-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Surgical Research
2014; 3(1): 1-6
doi:10.5923/j.surgery.20140301.01
Cytokines and Postoperative Hyperglycaemia: From Claude Bernard to Enhanced Recovery after Surgery
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLElroy Patrick Weledji
Senior lecturer in Anatomy and Clinical Surgery, Faculty of Health Sciences, University of Buea, Cameroon
Correspondence to: Elroy Patrick Weledji, Senior lecturer in Anatomy and Clinical Surgery, Faculty of Health Sciences, University of Buea, Cameroon.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Background:Immune response and metabolic regulation are highly integrated and the proper function of each is dependent on the other. Cytokines are helpful towards the host response but potentially hazardous if uncontrollable or in excess. This is seenmetabolically in the ‘diabetes of injury’ and the immunosuppression that follows major surgery or trauma. Objective: To evaluate the role of cytokines in the metabolic response to surgery and the association with the new insight of enhancing recovery after surgery. Methods:Electronic searches of the medline (PubMed) data base, Cochrane library and science citation index were performed to identify original published studies on cytokines and metabolism, and enhanced recovery after surgery. Relevant articles were searched from relevant chapters in specialized texts and all included. Results: Surgery is a stressor that affects homeostasis. Excess cytokines cause insulin resistance and thus type-2 diabetes through a compleximmuno-physiological response to surgery. Conclusion: A precise understanding of the cytokine response to surgical trauma may bring in interventions that would optimise the perioperative care of the patient, decrease morbidity and enhance recovery.
Keywords: Cytokines, Metabolism, Surgical stress, Insulin resistance, Enhanced recovery
Cite this paper: Elroy Patrick Weledji, Cytokines and Postoperative Hyperglycaemia: From Claude Bernard to Enhanced Recovery after Surgery, International Journal of Surgical Research, Vol. 3 No. 1, 2014, pp. 1-6. doi: 10.5923/j.surgery.20140301.01.
Article Outline
1. Introduction
- Many metabolic and immune response pathways have been evolutionary conserved throughout species.[1] Cytokines are signalling peptides produced by inflammatory cells during injury. They initiate the acute phase response, recruit reticulo-endothelial cells (lymphocytes, monocytes and macrophages), promote wound repair and induce the production of other cytokines (amplification of response).[2] The complex network of cytokines balances pro-inflammatory and anti-inflammatory effects and an imbalance or the uncontrolled production of cytokines can result in inflammatory disease.[1] The new insight of enhancing recovery after major elective surgery is based on the principle of reducing metabolic stress in surgery by limiting the initiating factors-(1) cytokines produced from tissue injury and (2) stress hormones from the hypothalamic- pituitary-adrenal axis (HPA).[3]
2. Surgical Stress
- Claude Bernard in 1877 gave the first report on hyperglycaemia in stress from haemorrhage. Thus, disclosing the glycogenic function of the liver and the drastic change in biological thought of plants being the sole source of glycogen (Fig. 1).[4] In acute haemorrhage, insulin resistance is needed to mobilize glucose to achieve fluid movements and plasma refill.[5] In the 20th century, this hyperglycaemia in stress was termed ‘diabetes of injury’ which is a type 2 (non-insulin dependent) diabetes. It is known that insulin resistance is a marker of surgical stress and cytokine hypersecretion stimulate insulin resistance.[6] The principal mechanism by which the inflammatory signals interfere with insulin action involves post translational modification of insulin receptor substrate molecules particularly via serine phosphorylation. The enzyme c- Jun N-terminal kinase (JNK) is a central mediator.[7] The endoplasmic reticulum (ER) plays a central role in integrating multiple metabolic signals critical in cellular homeostasis. Therefore conditions that challenge ER function such as hyperglycaemia in surgical stress would induce ER stress and increase serine phosphorylation of insulin receptor substrate-1 in an inositol requiring and JNK –dependent manner and thus block insulin action.[8] In mice, compromising ER function through targeted mutations in the Xbp-1 gene results in insulin resistance and type 2 diabetes that are also dependent on JNK activation.[8] Modulation of ER function by chemical chapeyrones,phenyl butyric acid and taurine-conjugated ursodeoxycholic acid led to markedly enhanced insulin receptor signalling in peripheral tissues and restored proper insulin function.[1,9]
 | Figure 1. Claude Bernard (1813-1878) |
2.1. Afferent Nerve Impulse
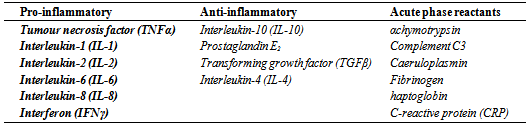
- Afferent nerve impulses to the brain are triggered not only by pain but by cytokines produced from inflammatory cells in the wound. Pro-inflammatory (interleukins IL-1,6, 8, tumour necrosis factor (TNF) and anti-inflammatory (interleukin-IL-10, IL-4) cytokines are released into the systemic circulation to cause a myriad of systemic effects- the acute phase response (Table 1). These include fever, leucocytosis, hypothalamic-pituitary-adrenal (HPA) axis stimulation of the catabolic hormones, acute phase protein synthesis in the liver and immune activation.[10]
|
2.2. Immunological Changes
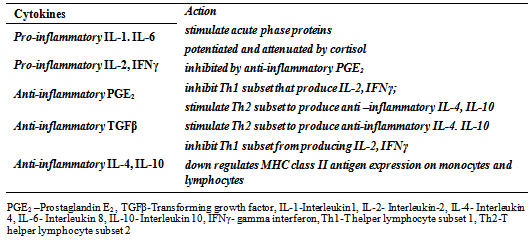
- Injury, haemorrhage and endotoxin result in the release of a number of key cytokines (prostaglandin (PG) E2 and transforming growth factor TGFβ), that haveprofound effect on monocyte function.[1,2] There are selective immunosuppressive effects during surgical stress. Cytokine secretion by T-lymphocytes is suppressed after major surgery giving rise to an increased susceptibility to infection with intracellular pathogens such as listeria and mycobacteria.[12] The cytokine prostaglandin (PG) E2 being principally immunosuppressive prevents the production and release of cytokines-interleukin (IL-2) and interferon (IFNγ) by the Th1 subclass of T helper lymphocytes. The production is impaired following surgical trauma or traumatic injury. [2,13] PGE2 is also capable of stimulating Th2 subclass to produce the anti-inflammatory cytokines IL-4 and IL-10 which inturn inhibit Th1 cytokine production during surgical injury (Fig.1). IL-10 downregulates the majorhistocompatibility complex (MHC) classII molecules on the surface of monocytes and T cells.The cytokine, transforming growth factor (TGFβ) also downregulates cellular processes by stimulating the Th2 subsets.[2] The transcription of gene for IL-10 is up regulated in peripheral blood mononuclear cells and the down regulation of MHS class II expression follows major resectional surgery. (Table 2)[14] The expression of MHC class II antigens is a marker of monocyte activation and the capacity to engulf opsonised organisms.[15] Downregulation correlates with clinical outcome and the development of infection following surgery due to defect in neutrophil chemotaxis, phagocytosis, and lysosomal enzyme contents.[16] Thus it seemed reasonable to attempt to adjust this MHC class II antigen level clinically by administering interferon (IFNγ). This may benefit those whose post-traumatic MHC class II recovery was delayed or did not recover at all. The first reported trial of treatment of trauma patients with recombinant human interferon provided supportive but not statistically significant data.[17] The multiplicity of factors that influence the outcome of major surgery and the variability of the individual’s response especially with regard to their initial level of receptor expression will obviate the effect.[2,18]
|
- The anti-inflammatory cytokine (IL-10) secretion is increased by monocytes after major surgery.[1,2] Although this may be a homeostatic response it would be interesting to know how much of these may be the effect of the hyperglycaemia (diabetes) of injury. This is corroborated by the observation that cytokine secretion by monocytes decrease following preoperative carbohydrate loading but increase in fasting.[19] Despite the major impact of prophylactic antibiotics, the overall incidence of sepsis after elective surgery remains static (5-10%).[2,10] Though technical factors may play a part this residual sepsis may be a reflection of perturbation of the immune system due to surgical stress.[1,2] Because many operations are accompanied by haemorrhage, the postoperative immune depression may also be caused in part by blood loss and cellular hypoxia rather than surgery.[5] Perioperative blood transfusion may also contribute to immunosuppression but the underlying mechanism is largely unknown.[20]
2.3. Acute Phase Response
- The positive acute phase reactants (cytokines) rise during the acute phase response to surgical trauma. These include α chymotrypsin, complement (C3), caeruloplasmin, fibrinogen, haptoglobin, and C-reactive protein (CRP). The negative reactants are the normal response to trauma with decreased protein synthesis, and the levels decline during the same period. These include albumin and transferrin. The reason for the acute phase reactants is for host defence. C3 and CRP are required by phagocytic cells for opsonisation, fibrinogen is essential for blood coagulation and proteases limit tissue destruction. The serum levels rise during the first 24-48 hrs after surgery is proportional to the severity of injury. It falls back to normal after 48-96 hrs but may remain elevated in presence of sepsis or other complications.[10] The systemic inflammatory response syndrome (SIRS) is a massive systemic reaction arising from a variety of insults. The evolution of cytokine cascade leads to sustained activation of the reticuloendothelial system and elaboration of cell damaging secondary mediators such as nitric oxide, arachidonic metabolites (prostaglandins and leukotrienes), oxygen free radicals, platelet activating factor causing platelet aggregation, vasodilatation and increased capillary permeability. The clinical response of SIRS includes 2 or more of the following (temp> 38℃ or <36℃; heart rate (HR)> 90 beats/min; respiratory rate (RR) >20 breaths/min; white cell count (WCC) >12 or <4 x 109 C.[1,10]
2.4. Metabolic Response
- The afferent stimuli from tissue injury produces neurohumoral responses in the form of cytokines and the stress hormones (adrenaline, glucagon, cortisol, growth hormone) that rapidly stimulate a cardiovascular and metabolic response. The metabolic response has a short ebb phase and a long flow phase. The short ebb phase lasting 12 to 24 hours is the period of traumatic shock with general depression of enzymatic activity and oxygen consumption. The blood pressure, cardiac output and body temperature are reduced. These are often associated with haemorrhage and result in hypoperfusion and lactic acidosis. As the blood volume is restored, more accelerated responses occur (the flow phase)in which the patient exhibits an increase in total energy requirement.[10,21] The flow phase has an initial catabolic phase which is of most concern in the management of the operated or injured patient and lasts for 3-8 days. Muscle and fat stores are plundered in order to maintain adequate energy for the whole organism. This is followed by an anabolic (recovery) phase which is now influenced by the anabolic hormone, insulin. The anabolic phase lasts for some weeks as protein and fat stores are restored and weight regained.[21] In the catabolic phase, adrenaline produced from the adrenal medulla by sympathetic nervous system stimulation mobilises protein and fat causing an increased urinary nitrogen excretion with consequent . negative nitrogen balance and weight loss. There is increase glucose production from glycogenolysis and gluconeogenesis from proteins stimulated by glucagon. Insulin secretion increases but its sensitivity decreases because of the inhibitory action of adrenaline and glucagon. All these gives rise to hyperglycaemia (‘diabetes’ of injury).[21,22] Insulin resistance rises with the magnitude of the injury. For example it is lower in laparoscopic than open cholecystectomy and greaterin major colorectal surgery. [11,23] In major surgical procedures such as major colorectal operations, up to 90% of the pre-operative insulin sensitivity can be lost after the operation.[6] This change in metabolism lasts for well over a week which is the average length of the catabolic phase of the metabolic response. [10,21]The catabolic period of the flow phase is of most concern in themanagement of the operated or injured patient. Factors that modify the metabolic response affect the magnitude and duration of the response. These include the severity of the injury as the greater the injury the greater the response; the nature of the injury as for example burns which produce a greater response because of greater heat and fluid loss from the burn area; infection and other complications such as deep vein thrombosis, pulmonary embolism which prolong the catabolic phase, and prolonged post trauma starvation that adversely affects convalescence. Anaesthesia and drugs modify the response by affecting the vascular system and hormone (catecholamine and anti-diuretic hormone) production (Table 3).[10,21]
|
|
3. Enhanced Recovery after Surgery–reducing Surgical Stress
- The independent factors predicting length of hospital stay are (a) type of surgery (70%), (b) perioperative blood loss and (c) postoperative insulin resistance.[3-6,29] The new insight of enhanced recovery after major elective surgery is manifested by avoiding the stress hormones using thoracic epidural anaesthesia and minimally invasive (laparascopic) surgery; avoiding stress-induced hyperglycaemia by pre-operative anabolic setting of the patient and avoiding fasting; treating hyperglycaemia with insulin; postoperative pain control with epidural analgesia and early postoperative feeding and mobilisation (Fig.2).[30-32] Epidural analgesia reduces postoperative insulin resistance by 45% due to blockage of afferent pain impulses and increases gut motility as compared to intravenous opioids which decrease gut motility.[33] By reducing surgical stress and hence minimising the catabolic response and insulin resistance, the patient including the high risk with comorbidity, the hospital and the community benefits.[34,35] The enhanced recovery programme being based on surgical physiology is the next revolution in surgical care following laparoscopy.[36]
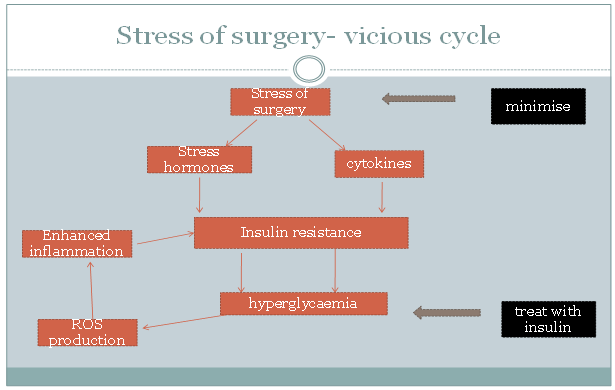 | Figure 2. The vicious cycle of the stress of surgery |
4. Conclusions
- Surgery is a stressor that affects homeostasis. It is a long way from Claude Bernard to the new insight of enhanced recovery after surgery. Further insight into the endoplasmic reticulum central mechanism underlying inflammatory and stress responses would offer potential new therapeutic opportunities against insulin resistance and type 2diabetes. A precise understanding of the cytokine response to surgical trauma may be exploited therapeutically to optimise the perioperative care of the patient, decrease morbidity and enhance recovery.