-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Stroke Research
2015; 3(1): 1-5
doi:10.5923/j.stroke.20150301.01
Risk Factors for Stroke: A Hospital Based Descriptive Study in North India
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRayaz Jan, Rajiv Kumar Gupta, Parveen Singh, Tajali Shora, Shahid Hussain
PG Department of Community Medicine, Govt. Medical College, Jammu, India
Correspondence to: Rayaz Jan, PG Department of Community Medicine, Govt. Medical College, Jammu, India.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Introduction: Stroke is a major public health problem, both in developed and developing world. It causes a lot of morbidity and mortality especially with advancing age and lot of economic burden on the families of those afflicted with stroke. Aim: To find out the association of risk factors like Obesity, Cholesterol, Smoking and Alcohol to the Stroke. Methodology: The present descriptive study was conducted in the calendar year of 2011. The study subjects comprised of the patients who were admitted to Govt. Medical College and Hospital Jammu with sign and symptoms suggestive of stroke. The relevant information of each study subject was recorded on pre-designed and pre-tested proforma. Results: A total of 209 respondents (114 males and 95 females) were interviewed during the course of study. 57.90% (121/209) study subjects were found to be obese. 77.96% (92/118) had cholesterol level on the higher side. Out of 114 males in the current study 60.52% (69/114) were smoker and 62.28% (71/114) were alcoholic. Both smoking and alcohol were found to be statistically significant risk factors for stroke. Conclusions: The results clearly demonstrate that lifestyle factors have a huge impact on the causation of non-communicable diseases in general and stroke in particular and hence the need for primordial prevention at the earliest.
Keywords: Stroke, Obesity, Smoking, Alcohol, Risk factors
Cite this paper: Rayaz Jan, Rajiv Kumar Gupta, Parveen Singh, Tajali Shora, Shahid Hussain, Risk Factors for Stroke: A Hospital Based Descriptive Study in North India, International Journal of Stroke Research, Vol. 3 No. 1, 2015, pp. 1-5. doi: 10.5923/j.stroke.20150301.01.
Article Outline
1. Introduction
- Stroke is a significant public health problem both in developed and developing world. Stroke caused 11% of global deaths in 2011 and was the second most frequent cause of death. [1] The trends have shown that number of stroke cases decreased by 10% in developed world but increased by 10% in the developing world between 1990 and 2010, [2] which has serious repercussions for the least developed and the developing nations.The estimated cost of stroke related healthcare is about 68.9 billion dollars both in terms of health care as well as lost productivity. [3] South Asia comprising of eight countries including India constitutes 22% of the world’s population and accounts for about 40% of global stroke deaths. In this region of the world, stroke and coronary heart disease occur a decade earlier than the rest of the world. [4] It is therefore imperative to study epidemiology including risk factors, region-specific issues and outcome of stroke in different regions of India. The specifics so understood would help in reducing burden of stroke and improve outcome.Considering the prevalence, incidence, morbidity and mortality and rising trend in younger population and in developing countries it seems mandatory to search for risk factors that predispose to stroke. In developed countries various endeavors are on for early diagnosis and appropriate management to reduce stroke related morbidity and mortality. But scenario in our country is different. Burden of disease in India (2005) [5] had estimated that there had been an increase in the number of stroke cases in India during the last one and a half decade by 17.05%, thus showing a worrying upward trends of disease.A variety of risk factors have been implicated in the causation of stroke. In the modifiable risk factors for stroke, high blood pressure, and atrial fibrillation are the most important, the rest being high blood cholesterol levels, diabetes mellitus, cigarette smoking, Lack of physical activity, obesity, unhealthy diet, [6] heavy alcohol consumption. [7]In the non-modifiable risk factors, advanced age is the single most significant risk factor as 95% of stroke cases occur in people aged 45 years and above and 2/3rd of stroke occur in those over the age of 65 years. Besides, men are 25% more likely to suffer strokes than women. [8, 9]In this part of country viz Northern India, very limited published literature is available especially in context of risk factors in stroke causation. It was in this context that this risk factor study was conducted in Jammu region of Jammu and Kashmir State, India (Fig 1). The present hospital based study was conducted in the Government medical college and hospital Jammu, with the aim to find out the association of risk factors like obesity, cholesterol, smoking and alcohol to the stroke.
 | Figure 1. Map showing study area (Jammu Province of Jammu & Kashmir State) |
2. Materials and Methods
- The present descriptive study was conducted in the calendar year of 2011. The study subjects comprised of the patients who were admitted to Govt. Medical College and Hospital (GMCH) Jammu with sign and symptoms suggestive of stroke irrespective of their age, sex, religion and place of residence.The state of Jammu and Kashmir consists of three regions: Jammu, Kashmir valley and Ladakh. Jammu is the winter capital of the state and Govt. Medical College and Hospital is the tertiary care hospital located in the heart of Jammu city. Total population of Jammu Province is approximately 53,50,811 (Census 2011) [10] distributed among 10 districts. It was expected that majority of the cases of acute stroke are referred or come on their own to avail the treatment facilities at this hospital.After initial emergency management, the suspected stroke patients are shifted to indoor wards for further work up. The researcher kept a tab on daily admission of these cases. The relevant information of each study subject was recorded on a pre-designed and pre-tested Proforma. Only those patients who were confirmed on Computed Tomography (CT) scan as stroke cases were included in the present study. Permission from the ethical committee of the Govt. medical college, Jammu was sought before conducting the study. The patient or his/her relatives were explained the purpose of the study before he or she was administered the questionnaires.After collecting the base line information on the designated Proforma, other relevant information about risk factors was elicited in detail from the study subjects when they were fit enough to respond to the questionnaire. In the event of study subjects being unfit to respond to our questionnaire, then the information was collected from a family member of the study subject who happened to be an attendant for him/her.All the relevant information regarding age, sex, place of residence, family composition & socio-economic status (“Modified Uday Pareek Scale” for rural patients & “Kappuswamy’s Scale” for urban patients) was meticulously recorded.Further, history was taken regarding lifestyle factors such as smoking and alcohol intake. Regarding smoking habits, they were enquired about the type of smoking i.e. cigarette, bidi/chillum, their frequency and duration. As for alcohol, each patients was also asked whether he/she takes alcohol and if yes, then its frequency and duration. Obesity was measured as per WHO classification of Body Mass Index [2003]. [10] Similarly the person was diagnosed as having increased level of cholesterol in accordance with National cholesterol education programe, adult treatment panel-III (2001) i.e. ≥200mg/dl. [12]Both general and physical examination of the study subjects was performed and the information so collected was recorded in the designed Proforma.The information & data thus collected was complied & analyzed using standard appropriate statistical methods.
3. Results
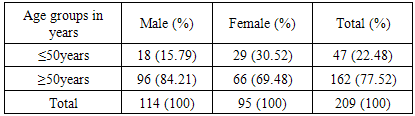
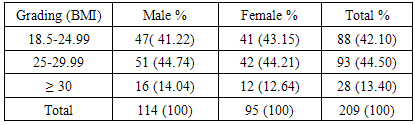
- A total of 209 respondents (114 males and 95 females) were interviewed during the course of study. It was observed that age group 51-70 years comprised more than half of the study subject’s (Fig 2). In the current study as per WHO criteria for pre-obese and obesity, 57.90% (121/209) study subjects were found to be obese. Of them 76.85% (93/121) study subjects were in pre-obese category and 23.14% (28/121) were in obese category (Table 2).
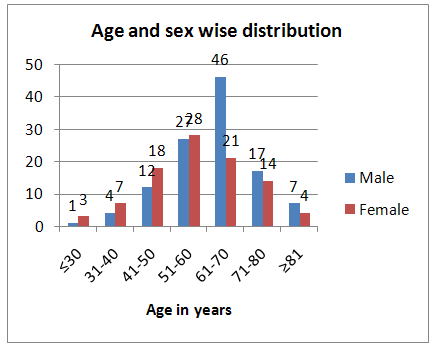 | Figure 2. Distribution of the study population on the basis of age and sex |
|
|
|
|
|
4. Discussion
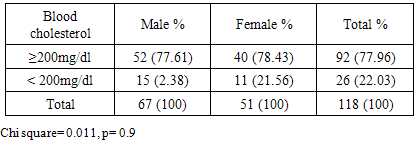
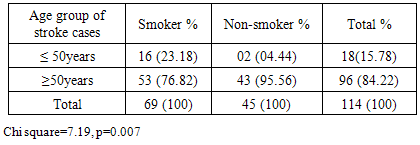
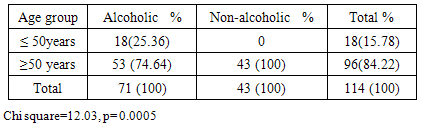
- In the current hospital based study of stroke, the results have revealed that as the Body Mass Index (BMI) increases, risk of getting stroke also increases. Majority of the stroke cases 57.89% (121/209) had BMI >25 kg/m2. In a meta-analysis carried out by Hiroshi Y et al [13] it was found that BMI >25 kg/m2 had a strong association with the occurrence of stroke cases. Strazzullo P et al [14] in his meta-analysis of 25 studies reported relative risk for ischemic stroke was 1.22 for overweight and relative risk 1.64 for obesity, where as relative risk for hemorrhagic stroke as 1.01 for overweight and 1.24 for obesity. Our results are not in agreement with the INTERSTROKE study [15] where assessment of anthropometrical factors showed that body mass index was not associated with stroke, but authors reported waist-hip-ratio was associated with increased risk of both ischemic and intracerebral hemorrhagic stroke.In the present study, 77.96% (92/118) of study subjects had higher level of cholesterol in their lipid profile. Our results are in agreement with those reported by Nayak et al (1997) [16] and J Woo et al (1990) [7]. However in some studies like Carlo La et al (1986) [17] blood cholesterol level did not show any relationship with stroke occurrence while, in another study done by Kagan A et al (1984) [18] blood cholesterol level was inversely related to stroke. Of the 114 male cases in the current study, 69 were found to be smokers. So 60.52% (69/114) of the study subjects who were smokers were affected with stroke, thus implicating smoking to be a major risk factor for the disease. Similar results were reported by other authors like Bhattachary et al (2005) [19] Nayak et al (1997) [16] Rajinder K Dhamija et al (2000) [20], R Monforte et al (1989). [21] Sanne A.E. Peters, Rachel R. Huxley and Mark Woodward (2013) [22] also reported that smoking was an independent risk factor for stroke in both sexes. Our results are also in agreement with a case control study conducted by Ma X et al (2014). [23] Where authors reported that cigarette smoking was associated with ischemic stroke.The results of the present study show that out of 114 male cases, 71/114 (62.28%) of the study subjects were alcoholic thus showing that alcohol intake has some role to play in the outcome of stroke. Alcohol consumption as a risk factor for stroke has also been reported by R Manforte et al (1989) [21] Hiroyasu Iso et al (1995). [24] The INTERSTROKE study [15] also reported that smoking and alcohol intake were significant risk factors for intracerebral hemorrhagic stroke. Rantakomi SH et al 2014 [25], in their study among eastern Finish men also reported strong association between the frequency of alcohol consumption and stroke mortality. Mostofsky E et al (2010) [26] also reported that 64% of the stroke cases had consumed alcohol in previous one year.
5. Conclusions
- Out of 209 study subjects, 114 were male and 95 were females. 121/209 (57.90%) of the study subjects were found to be obese as per WHO guidelines, but it was not statistically significant. 92/118 (77.96%) of the stroke cases had cholesterol levels on the higher side which was statistically insignificant. Of the 114 males in the study, 69 were smokers and smoking as a risk factor for stroke was found to be statistically significant. Similarly alcohol as a risk factor in stroke cases was also found to be highly significant statistically.
6. Limitations
- An important limitation of the current study was the inclusion bias which is attributable to a single medical college and hospital for the study purpose. Another limitation is the study design it being a hospital based study but though a descriptive one. More studies need to be carried out to determine the role of other risk factors in stroke causation like hypertension, diabetes mellitus, physical activity etc. in this region of India. Another limiting factor could be non-responding of smoking among females who may tend to hide this habit due to socio-cultural reasons.
7. Recommendations
- The risk factors of stroke need to be repeatedly promoted both in electronic and print media for public awareness. The essential component of such awareness programmes should include healthy eating habits, promoting regular exercise, avoiding junk foods, avoidance of alcohol and smoking and effective management of predisposing conditions like diabetes mellitus, hypertension and obesity. Interventions like promoting low salt intake, stop smoking campaign, promotion of physical activity and cost-effective medication are likely to avert 10 million deaths in next decade. It is imperative here to add the key role of primordial prevention in checking ever increasing levels of obesity in the population at large.