-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Surgical Research
p-ISSN: 2332-8312 e-ISSN: 2332-8320
2019; 8(2): 18-20
doi:10.5923/j.surgery.20190802.02

Successful Surgery of Penile Fracture with Severely Ruptured Tunica Albuginea During Sexual Intercourse: A Case Report
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbhishek Kumar, Snehlata
Vandana Nursing Home & Research Centre, Shivpuri, Hazaribag, Jharkhand, India
Correspondence to: Abhishek Kumar, Vandana Nursing Home & Research Centre, Shivpuri, Hazaribag, Jharkhand, India.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Penile fracture is a physiologically rare but clinically critical condition and requires earliest-cum-emergency urosurgical attention. Distinctive to the classic fracture, it is the traumatic tear and/or rupture of corpora cavernosa and tunica albuginea with or without disruptive injury to corpus spongiosum and urethra; a coordinating complex responsible for penile erection. However, severity, circumferences and extent of critical injury in penile fracture need to be examined and clinically confirmed on case by case basis. We, hereby, report a case of 38-year-old man who presented with acute penile pain, swelling, distortion of penis and sudden inability to sustain penile erection during normal coitus. Upon immediate urosurgical attention, we observed severely ruptured tunica albuginea and disrupted corpus cavernosum mediated penile fracture, which was adequately repaired by surgical management. In follow up the patient restored with physiological and void functions and regaining normal erectile function. In view of clinically critical and underreporting of cases, it is suggestive that prompt urosurgical intervention can preserve the psychological, urophysiological and reproductive functions to lead routine life with restored functions.
Keywords: Trauma to penis, Fracture Penis, Tunica albuginea, Corpora cavemosa
Cite this paper: Abhishek Kumar, Snehlata, Successful Surgery of Penile Fracture with Severely Ruptured Tunica Albuginea During Sexual Intercourse: A Case Report, International Journal of Surgical Research, Vol. 8 No. 2, 2019, pp. 18-20. doi: 10.5923/j.surgery.20190802.02.
1. Introduction
- A sudden unexpected accidental rupture of tunica albuginea and one or both of the corpora cavernosa complexes constitutes an entity called as the penile fracture. Although the most common cause is forced and violent sexual activity [1], other causes like an accidental injury during sleep are also known to cause this devastating injury. Prior infections or injuries in this region make the patient more prone especially if he is using performance-enhancing drugs. Along with penile fracture, corpora-spongiosal and urethral injuries are also said to exist [2]. The timely diagnosis followed by immediate surgical exploration and corporoplasty is the need of the hour in such condition [3]. Although, tunica albuginea has tensile strength and among the strongest fascia in human organs but at the same time quite prone to disruption, leading to penile fracture. One of the prominent plausible reasons for the increased risk of penile fracture is the coordinated working physiology of tunica albuginea during shaft erection. Precisely, it has been observed that tunica albuginea significantly elongates and becomes finer i.e. 0.25 to 0.5 mm during erection as compared to 2.4 mm in flaccid state. Bitsch et al. proposed that an intracorporal pressure of 1500 mmHg or more during erection can tear the tunica albuginea [4].The classic, "textbook" history of penile fracture is a sudden cracking sound as the tunica tears followed by pain, rapid detumescence, swelling and discoloration of the penis with or without voiding problems.
2. Case Report
- A 38 years male was brought by her wife to casualty in Vandana Nursing Home & Research Centre with complaints of pain and sudden detumescence of penis while performing coitus. Clinical examination revealed a swollen, flaccid, blackened penis deviated to one side [Figure 1] and there was severe tenderness on palpation. The urethral meatus was not bloodstained. A clinical diagnosis of fractured penis without any obvious urethral injury was made. The patient was immediately explored under anesthesia. A ruptured tunica albuginea was found which was about 10 x 8 mm in sized also near the right mid corpora cavernosa hematoma was seen to be localized [Figure 2]. The left corpora cavernosa and urethra appeared intact. A right corporal repair with inverted sutures of prolene 3-0 was performed. The patient was prescribed antibiotics and a prophylactic urethral catheter was kept for 14 days, which was subsequently removed. While on prescribed prophylaxis and upon discharge, patient was suggested to abstain from intercourse until complete healing and physiological comfort is attained for routine urological activity.
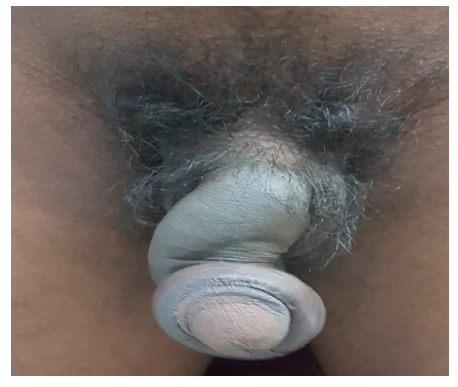 | Figure 1. Swollen and deformed fractured penis |
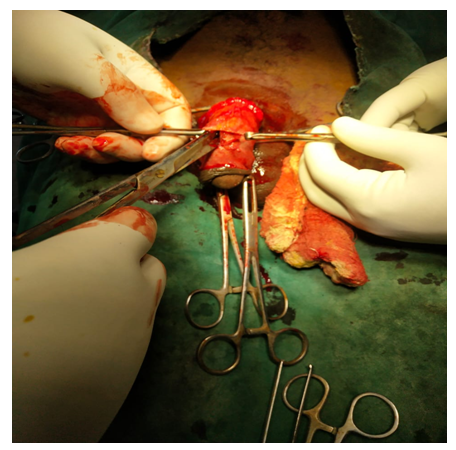 | Figure 2. Evacuation of hematoma revealing defect in right mid corpus cavernosum |
3. Discussion
- Normally inside the penile shaft, erectile tissues are arranged in columnar fashion. Dorsolaterally there are two corpora cavernosa and the ventromedially there is a corpus spongiosum, each enclosed in tunica albuginea. Ventral extension of the Buck`s fascia encloses the single corpus spongiosum whereas the dorsal one encloses the two corpora cavernosa. With sudden rise in the intra cavernosal pressure due to any extrinsic force the already thinned tunica albuginea of the erect penis gives away. Although, vaginal intercourse still remains the single commonest cause [5]; any activity carried in an erect state of the penis like masturbation, self-manipulation, sexual intercourse, rolling over in bed; can cause direct penile trauma and result in fractures. Pre-existing urethral or periurethral infections and injuries in this region increase the chances of penile fractures. Patients usually present with history that they heard or felt a sudden crack or snap-in penis, erection loss and swollen deviated painful penis. Usually only one side of the distal two-thirds of the penis is fractured and less than one-half of the cavernosal circumference is affected. Associated hematomas may be purely intracavernosal or extend to the perineum scrotum or even thighs. Associated urethral injury presents as hematuria or dysuria. A rare injury is bilateral penile fracture associated with urethral rupture following intercourse. It is believed that extreme reduction in the thinness of the corporal tunic (from 2 mm to 0.25mm) during erection and an intra-corporal pressure of at least 1500 mmHg predisposes it fracture [6]. Pre-existing local infections or injuries too are known to predispose to a tear in the buck’s fascia leading to a penile fracture on bending [7]. Particularly in this case, already available reports of various clinical investigations and preceding medication history of patients facilitated time management for earliest surgical intervention. Immediate exploration under anesthesia and repair of torn tunica after hematoma removal has been proved to be better than conservative measures [Figure 3]. This ensures quick recovery without any angulation deformity [8]. Thus, in today’s era with increased one-night stands and over the counter availability of performance-enhancing drugs, fracture penis no more remains a distant entity; but is now metamorphosing into a drastic reality. Hence, the entire medical fraternity must be aware of this entity so that it is diagnosed in time and treated appropriately at the earliest so as to ensure a better quality of life for the affected family. Innovative medical technology & health education is essential for patients so that diseases can be cured rather than be managed. [9]
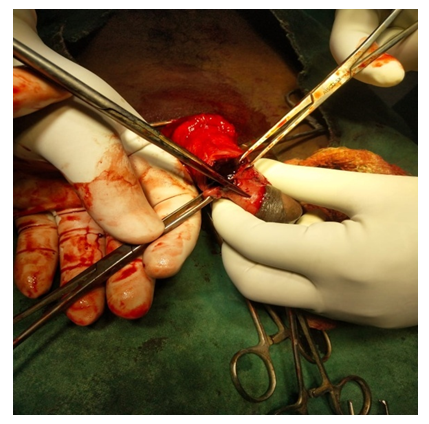 | Figure 3. Exposure of one of the fractured corpora cavernosa after penile degloving during surgical treatment |
4. Conclusions
- Penile fracture is a rare urological condition. Emergency surgical treatment can preserve voiding and sexual function.
Consent
- Written informed consent for publication of their clinical details and/or clinical images was obtained from the patient.
ACKNOWLEDGEMENTS
- The authors thank Dr. M Sohail for advice on this manuscript. Authors are also thankful to the supporting staffs of the centre.