-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Surgical Research
p-ISSN: 2332-8312 e-ISSN: 2332-8320
2018; 7(1): 7-11
doi:10.5923/j.surgery.20180701.02

Risk Factors and Complications for Anorectal Abscess in Sudanese Patients: A Case-Controlled Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLWalid Elhaj Abdelrahim 1, Ali Yasen Yasen MohamedAhmed 2, Kateera Abdl Wahab Ahmed Mohamed 2, Salma Saeed Sulaiman Mohammed 2, Kamal Elzaki Elsiddig 1, Eltahir Awad Gasim Khalil 3
1Department of Surgery, Faculty of Medicine, University of Khartoum, Khartoum, Sudan
2Sudan Medical Specialization Board, Khartoum, Sudan
3Department of Clinical Pathology & Immunology, Institute of Endemic Diseases, University of Khartoum, Khartoum, Sudan
Correspondence to: Walid Elhaj Abdelrahim , Department of Surgery, Faculty of Medicine, University of Khartoum, Khartoum, Sudan.
| Email: |  |
Copyright © 2018 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

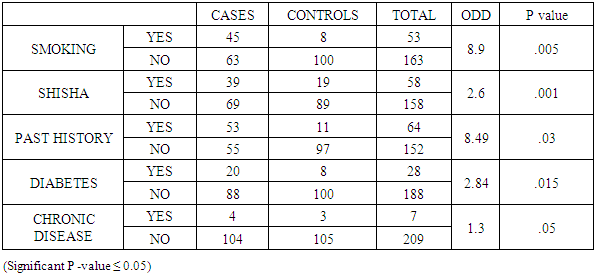
Background: Acute sepsis in the region of the anus is common and important clinical and surgical problem. The objective of the study was to study the risk factors and complications of anorectal abscess in Khartoum state. Patients and methods: This was hospital based, retro-prospective, case control and multicenter study was done in Khartoum state public teaching hospitals. All patients underwent perianal abscess drainage in the selected hospitals during the study period were included and matched with control group who never diagnosed with anorectal abscess. 108 patients were included as cases and 108 as control group. Results: Gender distribution was the same in both groups. Considering risk factors, the study showed that Shisha smoking (P value = .001), cigarette smoking (P value = .005), diabetes (P value = .015), past history of anorectal abscess (P value = .03) all statistically significant as risk factors for developing anorectal abscess. We observed that, in the case group 94% of patients presented by anal pain, 62% by indurated mass and 43% by fever. Regarding abscess type, perianal abscess form 58% of types, while other types like isciorectal, submicosal and intersphiteric form the remaining 42%. Regarding Complications, 20.4% develop Fistula and 15.7% of cases complicated by recurrence of the abscess. Sixteen percent of cigarettes smokers suffered from abscess recurrence (7/45) and a high rate (8/39) 21% was seen in Shisha smokers group, while a much higher rate (9/20) 45% was observed in diabetic patients. In this study only cigarettes smoking is statistically significant for abscess recurrence (p value 0.04). Conclusion: The main risk factors for developing anorectal abscess is smoking either cigarette or shisha, cigarette smoking is the main cause of complications, and the most common presenting symptom is anal pain.
Keywords: Anorectal abscess, Cigarette smoking, Fistula, Diabetes
Cite this paper: Walid Elhaj Abdelrahim , Ali Yasen Yasen MohamedAhmed , Kateera Abdl Wahab Ahmed Mohamed , Salma Saeed Sulaiman Mohammed , Kamal Elzaki Elsiddig , Eltahir Awad Gasim Khalil , Risk Factors and Complications for Anorectal Abscess in Sudanese Patients: A Case-Controlled Study, International Journal of Surgical Research, Vol. 7 No. 1, 2018, pp. 7-11. doi: 10.5923/j.surgery.20180701.02.
Article Outline
1. Introduction
- Anorectal abscess defined as the presence of a firm or fluctuant tender mass located close to the anus. Anorectal abscess and fistula are among the most common diseases encountered in adults. [1] Most perianal abscesses arise from the occluded duct of an anal gland with subsequent bacterial overgrowth and abscess formation [2, 3]. Infection usually caused by, an aerobic and anaerobic polymicrobial infection. Bacteroides fragilis is the predominant anaerobe. Other common bacteria include Escherichia coli and those of the genera Proteus, Bacteroides, and Streptococcus. Sources of bacteria are skin, bowel, and, rarely, the vagina [4].We designed this study to look into different risk factors for developing anorectal abscess as well as to factors that might be associated with complicated outcome.
2. Patients and Methods
- Our study is retrospective observational case-control study, in which 216 subjects in Khartoum state public teaching hospitals during the period of April 2016 till April 2017 were included. Volunteers were divided into two groups, a control group and a case group, each group composed of 108 volunteer. All subjects were given questions about smoking history and habits, diabetes, chronic illness and previous episodes of anorectal sepsis. Follow up for complications up to the third month after abscess drainage was done through telephone interview. Data were subsequently analysis using SPSS.
3. Results
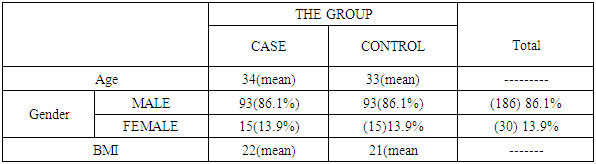
- Two hundred and sixteen men and women were included in this study, (186/216) (86%) were males and (30/216) (14%) were females with a mean age of 33.7±10.7 years with a range of (23 – 34) years. Both Groups were comparable regarding other characteristics (Table 1). Perianal abscess were the most common Varity (58%) in our study (Figure 1). We observed that, in the study group 94% of patients presented with anal pain, 62% with indurated mass and 43% had accompanying fever (Figure 2). Moreover only 10% of cases have a previous episode of anorectal sepsis.
|
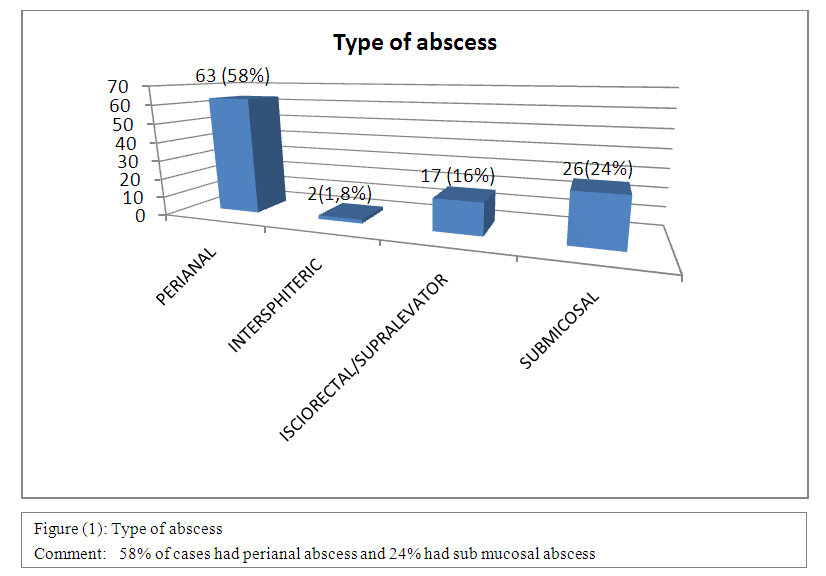 | Figure 1. Showed Type of abscess among cases group |
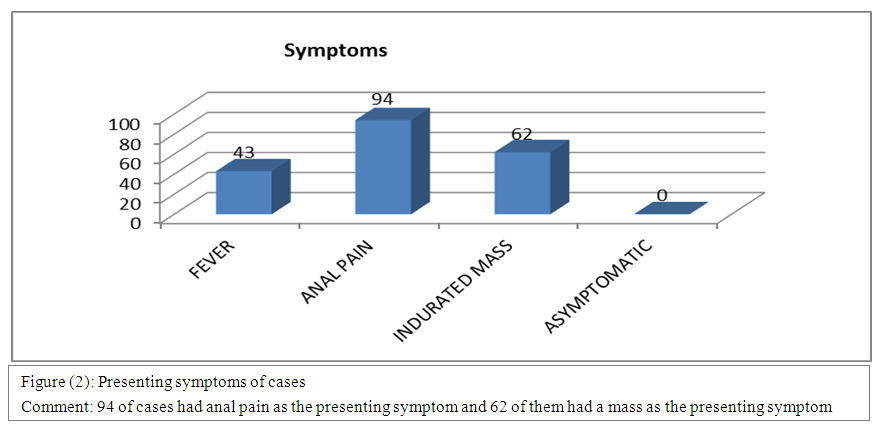 | Figure 2. Showed presenting symptoms among case group |
|
|
|
|
4. Discussion
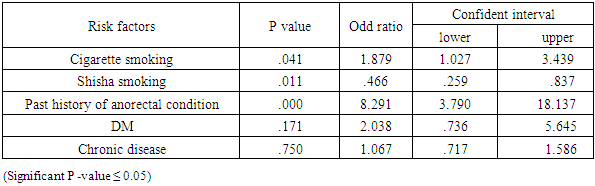
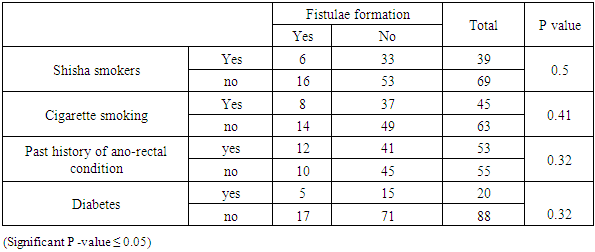
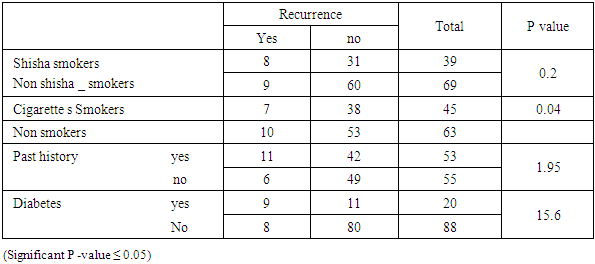
- Anorectal abscess is one of the most common diseases among adults, a fact that was demonstrated by this study as the mean age of cases was 34 years with standard deviation of 12.9 range between (21.1 _ 46.9) years. male: female ratio among study group was 6:1 this similar to the literature which demonstrated that anorectal abscess is more prevalent in males, also consistent with study done in Omdurman teaching hospital in 2011 with a male to female ratio of 5:1. [5] This may be due to cultural factors that females prefer to go to private clinics or hospitals when the medical problem related to sensitive areas.The main presenting symptom in our study was anal pain (n = 94) followed by anal mass (n = 62), this reported also by Mehmet. U et al with the anal pain and swelling as the most clinical symptoms [6], also consistent to study done by Saadeldin which reported that anal pain was the presenting symptom in 95% of patients. [5] In our study the perianal abscess was the most common type encountered among cases (58%) followed by the submucosal abscess (24%), this different from the results reported by Mehmet. U et al, with the 38% of cases had intersphinectric abscess followed by the perianal abscess 25%. [6]A study done by Bikash. D et al [7], concluded that smoking is a risk factor for developing anal abscess with an odd ratio of 2.15 between cases and controls (p = 0.0025), this similar to our findings with an odd ratio of 8.9 (p = 0.005), this means that smokers are eight times more susceptible to develop anal abscess than nonsmokers. No previous study proposed shisha smoking as a risk factor for anal abscess, but in our study we found that odd ratio of shisha between cases and controls is 2.6 which mean that shisha smokers are two times have the tendency to develop abscess than the non-shisha smokers with a significant p value of (0.001), this may be explained by that shisha smoking has the same pathological effect of cigarette smoking and also the majority of shisha smokers are cigarette smokers are also.Diabetes has been previously implicated as a risk factor for anal abscess, as the study done by Mehmet. U et al that found 22.2% of its cases were diabetics and study done by Bikash. D et al [7] with 20% of cases had diabetics, this almost similar to our results as 19% of our cases were diabetics, but this is far different from the results of study done by saadeldin. A et al [5] where only 8.1% were diabetics. Our study found that the odd ratio of diabetes is 2.8 (p = 0.015).The theory that anorectal abscess developed as a result of nonspecific cryptoglandular infection put for the first time in 1878 [4], apart from this theory other specific factors had been identified such as inflammatory bowel disease, tuberculosis, malignancy and other immunosuppressive diseases [8], our study didn’t revealed this relationship between those chronic diseases and anorectal abscess as only 4% of our patients had chronic diseases The study found that only 4% of cases have a chronic disease this similar to study done by Nezih. A et al, which found that this rate is only 11.8%. [9]The study revealed a total of 39(37%) case of complications, 22(20%) developed a fistula and 17(15%) had a recurrence of abscess. This similar to study done by Takaaki. Y et al in 2010 [10] which concluded that 20% of their patients developed anal fistula and 16% developed recurrence and consistent with the results obtained by Mehmet. U et al with 27% of their cases developed fistula [6], but this different from those obtained from Saadeldein A. [5] which reported that only 6 cases developed fistula and only 7 cases had a recurrence of abscess and different to results reported by Herand. A [11] with only 8.6% of cases developed fistula this may be due to difference in risk factors and difference in the follow up period between those studies.The mean BMI of cases was 22 with standard deviation of 3.5 range between (19.5 _ 25.5.) in our study BMI of more than 30 wasn’t associated with fistula formation, instead associated with fistula formation (relative risk = 1.3, attributable risk = 25%). BMI > 25 (overweight) is a risk factor for fistula formation (relative risk = 1.3, attributable risk = 25%) also for recurrence of abscess (relative risk = 1.3, attributable risk = 25%), those results are different from study done by Takkai [10] which concluded that there is no significant effect of BMI on complications of abscess drainage.When we analyzed smoking as a risk factor for developing complications, we found that smoking can be a risk factor for recurrence of abscess (p = 0.04) but not a risk factor for fistula formation (p = 0.41) which may mean that smoking in the first place is a major risk factor for developing an abscess it contribute largely to its recurrence. The study that conducted by Monfrecola G concluded that Smoking decreases the cutaneous blood flow [12] and another study done by A. F. J. De Bruin prove the rectal mucosal perfusion was found to be significantly lower in smokers [13]; these two studies support our result in that smoking is a major risk factor for anorectal abscess and its recurrence.The study found that the other risk factors like chronic disease, diabetes mellitus, shisha smoking and past history of anorectal abscess has no effect in developing complications.
5. Conclusion and Recommendations
- The main risk factors for developing anorectal abscess is smoking either cigarette or shisha, cigarette smoking is the main cause of complications, the most common presenting symptom is anal pain so clinician should think in anal abscess in any case presenting with pain. Anorectal abscess can be added to the list of inflammatory diseases that has strong association with smoking. This study should followed by other longer period case control studies and cohort study in more representative population in order to know the other risk factors and in which the association between smoking and Anorectal abscess could be tested prospectively. Meanwhile we have another associated disease to encourage people to quit smoking.