-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Surgical Research
2014; 3(1): 15-18
doi:10.5923/j.surgery.20140301.03
V-Y Advancement Flap for Reconstruction of Defects after Excision of Basal Cell Carcinoma of the Face
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLWaleed Elnahas1, M. T. Hafez1, Reda A. Younis2, Loai Elbassiony2, Mohamed A. Hegazy1
1Surgical Oncology Unit, Mansoura Oncology Center, Mansoura University
2Plastic Surgery Department, Mansoura University
Correspondence to: Waleed Elnahas, Surgical Oncology Unit, Mansoura Oncology Center, Mansoura University.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Background: Basal cell carcinoma (BCC) is the most common skin cancer. After excision of BCC on the face, the options of treatment for a skin defect are variable. Many surgeons prefer to use a local flap rather than a skin graft or free flap for small- or moderately-sized circular defects. We have evaluated the versatility of V-Y perforator flap for reconstruction of skin defects after excision of BCC of the face. Methods: All of the patients were pathologically diagnosed with basal cell carcinoma (BCC), Thirty-seven patients underwent V-Y advancement flap repair over the period between September 2011 and May 2013. We evaluated the postoperative complications in the form of flap loss either partial or complete, wound dehiscence, hematoma, seroma and wound infection. The cosmetic outcome and patient satisfaction was evaluated at 6 months after surgery. Results: There were 30 men and 7 women. The ages ranged from 51to 69 years with a mean age of 60 years. The causes were BCC in all cases. The tumor locations were the face in all patients. All of the flaps survived apart from only one case in which there was partial flap loss. Postoperative recovery was usually rapid. Conclusions: The V-Y advancement flap is preferably used for small and medium size facial defects. Its advantages are less scarring and superior aesthetic results as compared with other local flap methods.
Keywords: Surgical flaps, BCC, Face reconstructive surgical procedures, V-Y flap
Cite this paper: Waleed Elnahas, M. T. Hafez, Reda A. Younis, Loai Elbassiony, Mohamed A. Hegazy, V-Y Advancement Flap for Reconstruction of Defects after Excision of Basal Cell Carcinoma of the Face, International Journal of Surgical Research, Vol. 3 No. 1, 2014, pp. 15-18. doi: 10.5923/j.surgery.20140301.03.
1. Introduction
- Basal cell carcinoma (BCC) is the most common skin cancer with significant local tissue invasion and morbidity.[1] Since long time the conventional treatment option is surgical excision with free safety margins. The narrower the free surgical margin, the higher the recurrence rate.[2] Soft tissue defects due to tumor excision are important medical and cosmetic issues. Because of a rise not only in tumor incidence, but also in patients’ expectations regarding their quality of life after surgery, the need for functionally and esthetically high-quality reconstruction is now greater than ever.[3] Compared with skin grafts and free flaps, primary closure and local flap are advantageous because less scar tissue is formed following reconstruction, the use of similar adjacent tissue provides cosmetic benefits, and they do not have the risk of donor site morbidity.[4] V-Y advancement flap is a flap in which the incision is shaped like a V and after closure like a Y, partially or totally detached, to lengthen a localized area of tissue to gain access to structures underneath or to be used in repairing defects in an adjacent part of the body. In this study we evaluate the use of v-y advancement flap in covering defects after basal cell carcinomas excision of the face.[5]
2. Patients and Methods
- Over the period between September 2011 and May 2013, thirty-seven patients of basal cell carcinoma of the face were included in this study at surgical oncology unit, Mansoura oncology center and plastic department, Mansoura University. There were 30 males and 7 females. Age of the patients was ranged from 51 to 69. Patients with extensive co morbidity were excluded from this study. Sites of basal cell carcinoma in the face were summarized in table 1. Preoperative design and detection of the perforators within the flap by hand Doppler was performed. (Fig. 1).
|
 | Figure 1. preoperative design and detection of preoperative perforators by hand Doppler |
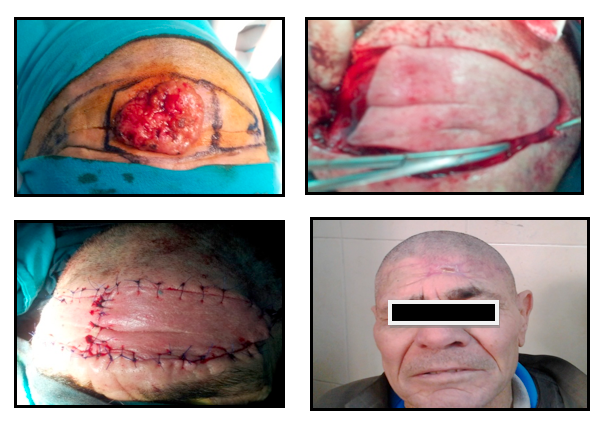 | Figure 2. preoperative marking, early post operative results and results after 6 month a case of basal cell carcinoma of the forehead |
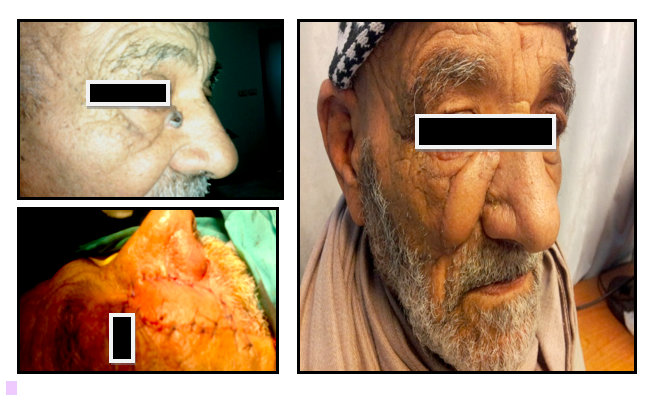 | Figure 3. preoperative, early postoperative and 6 month after surgery of a case of basal cell carcinoma of the side of the nose |
3. Results
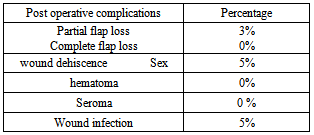
- The tumor diameters varied from 12 to 44 mm (mean, 28 mm). All patients were treated under general anesthesia. We did not apply any algorithm to select a unilateral or bilateral V-Y advancement flap, and thus, the choice was made after considering the defect location, skin condition, and expected scarring. Complete flap survival was achieved in 36 cases (97%). There was a case of partial flap necrosis of the forehead and healed by secondary intention. There was wound dehiscence encountered in two cases due to wound infection, which were managed by antibiotics, frequent dressings then secondary sutures. There was no hematoma, or seroma occurred. (Table 2) Bilateral flaps were used in 5 cases of the forehead while in the other 32 cases unilateral flap was used. All of the patients had excellent skin coverage. No recurrence at the primary tumor site was detected during the follow-up period, which ranged from 6 months to 26 months. Aesthetic results were deemed excellent in 20 patients (55%), while 13 patients shows good results (35%) and 4 patients were fair result (10%). The color and texture matches were aesthetically good and the contour was distinct in all patients.
|
4. Discussion
- In this study, all cases were basal cell carcinoma of the face planned for excision with three dimensional safety margins and reconstruction.Appropriate margins for malignant tumors depend on the cancer type, tumor size, tumor irregularity, and time elapsed from onset. In cases of basal cell carcinoma, an appropriate excision margin would be 2 to 5 mm from the tumor, whereas in cases with a small-sized lesion of <2 cm in diameter, it would be approximately 4 mm. On the other hand, in cases with a lesion of >2 cm in diameter or with a substantial delay after onset, the margin would be 1 cm, and in recurrent cases, it would be >1 cm. (1, 2). In our study, we used mean safety margins of 3 mm, and all margins were proved to be free by intraoperative frozen section.A number of different techniques have been described for reconstruction of the face defects after excision of malignant tumors. To date, there are no clear criteria for the selection of one or the other technique.[6]Four methods are used to reconstruct soft tissue defects after the surgical excision of skin tumors: primary closure, skin graft, local and free flaps. The most important factors to be considered for reconstruction are defect location and shape.[7]Primary closure is the most commonly used method to treat soft tissue defects. In the reconstruction of primary closure for circular defects, a dog-ear had been considered the standard approach. To avoid dog-ears, an elliptical excision would be needed that would include adjacent normal tissue. As a result, it would create a longer scar than the defect. Therefore, primary closure may not be appropriate for use in the facial region from a cosmetic perspective.[8]Skin grafting is usually performed when defects are large and unsuitable for primary closure or a local flap. However, skin grafts are less desirable due to the color differences between the donor and recipient sites and scarring. Therefore, in patients with small-to-medium defects, a local flap rather than a skin graft is preferred.[9]Various local flap methods can be used, the application of which are dependent on skin tissue status and skin defect location.[4] In practice, the optimal method for a local flap depends initially on the surgeon's preference. Rotational flaps are used frequently, but although the procedure is straightforward, it has the disadvantages of leaving large elliptical scars, requiring the resection of a large amount of normal skin tissue, and causing anatomical deformities of the adjacent structures. In particular, in younger patients, rotational flaps exert excessive tension on the face, where there is no redundant skin, and leave obvious scars. Advancement flaps are used when the patient is in overall good health and the defect is free of tumor and obvious infection. Flaps should match thickness, color, and texture of excised skin. Resultant scars should fall in relaxed skin-tension lines.We used V-Y advancement flaps with a unilateral or bilateral pedicle to reconstruct soft tissue defects after the surgical excision of skin tumors of the face. This method involves the transfer of a V-shaped flap to the defect site and converting it to a Y-shaped flap using a random pattern flap involving dermal plexus and subdermal plexus, which are connected by a subcutaneous perforating artery arising from the muscle.[10] We identified the subcutaneous perforator by hand Doppler preoperative in all cases to ensure adequate blood supply. Many authors including Dufourmentel and Talaat have previously described the subcutaneous pedicled V-Y flap,[11] who have coined the term "kite flap", which also refers to cases in which the skin island overlies the orbicularis oculi muscle for defects of the medial canthus and lower lid. The flap is optimally designed so that the common limb of the Y falls into the boundary with neighboring aesthetic regions or within a natural crease, fold, or wrinkle.The advantages of the V-Y advancement flap are the preservation of sensation and length, and good soft tissue coverage. Tension, however, is the primary problem encountered with this flap, especially with larger defects. The point of maximum tension occurs where the gap of the defect is greatest, which is in the mid portion of the defect. The need for a tension-free closure is highlighted in a variety of sources. If a tension-free closure is not achieved, the flap is at risk for necrosis.[12]The V-Y advancement flap is particularly useful when a structure or region requires lengthening or release from a contracted state. When a skin tumor is present on the margin of an aesthetic unit, excellent cosmetic outcomes can be obtained using a V-Y advancement flap. In elderly patients, by identifying redundant skin areas, we have transferred bilateral flaps after adjustment for size. Thus, by using V-Y advancement flaps we have achieved excellent cosmetic outcomes in the facial region.[3]Scar widening is related to ongoing tension. According to geometric analysis, compared with a pivot flap that includes a rotational flap and transpositional flap, the V-Y advancement flap provides much less tension, which reduces the risk of hypertrophic changes and scar widening in the long term.[13]Furthermore, because a V-Y flap also creates a smaller dead space, it presents lower risks of postoperative complications such as seroma and hematoma.Another disadvantage is scar revision for stigmata of a V-Y advancement flap. Although abnormal scar formation, such as a hypertrophic scar or widening scar, occurs less often with V-Y flaps than with the other flap methods, the stigmata is not linear; it is of a rhomboidal shape. Therefore, it is very difficult to correct the scar by making it invisible.[3]Although there are various methods for reconstructing skin defects created by skin tumor resection, we believe that the V-Y advancement flap produces good treatment outcomes in cases with small-to-medium defects.
5. Conclusions
- The V-Y advancement flap is preferably used for small and medium size facial defects. Its advantages are less scarring and superior aesthetic results as compared with other local flap methods.