-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Surgical Research
p-ISSN: 2332-8312 e-ISSN: 2332-8320
2016; 5(2): 17-20
doi:10.5923/j.surgery.20160502.02

Torsion of the Vascular Pedicle of a Wandering Spleen in Three Young Men: Diagnosis and Surgical Treatment
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAlpha Oumar Touré, Abib Diop, Ibrahima Ka, Ousmane Thiam, Mohamadou Lamine Gueye, Mamadou Seck, Mamadou Cissé, Ousmane Ka, Madieng Dieng
General Surgery Department, A. Le Dantec Hospital, Dakar, Senegal
Correspondence to: Alpha Oumar Touré, General Surgery Department, A. Le Dantec Hospital, Dakar, Senegal.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The twist of the elongated splenic pedicle of a wandering spleen, a rare anatomical entity characterized by its migration from left hypochondria to an anormal position in the abdomen or pelvis, can lead to spleen ischemia, infarction and necrosis. We report the cases of three young men with intestinal occlusion associated to abdominal mass. Preoperative medical examinations showed the torsion of the vascular pedicle of the wandering spleen. In one case there was a situs ambiguous with the liver sited into left hypochondria. Splenectomy was successfully performed in all patients. In one case a sigmoidoresection with double colostomy was realized.
Keywords: Wandering spleen, Splenectomy
Cite this paper: Alpha Oumar Touré, Abib Diop, Ibrahima Ka, Ousmane Thiam, Mohamadou Lamine Gueye, Mamadou Seck, Mamadou Cissé, Ousmane Ka, Madieng Dieng, Torsion of the Vascular Pedicle of a Wandering Spleen in Three Young Men: Diagnosis and Surgical Treatment, International Journal of Surgical Research, Vol. 5 No. 2, 2016, pp. 17-20. doi: 10.5923/j.surgery.20160502.02.
1. Introduction
- The wandering spleen is a rare anatomical congenital entity [1, 2]. Clinical signs are often poor and it's, therefore, discovered incidentally in most cases. The twist of the splenic pedicle is a serious complication that needs to be managed quickly to avoid radical surgery, especially in young patients. We report 3 cases of wandering spleen torsion managed in the General Surgery Department of the Aristide Le Dantec Hospital of Dakar and Regional Hospital El Hadji Ibrahima Niass of Kaolack in Senegal (West Africa). The aim of our study is to describe these cases and make a review of the literature.
2. Cases Report
- Case 1A17 years-old man was admitted at the surgical department of the Aristide Le Dantec Hospital for acute gastric pain evolving from 15 days. The patient, in good general condition without hyperthermia, presented at clinical examination anemia and an epigastric mass, which was sensitive and slightly mobile to palpation.
The blood cell count showed moderate leukocytosis (10,940/mm3), anemia with a hemoglobin level of 8 g/dL and platelets at 201 400/mm3. Fibrinogen was 4.79 g/l and CRP was negative.Abdominal ultrasound had revealed ectopic spleen in epigastric position with a subcapsular hematoma. Abdominal CT scan showed an ischemic spleen in ectopic epigastric position as shown in Figure 1.
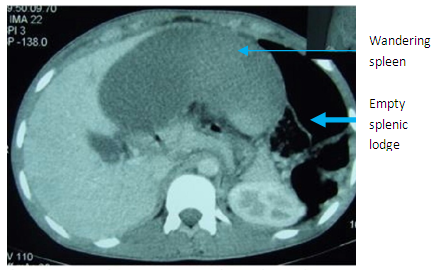 | Figure 1. Abdominal CT-scan showing a wandering spleen and empty splenic lodge (Photo Dr Touré) |
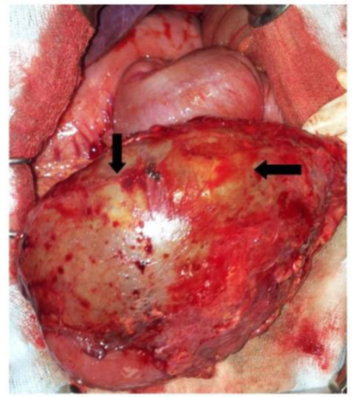 | Figure 2. Splenomegaly with necrosis areas (arrows) (Photo Dr I.Ka) |
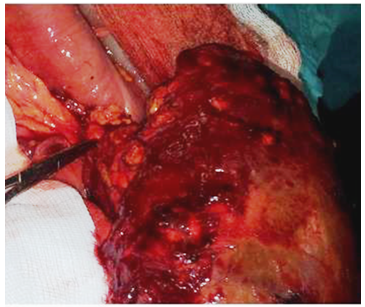 | Figure 3. Splenic pedicle torsion (Photo Dr I. Ka) |
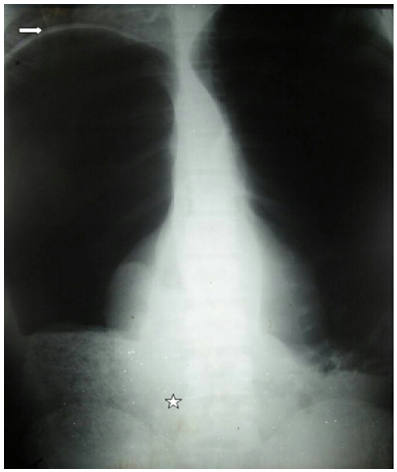 | Figure 4. Plain abdominal X-ray. Bowel dilatation reaches the diaphragm (arrow) with air-fluid levels. Absence of liver silhouette in the right upper quadrant. A spleen-like mass silhouette is seen in the lower middle quadrant (star), between the two iliac crests |
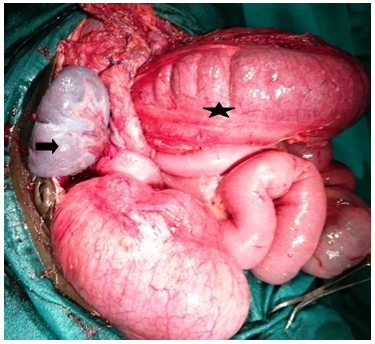
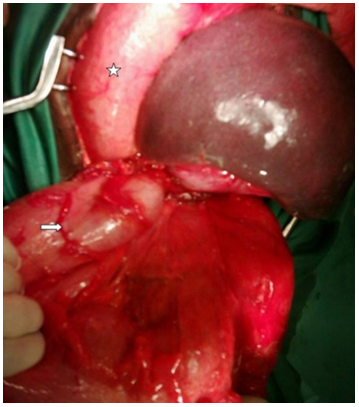 | Figure 5. Operative findings. Torsion of the pedicle of a wandering enlarged spleen around the sigmoid (arrow). Dilatation of the proximal part of the colon (star). The spleen has not any ligamentous attachments |
 | Figure 6. Situs ambiguous with liver in the left hypochondrium. The liver presents a complete agenesis of the right lobe. The gallbladder (arrow) is retrohepatic, in the extremity of the lateral segment of the liver |
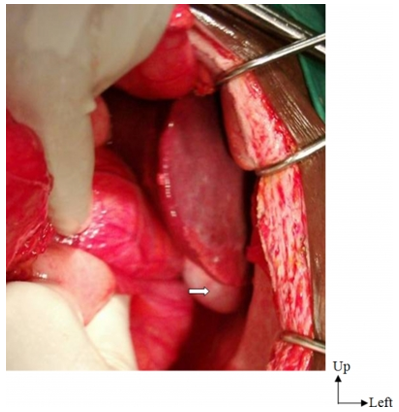
 | Figure 7. Splenic pedicle torsion in right upper (arrow) with colonic dilatation (star) (Photo Dr A Diop) |
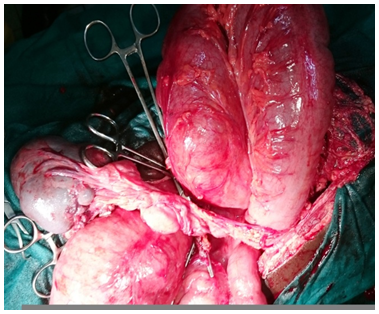 | Figure 8. Wandering spleen with long pedicle (Photo Dr A Diop) |
3. Discussion
- This is a rare anomaly that can be observed at all ages and in both genders with a predilection for boys under 10 years [3]. However, a few cases have been reported in women of childbearing age and in the elderly [4]. The incidence is less than 0.5% from a wide series of splenectomy. [5]. When congenital, wandering spleen is linked to a lack of attachment to the intestine back in the 2nd month of embryogenesis [1]. And the posterior midgut fails to merge with the posterior peritoneum leading to an absence of ligaments which ensure the fixity of the spleen. The existence of an ectopic spleen, added to a long pedicle and splenomegaly (frequent in our tropical countries with endemic malaria) could promote volvulus by the absence of splenic fixing system as in our patients [6-8]. Wandering spleen may be asymptomatic and only discovered incidentally, during a routine examination or during imaging for some other pathology [9]. It can also be discovered during complications such as an intestinal occlusion due to strangulation by the splenic pedicle as 2 of our patients [10]. Symptoms are variable and often poor, with a long latency period: more or less intense pain in the left upper quadrant, the discovery of splenomegaly or compression of a neighboring organ [11]. The twist is favored by its mobility, its weight and the length of its pedicle. It can sometimes be irreversible and present with a picture of acute abdomen with abdominal pain associated with nausea, vomiting, and fever [1]. In our observations, symptomatology was dominated by the occlusive syndrome. Mobile and painful abdominal or pelvic mass should be sought by palpation of the abdomen. This clinical picture may suggest the diagnosis of ectopic splenic torsion, but it will nevertheless rule out other diagnoses such as adnexal torsion or volvulus of small bowel tumors [1].The abdominal and pelvic ultrasound can confirm the diagnosis of torsion of ectopic spleen before the emptiness of the splenic lodge and the highlight of an abdominal mass recalling the spleen structure splenic; lack of vascularisation at ultrasound Doppler is suspected for spleen twisting [12, 13].Abdominal contrast-enhanced scan is the reference. It confirms the diagnosis by showing an empty splenic lodge with an abdominal mass or abdominal pelvic recalling the appearance of the spleen and not taking contrast after intravenous injection. [14] The twisted pedicle can be seen as a "whirlpool". [13]What to do is usually dictated by the surgical exploration. The treatment is surgical laparotomy or laparoscopy. The midline laparotomy provides good exposure. In the absence of splenic necrosis, untwisting associated with splenopexy, allow binding of the spleen in its anatomical position. It will be sutured to the diaphragm and to the front wall via a resorbable prosthesis [15-17]. If necrosis and due to the risk of recurrent twisting, the indication is splenectomy as advocated by many authors [18, 19]. All our patients received a total splenectomy after untwisting although two of our patients presented viable spleen. It’s due to recurrent unavailability of prothetic mesh for splenopexy.
4. Conclusions
- The wandering spleen torsion is a rare anatomical entity whose symptoms are not very specific. Abdominal imaging including abdominopelvic CT scan plays a major role in the diagnosis. It allows an adapted surgical management.