Zahra Khanum1, Yasmin Zahra Jafri1, Azhar Marri1, Shabana Yasmeen2, Summiya Malik3, Madiha Raza4, Syed Fareed Ullah1
1Department of Statistics, University of Balochistan, Quetta, Pakistan
2Agricultural Research Institute, Mastung, Pakistan
3Agricultural Research Institute, Quetta, Pakistan
4Zia-ud-din Medical University, Pakistan
Correspondence to: Zahra Khanum, Department of Statistics, University of Balochistan, Quetta, Pakistan.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
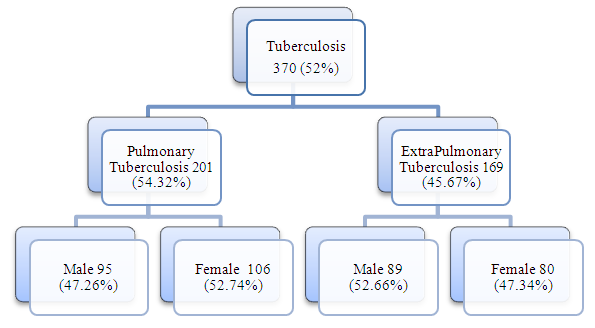
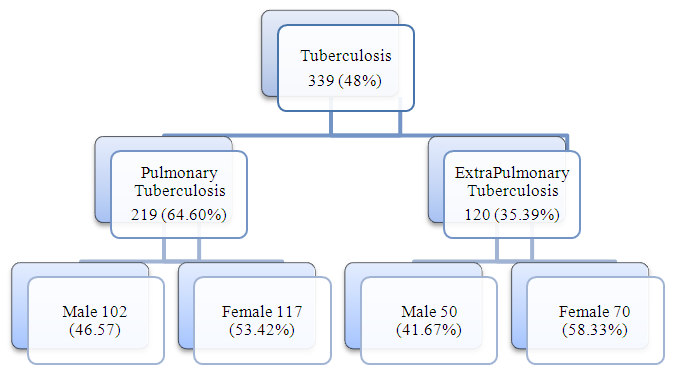
Background: Tuberculosis (TB) remains one of the leading communicable disease in the world. TB is a potentially serious infection disease that mainly attack lungs. 27000 new cases have been emerging from Balochistan every year millions of people are affected and loose their lives. This study was undertaken to determine the prevalence and risk factors of tuberculosis patients enrolled in Provincial TB Control Program. Data are collected from health units of Quetta, Jafarabad, Gawadar, Noshki, Lasbela, and Loralai (Balochistan, Pakistan). Objective: • The aim of current study was to determine the prevalence and associated risk factors of tuberculosis. • To see the effect of weather on tuberculosis in winter and summer. • Comparative study of Pulmonary and Extrapulmonary TB. • To create awareness in people of Balochistan against tuberculosis. Methods: A cross sectional study was designed over a period of six month (Jan to June) 2016 comprises two quarters, winter and summer in six districts of Balochistan, Pakistan. The data were collected from health clinics formed of Provincial TB Control Program Balochistan. A total of 2609 patients were screened systematically and diagnoses were based on clinical examination and bacteriological test. We also made comparison between pulmonary (PTB) and extrapulmonary (EPTB) tuberculosis in six major districts of Balochistan. Results: The prevalence of bacteriologically conformed of these 709 cases. Two quarters winter and summer comprises 370 and 339 patients respectively. In winter the prevalence of pulmonary tuberculosis (PTB) (54.32%), and extrapulmonary tuberculosis (EPTB) was (45.67%). The average age for pulmonary tuberculosis and extrapulmonary tuberculosis group were [15-24 (19.2%), and 25-34 (16.8%)]. In summer the prevalence of PTB (64.60%) and EPTB (35.39%). The age average for PTB and EPTB [15-24 (18.0%), & 25-34 (16.2%)]. In winter female or male was predominantly more infected by pulmonary TB (52.7%), while extrapulmonary tuberculosis was commonly detected in women (47.34%), (p = 0.423), and similarly for summer males and females was predominantly infected more by EPTB (58.3%), while PTB was commonly detected in women (53.42%), (p = 0.171).
Keywords:
Pulmonary Tuberculosis (PTB), ExtraPulmonary Tuberculosis (EPTB), World Health Organization (WHO), Directly Observed treatment Short Course (DOTS)
Cite this paper: Zahra Khanum, Yasmin Zahra Jafri, Azhar Marri, Shabana Yasmeen, Summiya Malik, Madiha Raza, Syed Fareed Ullah, Prevalence and Statistical Analysis of Various Risk Factors of Tuberculosis in Balochistan, Pakistan, International Journal of Statistics and Applications, Vol. 9 No. 6, 2019, pp. 191-200. doi: 10.5923/j.statistics.20190906.04.
1. Introduction
Literature survey is a necessary principle of every research which supports to get rational idea of the topic. Different secondary sources, .i-e., books, newspaper, reports, articles, and online basic material will be referred to gain insight of the topic. In 21st century, Tuberculosis (TB) is a main public health issue. The WHO report says that TB is the 2nd most important cause of deaths [1]. Balochistan is multicultural province of Pakistan, being the rich in resources. But, still is facing the life threatening disease such as tuberculosis, HIV, and Hepatitis, etc. With 44% of the total country area, Balochistan is the largest province of Pakistan. Most of the population is living in the rural areas in having the traditional tribal lifestyle and remaining is live in rural areas with sparse location. Nearest 2000 new cases of tuberculosis were recorded in 2012, although the directly observed treatment short course (DOTS) implemented effectively. A study was designed to observe the homological changes and related risk factor of smeared positive pulmonary tuberculosis patients in the targeted area. With a geometric progression (TB) is increasing 27000 new cases have been merging annually from Balochistan. The figures of TB patients have been observed increasing from Iran and Afghanistan. The people from these countries patients visit to Balochistan for treatment [2]. In 2013 alone, an estimated 8.0 million new cases of tuberculosis and 1.7 million deaths were recorded worldwide owing to tuberculosis while 370,000 of these deaths are as a result of HIV. Sub-Saharan Africa countries are responsible for the majority of these deaths and infections reported in the global south which is quarter of the world's TB cases [1]. Moghddam et al., reviewed that tuberculosis mainly affect any body part (TB extra-pulmonary) as well as brain, skin, bones, vertebral spine among others but can affect the lungs (pulmonary TB). The common sign of tuberculosis if the last cough for a period of more or 2 weeks which is generally accompanied with night sweats, fever, shortness of breath, tiredness, weight loss, chest pain, and loss of appetite in some instances hemoptysis. Extra-pulmonary (TB) presents with signs based on the body part affected in addition to general signs such as fever, weight loss, night sweats, and tiredness [3]. WHO Global Tuberculosis Reports says that along the human immunodeficiency virus HIV tuberculosis is the biggest health problem and being a prominent reason of death over the entire world. With the reference of 2016’s estimation 1.3million people acceded to the disease [4]. WHO Report says in 2016 worldwide with new cases 10.5 million and deaths 1.4 million (TB) tuberculosis is a leading infectious cause of death illness and death. [4]. Kyu et al studied that 95% deaths of tuberculosis occur in low income families [5]. The new cases of TB with 10.5 million new cases and approximately 40% without diagnosed in 2016 [6]. The major reason of deletion of TB disease is limited access to healthcare high treatment cost and social stigma. [7,8]. A continuous raise has been observed in case detection rate of childhood TB over the entire world with a parallel increase in the death toll of children with TB, According to WHO, mathematical calculation, it was calculated that 239,000 children died due to TB in 2015 [9]. In Pakistan, in the year of 2016, 518,000 calculated incidence of TB were confirmed. From which 50,000 were cases of children aged between ≤14 ages. Along India, Indonesia, Philippines, and China including Pakistan 57% of the worldwide total occurrence cases are accounted in 2016 [3]. Childhood TB is extensive and most significant reason of death and disease in increasing states remaining to poor socio-economic condition, hunger, and overloading, HIV co-infection [10]. The high prevalence of TB was studied by contacts in adults by Tilahun & Gebre-Selassie and the high commonness of tuberculosis in grownups associates [11]. In modern China, the most dangerous public health anxiety is population ageing. The percentage of aged women and men aged 65 and above used to be 10.8%, and persons aged 60 and above 16.7% of a populace of 1382 million persons in 2016 [12]. The scale of the wide ranging reflects the goal of the Sustainable Development Goals (SDGs) for 2030 and internationally its priority is to finish this disease TB globally [13]. Whereas TB Prevalence is no more an international sign per se, prevalence survey ensures precious practical steps to inform estimation of incidence and, in few cases impermanence [14]. Systematic screening of high-chance corporations to diagnose TB early has validated potent to support finish the worldwide TB epidemic [11,15].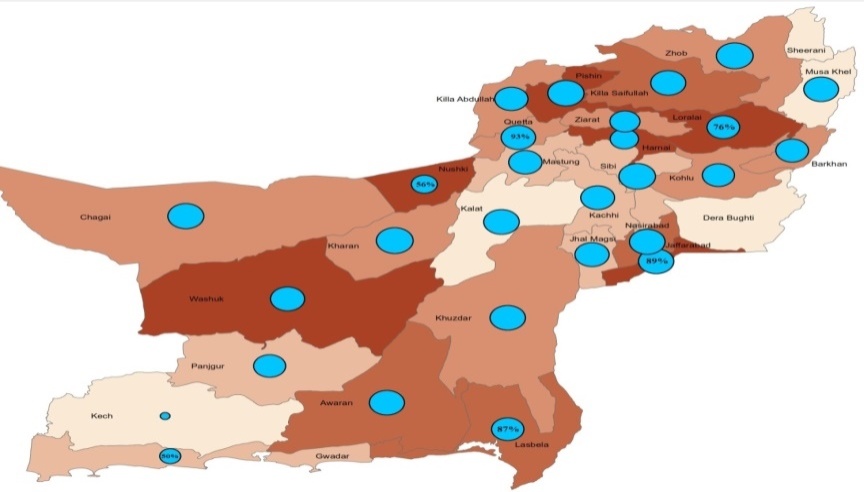 | Figure 1. Prevalence of Tuberculosis in Six Districts of Balochistan |
With 44% of the total country area, Balochistan is the largest province of Pakistan. Most of the population is living in the rural sparse locations in having the traditional tribal lifestyle and livelihood conditions are very poor. Nearest 2000 new cases of tuberculosis were recorded in 2012, although the directly observed treatment short course (DOTS) implemented effectively. A study was designed to observe the homological changes and related risk factor for smeared positive pulmonary tuberculosis patients in the targeted area were the trends (TB) of increasing [16].
2. Literature Review
Critical reviews of literature stays an obligatory part to get higher know-how of the challenge. One in all a kind secondary resource articles,. i-e., books, newspapers, opinions and on-line belongings can be referred to become understanding of the subject. Tuberculosis (TB) is an important public fitness bother that is preventable and treatable. Approximately 1-1/3 of world’s populace is infected with this disorder [17]. If left untreated, each energetic TB (sputum positive) case can infects ten to fifteen people in three hundred and sixty-five days. Worldwide Health Corporation (WHO) professed TB a universal emergency in 1993 and then it followed straight away create medicine, quick-path (DOTS) technique. After the implementation of dots, extra than twenty million patients were dealt with and greater than sixteen million cured of TB through 2004. Because of it, the mortality and prevalence of TB additionally decreased. Although development in this regards is gradual in Sub-Saharan Africa as well as the Japanese-Europe. Asia maintains to go through 0.33 of the weight of TB. Furthermore, new demanding conditions like tuberculosis and HIV co-infection, multi drug resistant TB and youth TB have emerged which might be hampering TB manipulation efforts [18]. To cope with those forms of problems, forestall TB approach was released by means of manner of (WHO) in 2006. One of the additives of this approach is to engage all care providers. Which means all fitness professionals offering care to the TB patients have to be worried? As a part of worldwide dots expansion plan, interest became known as to clinical schools. Medical university college students are future medical doctors and clinical faculties play a vital function in constructing competence and abilities of those college students in coping with the health troubles inside the network. Such as Pakistan is 5th amongst 22 global sites by maximum problem of TB, education of clinical university college scholars to solve this problem is not handiest vital, but urgent [19].In Pakistan one of the important public health problems is tuberculosis (TB). Pakistan positions 5th between tuberculosis immoderate-burden nations universal. It accounts for 61.0% of the TB burden inside the (WHO) Eastern Mediterranean area. About 430,000 new tuberculosis cases emerge every 365 days and partial of this sputum smear effectively. Pakistan is likewise predicted effectively to have the 4th main incidence of multidrug-resistant TB (MDR-TB) internationally [20]. Consistent with the statistics around 430,000 humans,of which 15,000 youngster’s settlement tuberculosis (TB) in Pakistan, fewer than 70,000 losses each one year may be credited to the infection inside the America yearly. TB is a main infectious disease due to lack of livelihood conditions. Pakistan ranks sixth globally. Tuberculosis burden worldwide places and underwrites an expected estimated 43.0% of the disease towards the Eastern Mediterranean region of the WHO. Pakistan is as well predicted to have the 4th maximum occurrence of multi-drug resistant TB (MDR-TB) internationally. While internationally due to TB every year 9.5 million fall ill and 1.6 million die. Over 95% in line with TB deaths rise in little and middle-profits countries [21]. This fatal disorder is increasing every day at few stages over the world. The shortage of fitness facilities, correct medicine and diagnoses underwriting to the excessive range of fatalities worldwide have become rampant. Balochistan stated 28.0% CDR, 80.0% TSR and 12.0% defaulting rate. (PTP Balochistan 2005). In order to raise the CDR to 70.0% and decrease the default rate fewer than 5%, there has been a need to broaden revolutionary interventions in order to critical targets set by WHO be carried out [22]. Given the importance of the TB trouble in Pakistan, in addition to the dimensions of the United States, a vertical TB manage programme is financially prohibitive and hard to maintain. Integration of the TB manipulation programme in percent has lately been opted for, as approach to its technical and managerial deficiencies. A network of laboratories requirements is to be created in addition to a system for making sure high-quality of sputum smear microscopy installed in every region or district.
3. Logistic Regression
Logistic Regression Model has a great collection review in biomedical and medical scan mostly to print models organization the factors that force to verify whether rather a risk occurs. The exceptional article of logistic regression model is that the outcome variable is dichotomous or binary. Generally, patient’s data would be used to find which ascriptions are powerful in calculating the result. They can previously be dignified for dressy patients over assigning in logistic regression model to solve the eventuality of supposing result called (Y). The binary logistic change of mind equation is:  | (1) |
in which P(Y) is the eventuality of subject to result forthcoming predicted and in this raw material was the emergency of foible in treatment course closing, β0 which is a Constant and X1 to X𝑛 shows the graph of logistic regression and explain it with equation (1), β1...βn are the models parameters rollick the style of constantsaside attributer.
4. Material and Method
4.1. Aim of the Study
Purpose of the recent research is the Prevalence and Risk Factor of Forecasting Tuberculosis (TB) on the basis of District, gender, marital status, age, smoking, history and HIV of TB.
4.2. Study Design
The present study was conducted in the period for Winter January, February, and March (2016) and for Summer July, August, and September (2016) and District at Quetta, Jafarabad, Gawadar, Noshki, Loralai and Lasbela.
4.3. Patient Registration and Microscopy
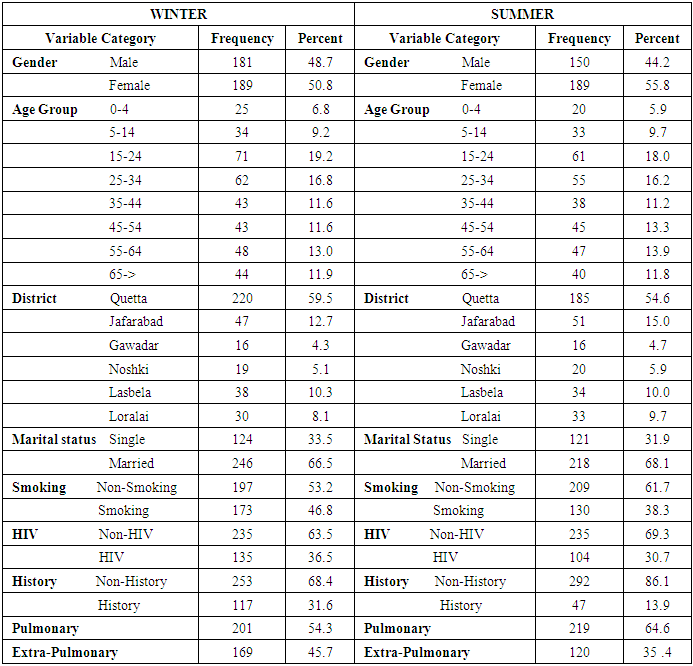
A total of 370 patients were registered in winter in the study period including 181(48.7%) male and 189(50.8%) females of the total cases, and in summer total 339 patients were enrolled in the reading period containing 150(44.2%) male and 189(55.8%) females of the total cases 339. Entirely the patients had come suspected with mutual symptoms, Smoking, HIV, History, Marital Status, Age, Gender, and District.
4.4. Data Collection and Description Analysis
The data were collected from health units of Provincial TB Control Program Balochistan. Demographic information was also recorded from all patients. We further analyzed to check the disease available data of TB for the District, Gender, Age, Marital Status, Smoking, HIV, and History wise analysis.
5. Statistical Analysis
To study probable risk factors for being there in a group with an index patient with Tuberculosis, to calculate Odd Ratio, 95% C.I and P-value we used Logistic Regression, for the categorical variables, and depending on the distribution, a threshold was used to define statistical P < 0.05 significance. All analysis was performed with use of SPSS for windows, Version 22.0. 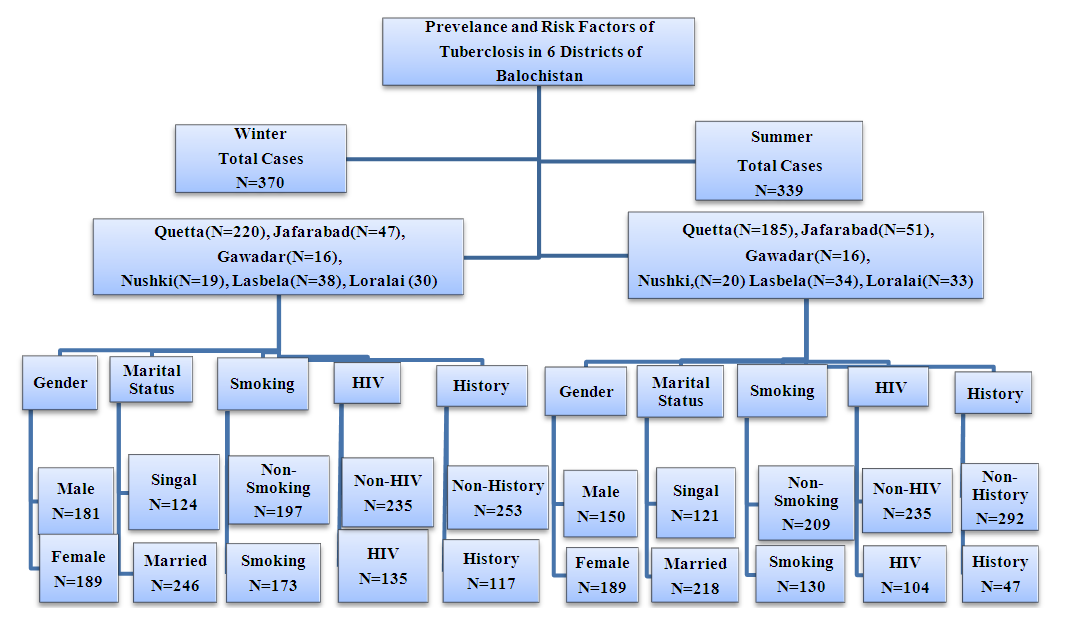 | Figure 2. Flow chart of Prevalence and Risk Factor of Tuberculosis in 6 Districts of Balochistan |
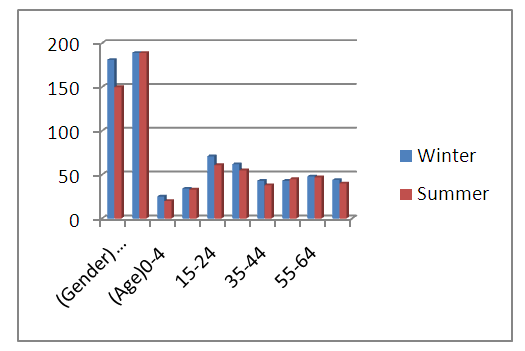 | Figure 3. Age and Gender wise Prevalence of Tuberculosis |
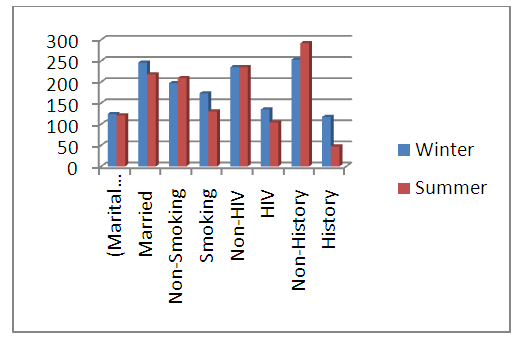 | Figure 4. Overall Risk Factors of Tuberculosis of two seasons |
6. Results
Analysis of the data, age wise, displays that in winter age group 15-24 years the most number, of cases 19.2% was recorded. Additionally closely same no.of cases 16.8% was also notified in the most productive and economically age 25-34 years. While in age group 0-4 year 6.8%, 5-14 year 9.2%, 35-44 year 11.65%, 45-54 year 11.6%, 55-64 year 13.0, and above 64 year 11.9% cases were reported. In the summer the male to female ratio was 150(44.2%) and 189(55.8%), respectively. In winter the high number of patients was registered while the lowest in summer. High prevalence of TB was recorded in Quetta on the basis of percentage. Similarly in summer 18.0% the high number of cases was recorded in age group 15-24 year. Also nearly same number of cases 16.2% was also notified in the most productive and economically age 25-34 year. While in age group 0-4 year 5.9%, 5-14 year 9.7%, 35-44 year 11.2%, 45-54 year 13.3%, 55-64 year 13.9, and above 64 year 11.8% cases were reported [Table 1].Table 1. Socio-demographic characteristic of tuberculosis in a cross sectional study Balochistan, Pakistan
 |
| |
|
 | Figure 5. Gender wise distribution of Pulmonary and ExtraPulmonary Tuberculosis in winter |
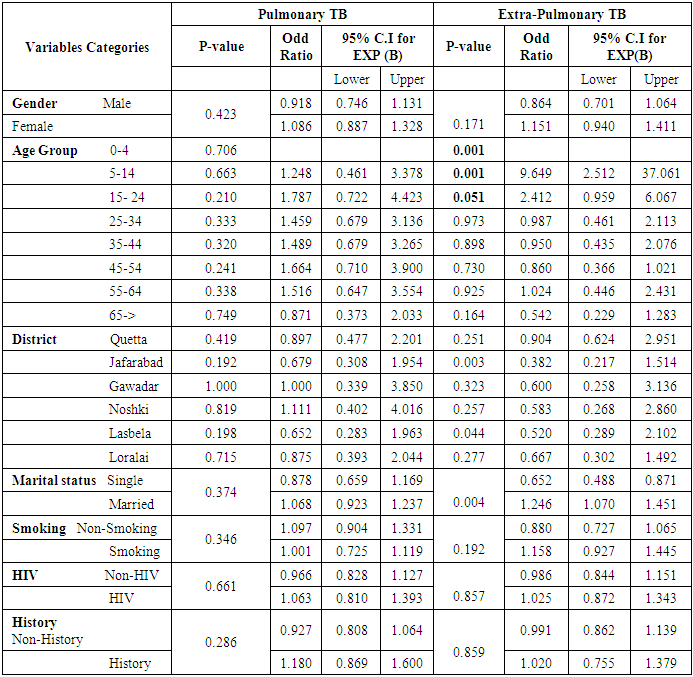
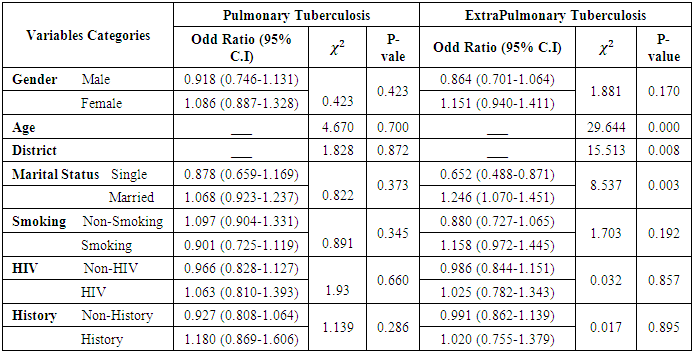
Table 2. Comparison of EPTB and PTB across demographic variables among TB patients in Balochistan (winter) 2016
 |
| |
|
 | Figure 6. Gender wise distribution of Pulmonary and ExtraPulmonary Tuberculosis in summer |
7. Discussion
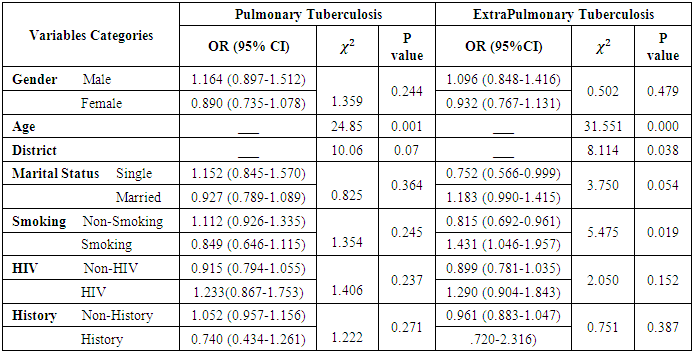
In this study, we aimed to investigate and compare the demographic of PTB and EPTB. Our results indicated that EPTB is almost as common as PTB and it is more likely to affect women. Moreover, both pulmonary tuberculosis and extra-pulmonary tuberculosis seem as disease affecting young adults. The recent study a total 709 patients of TB were recorded at Provincial TB Central Program, Balochistan in which 370 patients were enrolled in Winter, the male to female 181(48.7%) and 189(50.8%) and total 339 patients were enrolled in Summer, the female to male 189(55.8%), and 150(44.2%). In table 2, we applied logistic regression on tuberculosis data to find prevalence of TB with risk factors and demographic, it was found that Smoking, HIV, History, Age, Gender, District, marital Status are associated with TB. The overall prevalence rate of PTB was 52.18%. Almost 48.7% of the male and 50.8% of the female were with tuberculosis. More female were affected by Tuberculosis than male with an OR=0.918, 95% C.I (0.746-1.131) and the female OR=1.086, 95% C.I (0,887-1,328), respectively although no significant difference was highlighted [Table-2]. Age categories between 15-24 and 25-34 years were independent predicators of tuberculosis with OR=1.787[95% C.I (0.722-4.423)] and 1.459[95% C.I (0.679-3.136), respectively] although no significant difference was highlighted. Though there are not any statistical significant values between age group, gender, district, marital status, smoking, HIV, and history with TB. For all these factors the P-value was greater than more than 0.05. In table 2, the overall prevalence rate of EPTB was 52.18%. Almost 48.7% of the male and 50.8% of the female’s studies was tuberculosis. More females were affected by Tuberculosis than male with an Odd Ratio of 0.864, 95% C.I (0.701-1.064) and the female Odd Ratio is 1.151, 95% C.I (0.940-1.411), respectively] although there was no significant difference highlighted [Table-2]. Age categories between15-24 and 25-34 years were independent predicators of tuberculosis with Odd Ratio of 2.412[95% C.I (0.959-6.067)] 0.987[95% C.I (0.461-2.113), respectively] although no significant difference was highlighted. But there was statistical significant between age group 0-4 (p = 0.001), 5-14 (p = 0.001), and 15-24 (p = 0.051) district Jafarabad (p = 0.003), and Lasbela (p = 0.044), marital status (p = 0.004), and smoking (p = 0.041) with TB. The P-vale was less than 0.05 for all these factors. And other risk factors gender, HIV, and history there was no any statistical significant with TB. For all these factors the P-value was more than 0.05. The overall prevalence of Pulmonary TB 48.0%. Almost 55.8% of the females and 44.2% of the males are with TB. By males, females were affected with TB an Odd Ratio of 0.890, C.I (0.735-1.078) and the male 1.164, 955 C.I (0.897-1.512), respectively. Between Age group we have a significant result between aged 15-24 year and 65-> the P-vale of age (25-34) year is (p = 0.004), and also significant result in aged (65->) year P-vale is (p = 0.036), respectively. In district we have significant results in Quetta and Jafarabad district. The P-vale of district Quetta is (p = 0.000), and P-value of district Jafarabad is (p = 0.001). For this age group and district the P-value is less than the 0.05. The other risk factors smoking, history, HIV, marital status, age group 0-4,5-14, 25-34, 35-44, 45-54, and 55-64 for these factors P-vale is greater than and more than 0.05 which is not significant. In Extra-Pulmonary effected with tuberculosis district Quetta and jafarabad has a significant then other district Gawadar, Loralai, Lasbela, and Noshki. The P-value of Quetta district is (p = 0.000), P-value of Jafarabad district is (p = 0.000), O.R is 0.133, C.I (0.217-1.514) respectively; we have a significant value between age group 0-4, 5-14, and 15-24. The P-value of age 0-4 is (p = 0.000), age 5-14 is (p = 0.001), and 15-24 (p = 0.018). We have also significant value in marital status and smoking. In marital status P-value (p = 0.044), and smoking (p = 0.020) (Table 3).Table 3. Comparison of EPTB and PTB across demographic variables among TB patients in Balochistan (summer) 2016
 |
| |
|
Table 4. Binary Logistic Regression (Winter)
 |
| |
|
Table 5. Binary Logistic Regression (Summer)
 |
| |
|
8. Conclusions
The prevalence of risk factors of tuberculosis is very high and female younger age, living in Balochistan districts. The prevalence of risk factors of tuberculosis of female is high as compares to male, living in Balochistan (Pakistan) but the overall prevalence of risk factors of both types of tuberculosis (PTB and EXPTB) for the overall population is significant with geometric progression. Other factors also become a source like HIV, poor livelihood conditions, scarcity of health facilities, etc to being an impact on increasing trend for TB.
References
| [1] | WHO (2014a). Understanding and using tuberculosis data. Geneva: World Health Organization. |
| [2] | Www.bexpress.com.pk march 2018 |
| [3] | Taghizade Moghaddam, H., Emami Moghadam, Z., Khademi, G., Bahreini, A., & Saeidi, M. (2016). Tuberculosis: past, present and future. International Journal of Pediatrics, 4(25), 1243-1254. |
| [4] | WHO. (2017). Global tuberculosis control: WHO Report. Geneva: World Health Organization. |
| [5] | Kyu HH, Maddison ER, Henry NJ, et al. The global burden of tuberculosis: results from the Global Burden of Disease Study 2015. Lancet Infect Dis 2018;18:261–84. |
| [6] | Holt E. Tuberculosis on the political agenda. Lancet Infect Dis 2018;18:30. |
| [7] | Getnet, F., Demissie, M., Assefa, N., Mengistie, B., & Worku, A. (2017). Delay in diagnosis of pulmonary tuberculosis in low-and middle-income settings: systematic review and meta-analysis. BMC pulmonary medicine, 17(1), 202. |
| [8] | de Vries SG, Cremers AL, Heuvelings CC, et al. Barriers and facilitators to the uptake of tuberculosis diagnostic and treatment services by hard-to-reach populations in countries of low and medium tuberculosis incidence: a systematic review of qualitative literature. Lancet Infect Dis 2017; 17: e128–e143. |
| [9] | Dodd P, Yuen C, Sismanidis C, Seddon J, Jenkins H. 2017. Theglobalburden of tuberculosis mortality in children: a mathematical modelling study. The Lancet. Global Health 5: e898–e906. DOI10.1016/S2214-109X(17)30289-9. |
| [10] | Glaziou P, Falzon D, Floyd K, Raviglione M. 2013. Global epidemiology of tuberculosis. Seminars in Respiratory and Critical Care Medicine 34:3–16. DOI 10.1055/s-0032-1333467. |
| [11] | Tilahun G, Gebre-Selassie S. 2016. Treatment outcomes of childhood tuberculosis in AddisAbaba: a five-year retrospective analysis. BMC Public Health 16:612. DOI 10.1186/s12889-016-3193-8. |
| [12] | National Bureau of Statistics of China. Statistical Communiqué of the People’s Republic of China on the 2016 National Economic and Social Development: National Bureau of Statistics of China. Available from: http:// www.stats.gov.cn/english/PressRelease/201702/t20170228_1467503.html. Accessed 17 Oct 2017. |
| [13] | Health—United Nations Sustainable Development [Internet]. http://www.un.org/sustainabledevelopment/health/ (30 December 2016, date last accessed). |
| [14] | Glaziou P, Sismanidis C, Zignol M, Floyd K. Methods Used by WHO to Estimate the Global Burden of TB Disease — Technical Appendix to the Global Tuberculosis Report 2016 [Internet]. Geneva: Global TB Programme, World Health Organization, 2016. https://0x9.me/YqTa1 (26 July 2018, date last accessed). |
| [15] | World Health Oragnization.2017. Global Tuberculosis Report. (WHO/HTM/TB/2017.23). Geneva, Switzerland. Available at http://apps.who.int/iris/bitstream/handle/10665/259366/9789241565516-eng.pdf?sequence=1. |
| [16] | www.bbcurdu.com World TB day. 24 March, 2013. Accessed on 24-3-2013. WHO. (2010). The Stop TB strategy. Geneva: World Health Organization. |
| [17] | WHO. (2010). Global Tuberculosis control report: World Health Organization; 2010. Geneva: World Health Organization. |
| [18] | Khan, J., & Malik, A. (2003). Tuberculosis in Pakistan: are we losing the battle. Med Assoc., 53(8), 320-327. |
| [19] | WHO. (2013). GLOBAL TUBERCULOSIS REPORT 2013. Islamabad: World Health Organization. |
| [20] | Qasim, M. (2016). TB kills over 70,000 people every year in Pakistan. Islamabad: The News. |
| [21] | Pirkani, G. S., Qadeer, E., N, A., Razia, F., Khurshid, Z., Khalil, L., . . . Naeem, A. (2009). Impact of training of Religious Leaders about Tuberculosis on Case Detection Rate in Balochistan, Pakistan. Journal of Pakistan Medical Association, 59(4), 114-117. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML