-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Surgical Research
2014; 3(2): 27-30
doi:10.5923/j.surgery.20140302.03
Treatment of Paediatric Varicocele: A Research for the Best Method
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLG. Bolla
Department of Pediatric Urology, O.C. Dolo, Venice, Italy
Correspondence to: G. Bolla, Department of Pediatric Urology, O.C. Dolo, Venice, Italy.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
The research for the best method to treat paediatric varicocele is still troublesome. The high surgical ligature of the spermatic vessels – according to Palomo - and the antegrade sclerotherapy - according to Tauber – represent, up to now, two confirmed therapies. This paper analyzes the best therapeutical technique and the best operation timing; moreover, it analyzes the results relative to the relapses.
Keywords: Paediatric varicocele, Surgical ligature, Antegrade sclerotherapy
Cite this paper: G. Bolla, Treatment of Paediatric Varicocele: A Research for the Best Method, International Journal of Surgical Research, Vol. 3 No. 2, 2014, pp. 27-30. doi: 10.5923/j.surgery.20140302.03.
1. Introduction
- Varicocele is a physical abnormality found in the 11% of adult males [1, 2] and in the 25% of those with abnormal semen analysis [3]. Varicocele is a meshwork of distended blood vessels in the scrotum - usually on the left-side - due to dilatation of the spermatic vein. Although the concept that varicocele causes male subfertility has been around for more than 50 years, the mechanism by which varicocele would affect fertility is not yet clear. Therefore there isn’t any sufficient evidence to explain the mechanisms by which varicocelectomy would restore fertility. Furthermore, it has been questioned whether it exists a cause at all between the distension of the pampiniform plexus (a network of many small veins found in the human male spermatic cord) and impairment of fertility. The therapeutic approach for adolescent varicocele remains that of the patient to undergo several treatments, to be compared according to safety and effectiveness [4]. This study evaluates two different patterns of paediatric varicocele treatments: the varicocelectomy according to Palomo [5] versus the antegrade method of the sclerotherapy according to Tauber [6]. We wanted to compare the safety and effectiveness of these two treatments, especially in the presence of relapse of the varicocele.
2. Methods
- From June 2007 to May 2013 one hundred boys suffering for left idiopathic varicocele (second-third degree) were included in our therapeutic study: the diagnosis of varicocele was made by clinical examination and was confirmed by Color Doppler analysis; 50 boys were treated by surgical ligature of spermatic vessels through an access just above the inguinal channel (Fig. 1) and the remaining 50 by antegrade sclerotherapy performed with an injection into a vein of the spermatic cord at the apex of the scrotum – after the phlebography - of 1% Lauromacrogol 4 ml. (Fig. 2) (mean age 12,3 years and 13,3 years). Study occurred after having previously obtained the informed consent from the parents and the ethics approval according to Helsinki Declaration. The patients have been randomly selected; however, the previous clinical outcome (absence of relapse for the boys who have undergone the operation) allowed us to prefer the surgical therapy for the boys with testicular hypotrophy. All the boys were subjected to spinal anaesthesia. In the first group twelve boys showed testicular hypotrophy, eight of them in the second one (Fig. 3). The average operation time was 19’ for the first group, 27’ for the second (Fig. 4); average follow-up was 22,18 m. and 19,14 m. respectively. The follow-up was carried out 3 and 12 months after treatment.
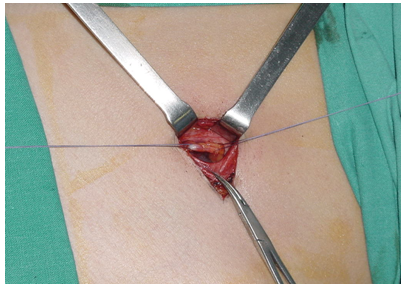 | Figure 1. The surgical ligature of spermatic vessels |
 | Figure 2. The injection into a vein of spermatic cord for antegrade sclerotherapy |
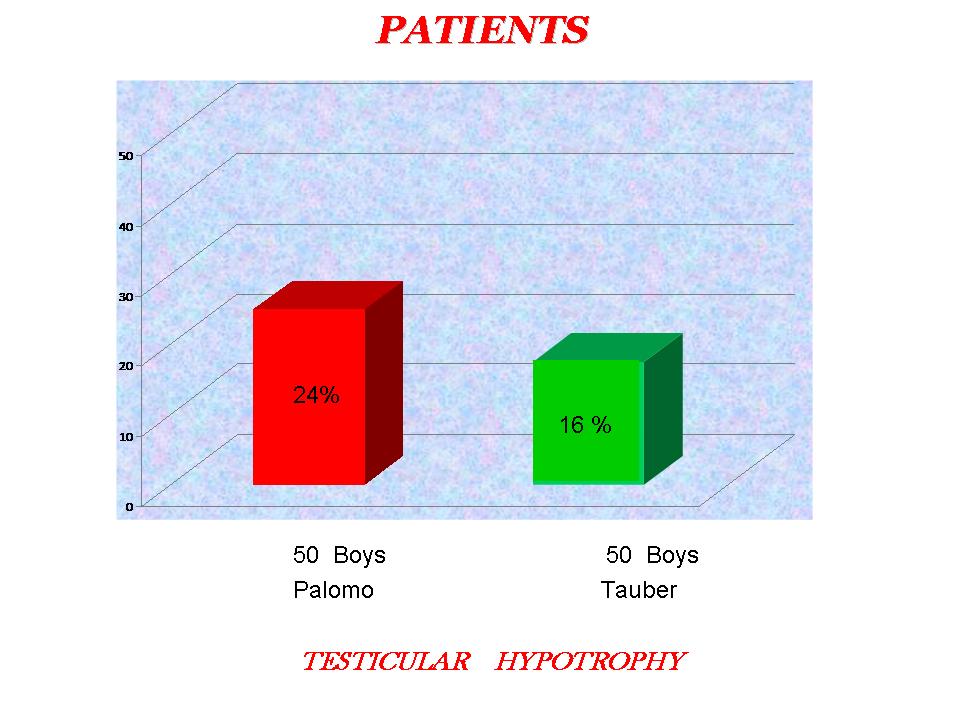 | Figure 3. The incidence of testicular hypotrophy |
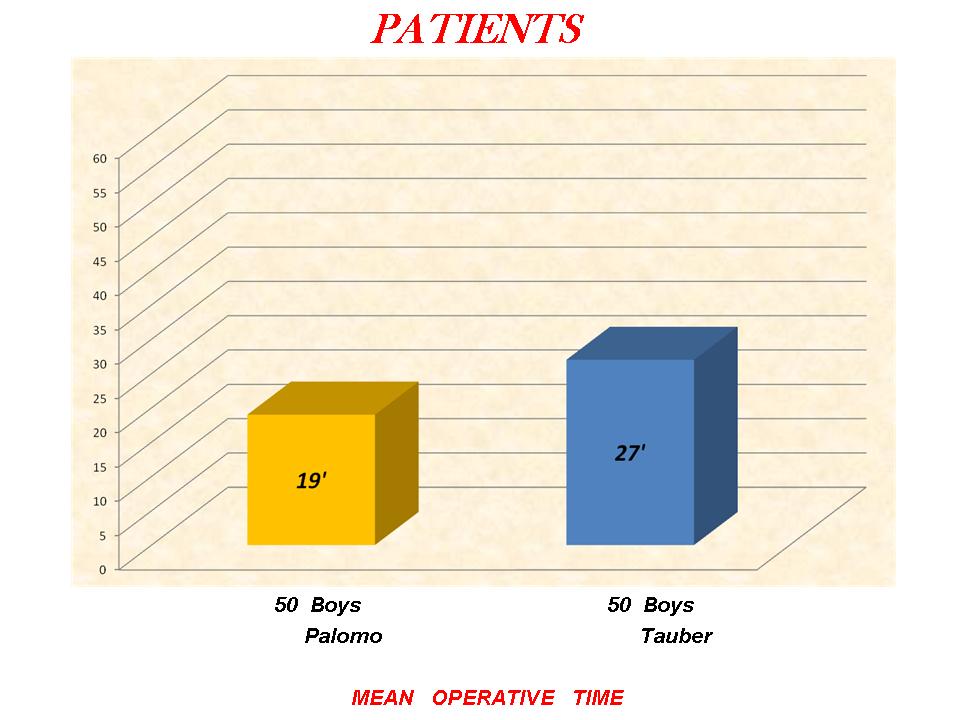 | Figure 4. Mean operative time |
3. Results
- We haven’t found any relapses of the varicocele within the first group (Palomo method). The group treated by sclerotherapy showed from a 6% incidence of relapse (all the relapses were noticed at first post-operative check-up: this aspect seems to show the recovery being unsuccessful since the start and therefore, consequently the inadequacy of the technique). Three boys treated by surgical ligature have produced a left hydrocele and three boys treated by sclerotherapy showed a modest haematoma into the spermatic cord.
4. Discussion
- There is a clear variability on treatment of paediatric varicocele, still now [7, 8]. This aspect indicates an uncertainty about the therapeutical approaches to the problem. The variability regards both the surgical treatments (like the ligature of the vessels or the veins on a different level and like the various vascular anastomoses) and the other therapies (antegrade or retrograde sclerotherapy, retrograde embolisation) [9, 10]. In our opinion the treatment of paediatric varicocele ought to be done at the first diagnosis, in order to prevent a possible future infertility [11, 12] thus allowing the regular testicular growth [13, 14]. Unavoidably for adolescents the functional fertility evaluation is not possible, for ethical reasons and physical ones (hormone release). The clinical samples, in our experience, were too little to draw a significant statistic, but the trend related to the comparative frequency (Boole function) of relapse in two groups of therapy has been definite. In paediatric age we believe that spinal anaesthesia is proved to be more effective in the sclerotherapy: the boy gets excellent pain suppression without the need of an additional use of sedative drugs; with local anaesthesia instead the injection of anaesthetic drug into the spermatic cord (immediately before the sclerotherapy) can be troublesome. The antegrade sclerotherapy showed an appearance of relapse, although restricted. In conclusion, the laparoscopic approach requests a triple access, a general anaesthesia and it involves a longer operation time than the open surgery [15].
5. Conclusions
- The surgical open ligature shows, by these preliminary compared data, to be an effective treatment method [16, 17], with a short operation time and without evident complications.
ACKNOWLEDGEMENTS
- Best greetings to my teacher of Surgery, Prof. Giampiero Belloli, and to my son Alberto, experienced in Statistics.