-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Surgical Research
p-ISSN: 2332-8312 e-ISSN: 2332-8320
2024; 12(1): 9-13
doi:10.5923/j.surgery.20241201.02
Received: Jul. 28, 2024; Accepted: Aug. 15, 2024; Published: Aug. 23, 2024

Treatment of Congenital Bronchial Lesions
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKh. X. Sultanov1, M. M. Aliyev2, U. X. Tilavov2, S. T. Islomov1, Auyezov Ali Muxtar Uli1
1Department of Pediatric Surgery, National Children’s Medical Center, Uzbekistan
2Department of Pediatric Surgery, Tashkent Pediatric Medical Institute, Uzbekistan
Correspondence to: Kh. X. Sultanov, Department of Pediatric Surgery, National Children’s Medical Center, Uzbekistan.
| Email: |  |
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

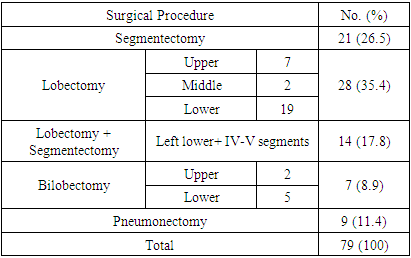
Objective. To review the surgical management of congenital bronchial lesions - bronchiectasis (CB) in a pediatric surgery unit over a period of 16 years. Patients and Methods. We retrospectively reviewed the medical records of 116 consecutive children who underwent surgery for CB in our clinic between 2004 and 2024. Results. Seventy-nine patients underwent 83 pulmonary resections during the study period. The mean ages at diagnosis of CB and at the time of surgery were 8.10 ± 4.10 years (range, 1 to 17 years) and 9.70 ± 4.20 years (range, 2 to 18 years), respectively. There were 44 males (55.7%) and 35 females (44.3%). The causes of bronchiectasis were congenital hypoplasy of bronchi (n = 31), secondary bronchiectasis was additional nonspecific pulmonary infection (n = 42) and foreign body aspiration (n = 6). Chest X-rays, bronchography and bronchoscopy (n = 79), chest HRCT (n = 61), angiopulmonography (n = 23) were used, and pulmonary function tests (n = 48) were performed. The types of resections were segmenectomy (26.5%), lobectomy (35.4%), and lobectomy with segmentectomy (17.8%), bilobectomy (8.9%) and pneumonectomy (11.4%). The postoperative status of the patients as follows: “well” in - 49 patients (60.7%), “improved” in 23 patients (29.5%), “worsened” in 6 patients (7.7%). Moreover, unfortunately two patients “died” (2.6%). Conclusions: A radiologic and morphologic evidence of reversal of airway abnormality has been shown in cases of congenital defects of bronchial wall. The morbidity and mortality rates of bronchiectasis surgery are within acceptable ranges. Segmentectomy and lobectomy are well tolerated in children without increase in morbidity and mortality.
Keywords: Bronchiectasis, Airway abnormality, Pulmonary resection, Children
Cite this paper: Kh. X. Sultanov, M. M. Aliyev, U. X. Tilavov, S. T. Islomov, Auyezov Ali Muxtar Uli, Treatment of Congenital Bronchial Lesions, International Journal of Surgical Research, Vol. 12 No. 1, 2024, pp. 9-13. doi: 10.5923/j.surgery.20241201.02.
Article Outline
1. Introduction
- Congenital bronchiectasis (CB) is rather uncommon, and knowledge of this disorder is not very extensive. CB is defined as permanent and irreversible abnormal dilatation of bronchi, and is usually considered to be acquired. There is a type of bronchiectasis which is probably congenital in origin, although in most cases this is difficult to prove [6,10]. Congenital cystic bronchiectasis is thought to be the result of developmental arrest [16]. This may result in cyst formation, retention of fluid or air, and the risk of subsequent infection [1]. Congenital cystic bronchiectasis has been found almost exclusively in infants and young children [2,3] and also has been reported accompanying other congenital anomalies [4], or in patients with deficiency of bronchial cartilages. Surgery was considered the only alternative method for the treatment of bronchiectasis in the early and mid years of this century. However, the indications for surgery have been limited in recent decades because of expectant results of conservative treatment [12,14]. Although there are no prospective randomized trials comparing the efficacy of conservative and surgical treatment options, the indications of surgery for bronchiectasis can be considered in 2 main categories among children. Surgery can be performed for eradication in children suitable for total resection who do not respond to conservative treatment or for controlling the symptoms by removing the worstinvolved part in children with diffuse bronchiectasis [16]. A retrospective series analysis was conducted to evaluate the results of surgical treatment according to the reasons and procedures in children with bronchiectasis.
2. Materials and Methods
- We reviewed the medical records of all children who underwent surgery for bronchiectasis between 2004 and 2024 at Pediatric Surgery Department of the TasahPMI and NCMC. Medical records of 116 patients were analyzed for age, gender, clinical characteristics, radiologic findings and details of surgery including type of resection, operative morbidity, mortality, and overall outcomes.Surgical treatment was considered if the symptoms persisted in spite of repeated courses of medical treatment including antibiotics, mucolitics, chest physiotherapy, bronchodilators, or steroids. Candidates were evaluated for the resectability of all diseased lung tissue or the expected benefit after excision of most affected parts of lungs with extensive disease.Preoperative bronchography or chest high-resolution computed tomography (HRCT) was performed to evaluate the type, severity, and distribution of CB. Pulmonary function tests were done to estimate the lung function. Bronchoscopy was performed in all patients to rule out bronchial obstruction or stenosis caused by foreign body or endobronchial tumor.Preoperative bronchoscopy was performed to clear bronchi and to prevent spillage of secretions during operation. Surgical acces was obtained via posterolateral thoracotomy in all patients. The fourth or fifth intercostal spaces were used to reach the diseased lung area. The most common surgical procedures were formal segmentectomy and lobectomy, however, in some of the cases, when required lobectomy plus segmentectomy, bilobectomy and pneumonectomy was performed. A chest tube was placed and connected to an underwater seal system by Byulau in all patients. Postoperative management included intensive chest physiotherapy, analgesic, and antibiotics.Complications were analyzed for intraoperative and postoperative periods. The outcome of surgery was evaluated at last follow-up visit and rated according to the degree of symptoms. Symptoms were categorized as follows: “well” when the patients are free of symptoms, “improved” when patient’s symptoms redused, “worse” if the patient’s symptoms persist.
3. Results
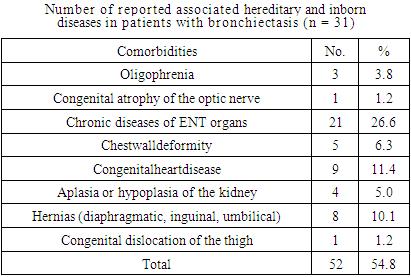
- Seventy-nine patients underwent 83 pulmonary resection operations with the diagnosis of bronchiectasis during the study period. The mean ages at diagnosis of bronchiectasis and at the time of surgery were 8.10 ± 4.10 years (range, 1 to 17 years) and 9.70 ± 4.20 years (range, 2 to 18 years), respectively. There were 44 males (55.7%) and 35 females (44.3%). The causes of bronchiectasis were nonspecific pulmonary infection (n = 42), congenital hypoplasy of bronchi (n = 31), and foreign body aspiration (n = 6). The details of comorbidities are shown in Table 1.
|
|
|

4. Discussion
- Bronchiectasis was uniformly fatal when it was described in detail by Laennec in 1819. Demonstration of abnormalities of bronchial architecture by using nebulized bismuth powder and iodized oil allowed further understanding of the pathogenesis of bronchiectasis. In modern description, bronchiectasis is characterized by abnormal, irreversible dilatation of the bronchi in association with a variable degree of chronic bronchitis, pneumonitis, or other pathologic changes.The common cause of bronchiectasis is bacterial infection usually after pneumonia. Other causes include pertussis, viral infections, and obstruction secondary to foreign body aspiration, tracheobronchial aspiration, congenital lesions and immune deficiency [5]. Cystic fibrosis is the most common cause of bronchiectasis especially in the white population of Europe and North America. Nonspecific pulmonary infection was the most frequent cause of bronchiectasis in our series. The prevalence of bronchiectasis decreased significantly over recent decades. In the base of some of bronchiectasis lays the hypoplasia of the bronchial wall elements, bronchioles and alveolus in whole or limited area of the lung [8,10]. Antimicrobial therapy and immunization against viral and bacterial agents significantly decreased the incidence of bronchiectasis. Early recognition of foreign bodies with bronchoscopy also decreased the incidence of postobstructive bronchiectasis. However, the incidence of bronchiectasis is still high in developing countries [9].The initial treatment of bronchiectasis is conservative and includes reducing airway obstruction and elimination of microorganisms from the lower respiratory tract. Therefore, medical therapy for bronchiectasis consists of antimicrobial therapy, postural physiotherapy, bronchodilators, corticosteroids and bronchoscopic cleaning of the tracheobronchial tree [15].The main rationale for surgical treatment of bronchiectasis is to increase the quality of children’s lives and protect them from complications such as empyema, hemoptysis, and lung abscess. The successful results can be achieved only by careful and proper selection of candidates for surgery. Instead of following rigid criteria for patient selection, each child should be evaluated separately for surgery [7,11].The indications for surgery are not fully established in children. However, there seems to be agreement that the appropriate antibiotic therapy and chest physiotherapy should be tried for a period. In adults, indications for surgery have been reported to be resistance to appropriate antibiotic therapy in addition to an extensive postural drainage and chest physiotherapy program for a reasonable period of at least 2 years. In children, in addition to the above-mentioned criteria, growth retardation, failure to thrive, inability to follow the educational program because of frequent infections, and socioeconomic status of the family should also be considered when deciding on surgical treatment [10].Since all diseased parts of the lung can be resected, the decision for surgery is relatively easy in children with localized bronchiectasis [13]. The presence of accompanying complications such as growth retardation, abscess, and hemoptysis help surgeons in their decision for operation. However, when the bronchiectasis diffusely affects multiple lobes or segments and sometimes both lungs, the operative decision is quite difficult. Especially in the presence of comorbidities such as deformation of thorax and congenital heard diseases, total resection of all affected tissue usually is impossible. All candidates of surgery should be free of an ongoing pulmonary infection at the time of operation. Broad-spectrum antibiotics should be given in the preoperative period. Bronchoscopy should be performed in all candidates to exclude bronchial obstruction caused by a foreign body. Bronchoscopy should be also done just before the operation to clear airways. In our series, a rigid or flexible bronchoscopy, or both, was performed for the removal of secretions and the detection of a foreign body or an endobronchial lesion [15].The localization of disease should be evaluated radiologically. Bronchography had been used extensively for both diagnostic and follow-up purposes in bronchiectasis. Although it was very sensitive and informative, it has been almost totally abandoned today in children. High-resolution chest CT has replaced the bronchography. Angiography has been recommended to find out whether the diseased area is perfused and detected of pulmonary vessels hypoplasy. It has been suggested that only nonperfusing lung and pulmonary vessels hypoplasy areas should be resected [9]. Pulmonary function tests may not be required in children with localized bronchiectasis. However, it should be performed in cases of extensive involvement or in patients undergoing reoperations.The aim at operation is to excise all diseased lung areas whenever possible and to preserve as much healthy lung parenchyma as possible. It is known that even only 2 or 3 preserved segments can fill the hemithorax, if operation had performed till 8 age old. All resections should be performed within anatomic limits. Lobectomy was the most frequently performed operation in our series. Left lower lobe was the frequently affected area as seen usually in bronchiectasis. Pneumonectomy was the second most frequent operation. Although pneumonectomy has been accepted to result more complications and mortality than that of other limited resections, complications has occurred after removing much volume lung tissue, such as lobectomy plus segmentectomy, bilobectomy and pneumonectomy in long-term period, and it has been well tolerated in children in the current series.The success of surgery for CB is directly related to the extension of the disease, underlying cause of bronchiectasis, and the completeness of the resection. Most of the children benefited from bronchiectasis surgery with regression of symptoms. Bilateral bronchiectasis exposed a high risk of mortality with all deaths occurring in these children. We could not find the exact cause of deaths in this patient, because no autopsy was allowed. Patients with bilaterally bronchiectasis should undergo a complete cardiologic evaluation for possible accompanying intrinsic abnormalities before operation [16]. Total excision of the diseased lung areas was accomplished in most children resulting in an apparent improvement in symptoms. However, symptoms have been persistent in children who had incomplete resection [10]. Whether in the same or other site, the presence of residual diseased lung area has the potential to produce symptoms.
5. Conclusions
- The decision for surgical intervention should be made in cooperation with the chest diseases unit. Anatomic localization of the disease should be mapped clearly by radiologic investigations. In addition, radiologic and morphologic evidence of reversal of airway abnormality has been shown in cases of congenital defects of bronchial wall. The morbidity and mortality rates of bronchiectasis surgery are within acceptable ranges. Most of the children benefit from the surgery, especially when total excision of the all diseased lung areas can be accomplished. Segmentectomy and lobectomy are well tolerated in children without increase in morbidity and mortality. Therefore, resection of damaged part of the lung tissue may be preferred instead of removing much volume lung tissue, but pneumonectomy may be preferred instead of leaving residual disease in the absence of contralateral lung involvement.
Compliance with Ethical Standards
- Funding: This study was not funded.Conflict of Interest: Authors declares that they have no conflict of interest.Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee.Informed consent: Informed consent was obtained from all individual participants included in the study.