for dose management in CT[27]. Certainly the increased routine of teams trying to achieve the universal goals of dose reduction inherent in all the diagnostic techniques that use ionizing radiation, are responsible for the fact noted earlier.As regards the concepts and ultra-low dose low-dose recently introduced, remains only a qualitative reference for dose level, because they are devoid of any quantitative reference standard. It is clear that there is no concrete definition of what is and what matches each. The concept is an ultra-low dose supposed evolution of the low dose, although, with the exception of an article[5], which we cannot quantify the value of reduced dose of ultra-low dose compared to low dose.As shown, the scientific literature, these two designations used without reference is made (in the percentage or absolute value) as the equivalent each. Regarding the concepts of qualitative dose measurement, low dose and ultralow dose are devoid of any quantitative standard reference that allows us to determine where one begins and the other ends, much less which concept manufacturer´s marketing campaigns will follow. As we have seen, there is a starting point, a DRL, which is much connoted with the FBP algorithm used in CT since the 1970´s. This algorithm has been the reference from which we intend to establish buzzwords that characterize dose reduction, but often we cannot quantify it. Established standard diagnostic dose references, when we speak about low-dose, what is the percentage decrease of radiation dose? And for ultralow-dose what should we expect in relation to the standard diagnostic dose, or in relation to the low-dose concept? In fact, we found in the literature, several references that enable us to conclude that we have presently on the market, algorithms that reduce the dosage from about 35% (IRIS using three iterations) to 98.6% (ultralow dose CT). We also found that the reduction of dose related to the concept of low-dose is about 94%, compared with standard diagnostic dose. Thus we see that the ULD has an absolute value close to 40% to 50% reduction for the LD concept [14 ,15, 16].According to several researchers, this pattern appears constant for chest studies. There are also studies that measure the image quality for this anatomical region, by using technical expert boards or Delphi panels[15, 16]. The chest (lung) therefore seems to be the prime test spot for dose reduction. As we analyse other anatomical regions, we found a large dispersion and discrepancy.In summary, according to the previously defined quality standard of care in CT, we can focus on the issues of dose reduction, and proceed to the goal of providing safe care; we must assume that image quality and any assumptions generically associated with health care quality are complied. Thus, in order to provide safer healthcare and make wise choices in CT, we need to delimit the concepts of low dose and ultra-low dose.There are no studies that define the concepts assertive low dose and ultra-low dose, similar to what happened at the beginning of the XXI century with the concept of pitch, it is necessary to normalize definitively which corresponds, under penalty of being an expression trivialized.It is important that the responsible authorities and departments for radiation issues define among which ranges of percentage of the standard diagnostic dose we can call dose reduction as LD and ULD. This concept should be established by the type of examination.
5. Conclusions
- The main results of this literature review point to the inexistence of literature that clarifies all the concepts related to Dose Reduction, Low Dose and Ultra Low Dose.These terms were introduced by CT equipment manufacturers and are used when it is intended to refer dose reduction. Although, these terms rarely discriminate, in absolute or percentage values, the effective dose radiation reduction achieved by the several techniques and technologies used.The dose reduction concept, due to his non-specificity and qualitative connotation, must be understood as any technique, technology or software that reduces the radiation level, when compared to a similar exam with the same diagnostic goals. This concept is fairly explained in the literature.However, it is unclear in the majority of the documents analysed, what should be the reference to use when it is intended to quantify the dose reduction level.Some literature is obscure when expressing that the reference pattern is the filtered back projection reconstruction algorithm.The reference pattern to be used when quantifying the radiation dose variation must be indicated unequivocally and universally.We also propose, based on the reduction of effective dose per examination type, an interval scale for the classification of new technologies (CT equipment), averaged over the dose values obtained after analysis of the levels of all types of examinations that the equipment can perform. This way we would know the real value of dose reduction (considering the maximum permissible standard deviation) for each of the concepts associated with dose reduction.Finally, it is intended that the findings of this article serve as a point of reflection on the determination of concepts extremely important and sensitive computerized tomography, starting from studies that have consolidated and universally quantify their use, under penalty of being trivialized foreseeable future.
ACKNOWLEDGEMENTS
- I would like to thank all radiology professional who work with CT, as well as all those who have contributed to the development of this diagnostic tool with increasing quality and safety.