-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Surgical Research
2015; 4(2): 15-18
doi:10.5923/j.surgery.20150402.02
Comparative Study between Two Types of Implants Supporting Mandibular Overdenture
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMohammad M. Beyari
Department of Oral and Maxillofacial Surgery & Rehabilitation, Prosthetic Branch, Faculty of Dentistry, Umm Alqura University, Makkah, KSA
Correspondence to: Mohammad M. Beyari, Department of Oral and Maxillofacial Surgery & Rehabilitation, Prosthetic Branch, Faculty of Dentistry, Umm Alqura University, Makkah, KSA.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
This study was performed to compare between two types of implants supporting overdentures, Mini dental implants, ball type single piece implant and screw type tapered root form implants surgically placed in the canine regions bilaterally. Methods: Fourteen completely edentulous patients received two implants in the canine region were divided into two groups, seven each. The first received screw type tapered root form implants surgically placed and loaded 3 months thereafter with ball attachment. The second received ball type 2.8mm single piece implants loaded 3 months thereafter. All patients have been evaluated for bone density and bone height changes around the implants at 0, 6 and 12 months after loading. Results: Comparing the two groups throughout the whole study period, there was no statistically significant difference between them regarding the effect of treatment. Conclusions: Within the limitation of this study, the two types of implants had the same effect on the response of the alveolar bone surrounding the implant.
Keywords: Complete denture, Overdenture, Implant supported overdenture, Implant retained overdenture, Ball attachment, Single piece implant
Cite this paper: Mohammad M. Beyari, Comparative Study between Two Types of Implants Supporting Mandibular Overdenture, International Journal of Surgical Research, Vol. 4 No. 2, 2015, pp. 15-18. doi: 10.5923/j.surgery.20150402.02.
Article Outline
1. Introduction
- Alveolar bone loss under complete dentures is evident [1-3]. Overdenture concept was introduced as an alternative [4] and the procedure is accepted as a definitive method of treatment [5]. To improve support and or retention of the removable prosthesis, implants are advocated [6] and minimal number of implants are used [7-9].The condition of alveolar bone surrounding the abutments teeth was studied in tooth supported overdentures where Radiographic evaluation of the condition of alveolar bone is done using special film holder to render the procedure reproducible, it was found that alveolar bone distal to the abutments teeth was preserved [10].Implant retained/supported mandibular overdentures have saved many problems for complete denture patients and allowed authors to consider it as the quality of standard for the edentulous patient [11].The one surgical stage implant design; transgingival, is inserted into the bone where its abutment penetrates the oral mucosa without micro gaps between the abutment and the implant inside the tissues [12, 13]. The purpose of this work is to compare between the supporting structures of the two types of implants under mandibular overdenture.
2. Materials and Methods
2.1. Patients Selection
- Fourteen completely edentulous patients were selected from the clinic of Faculty of Dentistry, Umm Alqura University to participate in this study. The patients had an average age of 52 years. They should be free from any systemic disease that may interfere with dental implant placement and / or osseointegration e.g. uncontrolled diabetes, hypertension, blood diseases, bone diseases….etc. All the patients should have Class I jaw relationship and adequate inter-arch distance [14].An upper arch of moderate size and a lower arch showing flat to moderate size ridge. Patients showing gagging reflexes, parafunctional habits and heavy smokers were excluded from the study. Only cooperative patients following instructions and having proper neuromasculer co-ordination were included in the study.Selection criteria were verified by thorough patient history and clinical examination, as well as radiographic assessment by 1:1 panoramic radiographs to assess the available bone quantity corresponding to the proposed implant sites.
2.2. Denture Construction
- All the complete dentures were constructed according to the standard technique followed at the Faculty of Dentistry, Umm Alqura University. The finished lower denture was duplicated for each patient and processed in clear acrylic resin in order to construct a surgical guide template, and then it was finished, polished and checked in the patient’s mouth for correct seating.At the delivery appointment, final occlusal adjustments and refinements were done and the denture was delivered to the patients to get used to it. The denture was inspected few days later in order to perform any required adjustments before the surgical appointment.About 4 mm depth cavity was done in the fitting surface of the surgical template in the site corresponding to the area between the 1st and 2nd premolars and was filled with amalgam filling material as a radio- opaque material to help in the proper assessment of the location of the mental foramina relative to the teeth of the template guided by digital panoramic radiograph. Holes were then drilled at the chosen implant sites in order to facilitate implant placement during surgery.
2.3. Grouping
- Patients were randomly divided into two groups according to the type of implant placed in the canine region bilaterally. Group I consisted of 7 patients to receive two screw type tapered root form implants (Legacy, Spectra system, Implant Direct, U.S.A.) while Group II consisted of 7 patients to receive two ball type 2.8mm single piece implants (Mini Implants, OsteoCare™ Implant System Ltd. Berkshire, UK).
2.4. Implant Placement
- Two screw type tapered root form implants (Legacy, Spectra system, Implant Direct, U.S.A.) were surgically placed bilaterally in the canine regions for Group I patients following a 2 stage surgical technique, their implants were exposed after three months and stud attachments were installed and dentures adjusted (Figure1).
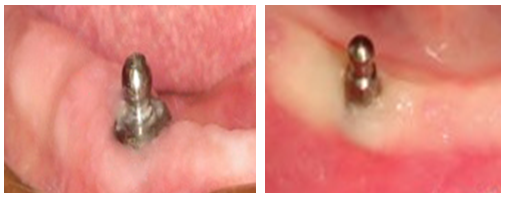 | Figure 1. Left the ball attachment, Right the mini implant |
2.5. Radiographic Evaluation
- All patients have been radiographically evaluated at the time of loading (base line), 6months and 12 months thereafter. Standardized periapical radiographs were achieved through the use of digital periapical radiography (Digora system, Soredex-Finndent, Finland) with paralleling technique utilizing a specially designed radiographic guide for this purpose. The specially designed radiographic guide represents a simple modification of an L shaped bite block (XCP Instrument, Dentsply Rinn Corporation, USA). The modification was done by attaching the green snap-on mount transfer of the implant to the L shaped bite block by means of a self-curing acrylic resin in such way that the transfer is brought parallel to the film holding part of the bite block. The exposure protocol starts by the removal of the abutments from the implant using the torque wrench. Then the bite block with the image plate was snapped on the implant. The indicator arm and the aiming ring were then assembled to the bite block. The patient was asked to close on the bite block to avoid its movement during cone adjustment. Radiographs were recorded, all with the same radiographic machine and exposure parameters. The radiographs were compared with regard to the marginal bone height and density.
3. Results
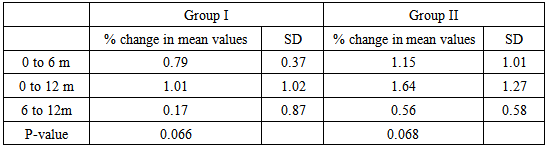
3.1. Relative Bone Density
- The mean values of relative bone density changes in both groups (I) and (II) showed no statistically significant difference during the follow up periods(P <0.05).The relative bone density changes around the implants showed no statistically significant difference between the two groups during the follow up period (P > 0.05) table 1.
|
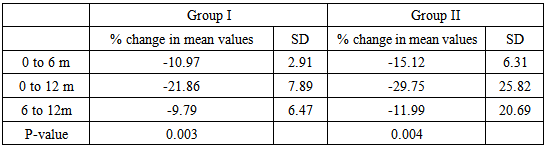
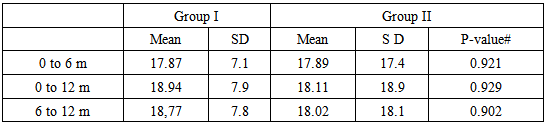
3.2. Bone Height Changes
- The mean values of bone height changes percentage in both groups I and II showed statistically significant difference during the follow up periods (P <0.05) table 2, while the bone height changes around the implants showed no statistically significant difference between the two groups during the follow up period (P > 0.05) table 3.
|
|
4. Discussion
- Lateral load is claimed to have more deleterious effect on dental implants than vertically applied load [15]. Despite the difference in design of the two implantsused in the two study groups, there was no statistically significant difference in bone changes (height and density) between both groups. This may be attributed to 1) The difference in height may be not enough to induce significant increase in the lateral load, 2) The two implant abutments used permit a universal movement and stress breaking action by virtue of their design and resiliency thus allowing the ridge to bear most of the load. 3) The single piece implant has no micro gap and the two piece implant when done with accuracy [16] seems to have no difference; however, it wasn’t investigated in this study.Although it was reported that a major advantage of implant supported prosthesis is that the abutments cannot decay, but on the other hand many mechanical complications have been encountered from the retentive attachments of implant supported prosthesis as looseness, fracture and wear of the attachments [17]. None of these complications was encountered in this study. This may be explained due to the short period of the study.The delayed loading to the mandibular implants after 3 months allows for better osseointegration [18] that is why it was chosen in this study and may explain the results.
5. Conclusions
- Within the limitations of this study, the two implant designs used to retain mandibular overdenture prostheses had the same effect onthe response of the alveolar bone surrounding the implant.