-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Surgical Research
p-ISSN: 2332-8312 e-ISSN: 2332-8320
2020; 9(1): 17-22
doi:10.5923/j.surgery.20200901.03
Received: Nov. 14, 2020; Accepted: Nov. 30, 2020; Published: Dec. 18, 2020

Clinicoepidemiological Survey of Tonsillitis in Ekiti State University Teaching Hospital, Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLWaheed Atilade Adegbiji 1, Shuaib Kayode Aremu 2
1ENT Department, Ekiti State University Teaching Hospital, Ado Ekiti, Ekiti State, Nigeria
2Afe Babalola University, Ado-Ekiti, Ekiti State, Nigeria
Correspondence to: Shuaib Kayode Aremu , Afe Babalola University, Ado-Ekiti, Ekiti State, Nigeria.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

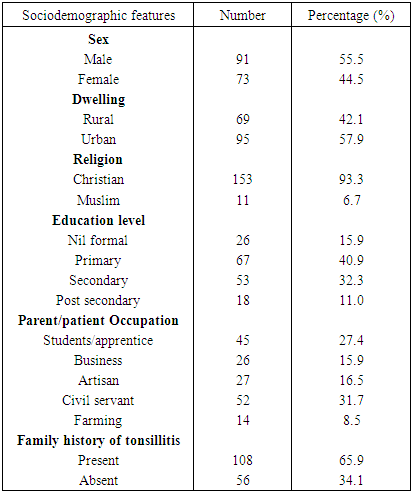
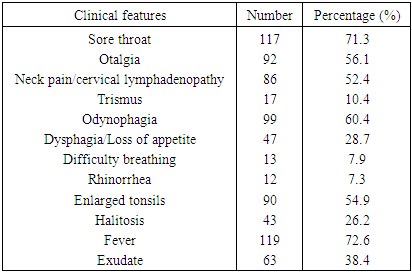
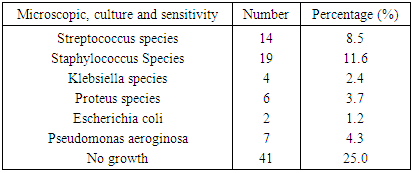
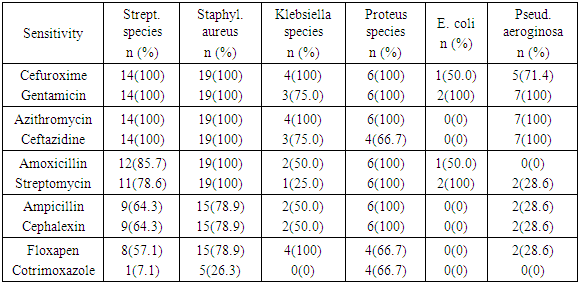
Background: Tonsillitis is a common throat infection with poor documentation in developing countries. In this study, we aimed to evaluate the prevalence, sociodemographic features, clinicoepidemiological survey, and bacteriology of tonsillitis among patients in our practice. Materials and Methods: This was a prospective study of all patients with a diagnosis of tonsillitis at Ekiti state university teaching hospital, Ado Ekiti, Nigeria. Data was collected using a pretested interviewer assisted questionnaire. Bacteriological investigations of tonsils were done and results were recorded. Data obtained were collated and analyzed using SPSS version 18.0. Results: Prevalence of tonsillitis was 12.7%. There were 55.5% males and male to female ratio was 1.2:1. A family history of tonsillitis occurred in 65.9%. The commonest type of tonsillitis in this study was 59.1% recurrent tonsillitis. The majority 38.4% of the patients were referred by a paediatrician. The majority 70.7% of the patients were seen in the ear, nose, and throat outpatient clinic. Most of the patients presented with fever, sore throat, and odynophagia in 72.6%, 71.3%, and 60.4% respectively. Frequent findings on clinical examination were 54.9% enlarged tonsils and 52.4% neck pain/cervical lymphadenopathy. No bacteria were isolated from 25.0% patients while common isolated bacteria were 11.6% Staphyloccocus aureus and 8.5% Streptococcus species. In this study, isolated Streptococcus species and Staphylococcus aureus showed 100% sensitivity to cefuroxime, gentamicin, azithromycin, and ceftazidime. Commonest associated complication was otitis media in 18.9%. Conclusion: Tonsillitis is quite a prevalent febrile illness with a sore throat and enlarged tonsils. Diagnosis is commonly omitted, poorly treated with associated complications at presentation to the specialist clinic.
Keywords: Tonsillitis, Prevalence, Bacteriology, Febrile illness, Nigeria
Cite this paper: Waheed Atilade Adegbiji , Shuaib Kayode Aremu , Clinicoepidemiological Survey of Tonsillitis in Ekiti State University Teaching Hospital, Nigeria, International Journal of Surgical Research, Vol. 9 No. 1, 2020, pp. 17-22. doi: 10.5923/j.surgery.20200901.03.
1. Introduction
- Tonsillitis is a throat disease that is characterized by the inflammation of the tonsils secondary to different types of infection [1,2]. The tonsils, palatine tonsils is one of the major lymphoid tissue in the lateral wall of the oropharynx. They help in the immune system which protects the body against various forms of infections that may enter through the upper aerodigestive tract [3]. It is major caused by various type viral or bacterial infection others were fungal and tuberculosis [4,5] Infected mucous from the patient are contagious and spread by contact with the mouth, throat or air droplet from sneezing. Infected tonsils are inflamed, enlarged, engorged, red, with or without yellow or white coating [6-11]. Post-treatment, the majority of the patient may recover completely or progress to recurrent tonsillitis or chronic tonsillitis [12]. Untreated or poorly treated cases may develop peritonsillitis, peritonsillar abscess, parapharyngeal abscess, retropharyngeal abscess, and other forms of systemic complications. There are different types of tonsillitis in clinical practice [11-14]. Acute tonsillitis occurred when the disease duration is less than three weeks. Subacute tonsillitis is when symptoms last between three weeks to three months. Recurrent tonsillitis is frequent attacks of acute tonsillitis over a year or two. Chronic tonsillitis is characterized by symptoms of tonsillitis last more than three months. Peritonsillar abscess when there is an accumulation of purulent suppuration in the peritonsillar capsule.Patterns of clinical manifestations of tonsillitis depend on the type of tonsillitis. Common symptoms include a sore throat with associated referred otalgia, neck pain, and trismus in acute and recurrent tonsillitis [15]. Also, sore throat is associated with dysphagia and odynophagia in acute or recurrent tonsillitis. Chronic tonsillitis is associated with difficulty breathing, cough, snoring, halitosis, sleep apnoea, reduced appetite, and weight loss. Acute symptoms include fever, chills, and malaise. Associated constitutional symptoms are loss of appetite, nausea, vomiting, stomach ache, and furry tongue which may mimic other febrile illnesses. Clinical findings are enlarged cervical lymph node, swollen tonsils, pus on tonsils crypts [16-19].There are only a few studies on tonsillitis in developing countries particularly in Nigeria in the literature. In this study, we aimed to evaluate the prevalence, sociodemographic features, clinicoepidemiological survey, and bacteriology of tonsillitis among patients in our practice.
2. Materials and Methods
- This was a prospective hospital-based study of all patients with a diagnosis of tonsillitis at Ekiti state university teaching hospital, Ado Ekiti, Nigeria. This study was carried out over one year between July 2018 and June 2019. Data was collected using a pretested interviewer-assisted questionnaire. Data were obtained on sociodemographic features. Others were presenting complaints such as sore throat, painful swallowing, difficulty breathing, cough, snoring, halitosis, sleep apnoea, fever, and malaise on the onset, duration, frequency, severity, relieving factor, and treatment. Ear, nose, and systemic symptoms were obtained and documented. Detailed oropharyngeal, neck, ear, and nose examinations were done and findings were also documented. Bacteriological investigations by tonsils swab were taken for microscopic, culture, and sensitivity tests. Results were obtained and findings were recorded. Data obtained were collated and analyzed using SPSS version 18.0. The data were expressed with descriptive statistics by frequency distribution table, percentage, bar chart, and pie chart. Ethical clearance for this study was sought and obtained from the ethical committee of the hospital. Informed consent was obtained from the enrolled patient, parent, or guardian.
3. Results
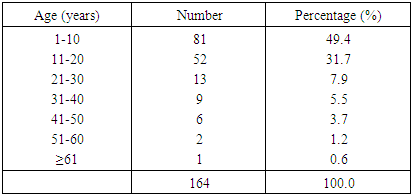
- The total number of patients seen in the ear, nose, and throat department over the studied period was 1,296 out of which 164 patients had tonsillitis. The prevalence of tonsillitis was 12.7%. All the studied age groups were involved with a peak age value of 81 (49.4%) at the first decade of life and the least age value of 1 (0.6%) at the extreme age group of ≥61 years. As illustrated in table 1.
|
|
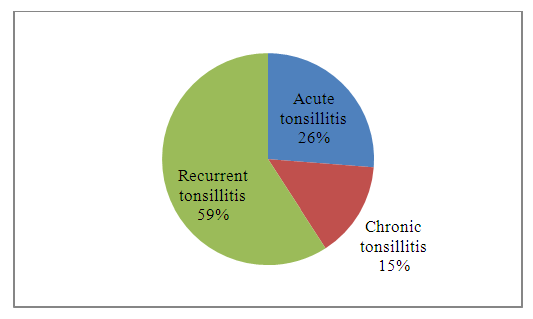 | Figure 1. Types of tonsillitis among patients |
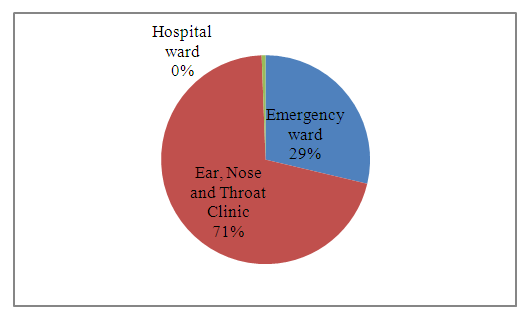
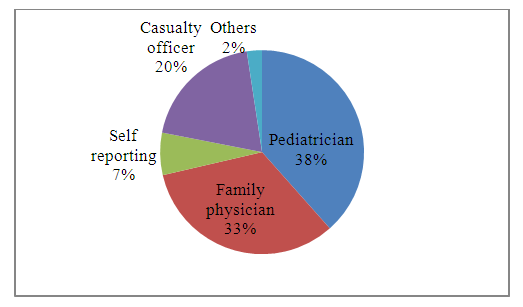 | Figure 2. Sources of referral among patients |
 | Figure 3. Pattern of presentation among patients |
|
|
|
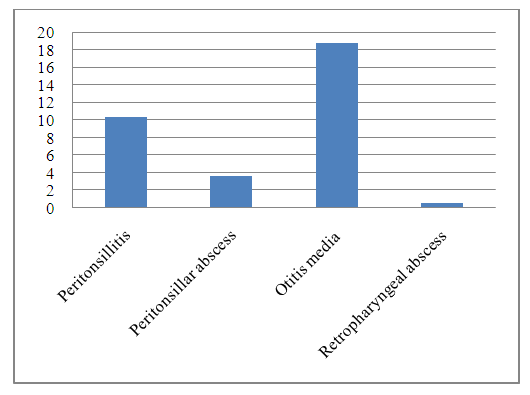 | Figure 4. Complication of tonsillitis among patients (bar) |
4. Discussion
- Tonsillitis is a common throat disorder with poor epidemiological studies in developing countries including Nigeria. In this hospital-based study, the prevalence of tonsillitis was 12.7%. This prevalence was lower than findings from other studies [20,21]. The lower patient presented in this study center may be due to our peculiar sociocultural practice of treatment of sore throat with jin and spicy local concussion by the sufferer. On sociodemographic features, tonsillitis is commoner in children and younger age groups compared to adults. A study conducted in Scotland also found tonsillitis to be commoner in children compared to adults [22]. This may be due to cross-infection among school children with the habit of sharing utensils and cups. Another contributing factor is the high incidence of family history of tonsillitis in this study [23]. The order of prevalence of families with tonsillitis were siblings, mother, father, and other relatives, and this is further determined by their closeness and family ties. Most patients with tonsillitis believed it is a minor illness and was not a communicable disease. Prevalence of tonsillitis was higher in males than females in this study. This is contradictory to findings from the previous study in other parts of the world which revealed higher female prevalence [24]. This may be secondary to a higher incidence of outdoor activities in males than females. More males feed outside the home in the eatery, cafeteria, and local food vendor sharing poorly treated cups and utensils after use. This habit was commoner among urban dwellers, businessmen, students, and apprentices in this study. In this study majority of the patients were diagnosed with recurrent tonsillitis. Many patients and their relatives believe tonsillitis is a minor illness that can be cured with a homemade herbal concussion as a remedy. Also, some believe that it is a self-limiting disease. The second most common type of tonsillitis is acute tonsillitis followed by chronic tonsillitis they present early and late respectively. Both acute and recurrent tonsillitis mainly presented due to odynophagia which may be severe enough to cause total dysphagia or limit the patient to a liquid diet. The majority of chronic tonsillitis seek expert opinion due to persistent throat discomfort or obstructive symptoms. The patients first approach to the treatment of tonsillitis was home care followed by over the counter drugs or pharmacy. Failure of all these cares usually the prompt patient or their relatives to contact a family physician for definitive treatment. Referral of the patient to specialist was mainly from the family physician or paediatrician if treatment failed. Unfortunately, the majority of the patient presents in ear, nose, and throat outpatient clinic in the subacute state. Few cases presented in casualty with complicated tonsillitis. Majority of our patients presented with fever and sore throat. Many of the patients were treated as a case of either Malaria or Typhoid fever. Which are common causes of fever in the Malaria endemic zone. Unfortunately, the majority of the primary health care officer does not consider tonsillitis as one of their differentials in their diagnosis. Clinical examination of the oropharynx revealed enlarged inflammation of the tonsils. Oropharyngeal examinations are not routinely done and these findings are often omitted by the primary health care officer. This finding is contrary to the report from other studies [25,26]. In this study, no growth of bacterial was reported in about half of the throat swab sent for microscopy, culture, and sensitivity test. This is most likely due to wrong diagnosed Malaria or Typhoid fever and inappropriate antibiotics with another form of treatment. The most common isolated bacteria were Staphylococcus aureus which is followed by Streptococcus spices and Pseudomonas aureginosa. All these bacteria were found in acute tonsillitis and recurrent tonsillitis. Similar results were recorded from other studies on the most common isolated bacteria [27,28]. A contrary result was reported from another study [29]. These different findings may be due to different population studies, sociocultural practices, and types of abused antibiotics. Staphylococcus aureus and Streptococcus spices in this study were found to be sensitive to Cefuroxime, Gentamicin, Azithromycin, Ceftazidime, Amoxicillin, Streptomycin, Ampicillin, Cephalexin, Floxapen, and Cotrimoxazole as in other studies [27,29]. Slight different results of some antibiotics resistance were reported in other studies [21]. The observed differences in antibiotics sensitivity maybe after the wrong diagnosis and inappropriate antimicrobial administration. This practice leads to the waste of scarce resources, waste of precious time, exposure to toxic effects of drugs and promotes the emergence of resistant bacteria. Wrong diagnosis and poor treatment were the main causes of complicated tonsillitis in this study. The main encountered complications were otitis media, peritonsillitis, and peritonsillar abscess. These are avoidable if accurate diagnosis and prompt treatment were instituted.
5. Conclusions
- In this study, tonsillitis was found to be common in all age groups and presents mainly with fever, sore throat, and tonsil enlargement. The condition is commonly misdiagnosed for other causes of fever and wrongly treated. The majority had recurrent tonsillitis and Staphylococcus aureus with Streptococcus species were isolated and sensitive to common antimicrobials. There were associated avoidable complications at presentation. Differentials of tonsillitis should be considered in patients with febrile illnesses.
Funding
- There was no financial support. It is a self-sponsored research study.