-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Statistics and Applications
p-ISSN: 2168-5193 e-ISSN: 2168-5215
2019; 9(2): 59-66
doi:10.5923/j.statistics.20190902.03

Survival Analysis of Under-five Mortality and Its Associated Determinants in Nigeria: Evidence from a Survey Data
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAnthony I. Wegbom1, Isaac D. Essi1, Victor A. Kiri2
1Department of Mathematics, Rivers State University, Port Harcourt, Nigeria
2Department of Mathematics, Physics & Electrical Engineering, Northumbria University, Newcastle upon Tyne, United Kingdom
Correspondence to: Anthony I. Wegbom, Department of Mathematics, Rivers State University, Port Harcourt, Nigeria.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Child mortality is a deciding factor of the well-being of a population and often serves as a pointer of the socio-economic status and health development of a nation. A 2017 report on child mortality indicated most child deaths happened in two regions of the world: Sub-Saharan Africa (38%) and South Asia (39%). In Nigeria, around 839,500 children die each year prior to their fifth birthday. This places Nigeria third among the nations of the world with the highest absolute number of child deaths, next to India and Pakistan. Our study is aimed at assessing the effect of socioeconomic, bio-demographic and health-related factors on mortality risk among the under-five (U5M) of Nigerian children, using the 2013 Nigerian Demographic and Health Survey data. We used the non-parametric Kaplan-Meier survival method to assess the influence of the sets of candidate factors on the survival of children aged under-five (U5) and used the Cox proportional hazard model to assess the form of the influence on mortality risk. Those found to have a significant influence on the risk in Nigeria were: mother's educational level, wealth index, marital status, place of residence, sex of the child, region, maternal age at childbirth, number of children ever born, birth interval, and child size at birth. We also found evidence that U5M in Nigeria may be more associated with social, economic, environmental and demographic factors, than with health-related factors. We conclude that for Nigeria to achieve the Sustainable Development Goals, its public health interventions may need to take into account, the factors we have identified.
Keywords: Survival analysis, Under-five mortality, Determinants, Nigerian Demographic and Health Survey, Nigeria
Cite this paper: Anthony I. Wegbom, Isaac D. Essi, Victor A. Kiri, Survival Analysis of Under-five Mortality and Its Associated Determinants in Nigeria: Evidence from a Survey Data, International Journal of Statistics and Applications, Vol. 9 No. 2, 2019, pp. 59-66. doi: 10.5923/j.statistics.20190902.03.
Article Outline
1. Introduction
- Globally, it was estimated that about 5.4 million children aged under-five die each year, with huge variations and trends across regions and nations [1]. A 2017 UNICEF report on child mortality states that most of these child deaths happened in two particular regions: sub-Saharan Africa (38%) and South Asia (39%). Over half of these deaths occurred in just five nations: the Democratic Republic of the Congo, India, Ethiopia, Nigeria and Pakistan. All things considered, 1 out of every 13 children born in sub-Saharan Africa dies before their fifth birthday as against 1 out of every 185 in high-income countries- meaning that the highest proportions of under-five mortality are concentrated in sub-Saharan Africa and South Asia [1]. About 839,500 Nigeria children die each year before their fifth birthdays. This places Nigeria third among the countries of the world with the highest absolute number of child deaths, next to India and Pakistan [2-4].The Millennium Development Goal (MDG) progress report of 2013 revealed that at the national level, only 1/5 of the countries with a high death rate of about 40 deaths per 1000 or more had the chance to achieve MDG Goal 4- the absence of adequate progress in reducing the rates of under-five mortality by many of the developing countries, has resulted in the newly adopted Sustainable Development Goals (SDGs), with the target of reducing U5 mortality to 25 per 1,000 or less by 2030 [5].While U5 mortality rates have dropped globally by about 56%, that is, from 93 deaths/1,000 live births in 1990 to 41 deaths/1,000 live births in 2016, the rate of progress has been unbalanced across nations with the worst in sub-Saharan Africa where accelerated and sustainable improvements are urgently needed [1]. According to UNICEF 2017, in excess of 50 nations, including Nigeria are missing their SDG targets on child survival, and nearly 60 million children under age 5 will die between 2017 and 2030 if current trends continue.Nigeria is among the nations in sub-Saharan Africa with very high under-five mortality [6]. The U5 five mortality rates in 1990 was 201 deaths per 1000, which later dropped to 128 deaths per 1000 in 2013 -marking a 36 per cent drop within the 23-year period. However, this placed Nigeria among the nations that fell far short of achieving the MDG 4 [7]. In any case, there is no evidence that the advancement being made in reducing under-five mortality in Nigeria could be maintained in the post-2015 Millennium Development Goals (MDGs) worldwide plan [8]. In Nigeria, according to the 2013 NDHS report, infant and child mortality is 69 and 64 per 1000 live births respectively. This implies that one in every 15 Nigerian children dies before reaching age 1, and one in every sixteen does not live to their fifth birthday from their first [7]. Factors such as low level of mother's educational level, unsafe sanitation and drinking water, family income, breastfeeding period, birth interval, and place of delivery have been suggested as risks factors of under-five death. This study aims to identify the factors which influence child survival in Nigeria.
2. Materials and Method of Analysis
2.1. Source of Data
- Like other surveys that collect data on birth outcomes, the Demographic and Health Surveys (DHS) is a survey that collects data on under-five mortality assessment in developing states like Nigeria, where adequate and reliable vital registration system is missing [9].The DHS was conducted in 1990, 2003, 2008 and 2013 in Nigeria. This survey is intervallic and cross-sectional directed at the household level. In this study, we used data from the 2013 Nigeria Demographic and Health Survey. The survey is a three-stage stratified cluster design consisting of 904 clusters from which sample of 40,680 households was selected, 45 households in each cluster. A sample of 18,516 women aged 15–49 who had given birth in the past five years preceding the survey was interviewed. Thus, the 2013 NDHS sample was designed to provide estimates for the demographic and health variables at the national level, taking into account, both the rural and urban areas of Nigeria as well as its six geopolitical zones [7].
2.2. Variable Description
- The response variable in this study was under-five mortality as a binary with survival status (alive =0 or dead=1) based on age at death in the last five years preceding the survey. In other words, under-five mortality refers to the death of children below the age of five years [7]. The explanatory variables are social, economic, biological, demographic, and health-related variables. The covariates were selected from Mosley and Chen framework [10] as well as some relevant literature and they were accordingly handled as categorical variables: namely, mother educational level (None, primary, secondary, tertiary), wealth index (poor, middle, rich), marital status (never married, married), religion (Christianity, Isam, others), place of residence (Urban, rural), source of water (unimproved, improved), toilet facility (unimproved, improved), sex of the child (male, female), region (north-central, north-east, north-west, south-east, south-south, south-west), maternal age at childbirth (<25yrs, 25-34yrs, >=35yrs), birth interval (first birth, <24months, 24-35months, >35months), number of children everborn (<=2, 3-5, >6), child size at birth (large, average, small), use bednet (no, yes), place of delivery (public, private, home), and mode of delivery (Cesarean section, other).
2.3. Methods of Analysis
2.3.1. Survival Analysis
- We used survival analytical methods, being the conventional approaches for analyzing survival (i.e. time-to-event) data [11-12]. Survival analysis is primarily for studying follow-up times (years, months weeks or days) to the occurrence of any particular event of interest (death or disease) and the technique is particularly very popular in Biostatistics and Demography. Indeed, these methods are the standard statistical techniques of choice for analyzing censored data (i.e. those that containing missing event dates such as where subjects are lost to follow-up) and also for data where the underlying distribution may not be normal [13].We used the Kaplan-Meier survival technique which is a univariate approach, to identify the effect of each individual variable on the time to death and applied the associated log-rank test to assess the unadjusted effect of each variable on the risk.In general, the first step in the analysis of survival data is usually to estimate the distribution of the survival times, known as failure times. The survival function is used to describe the lifetimes of the population of interest and subsequently, to estimate the adjusted effects of the explanatory variables.
2.3.2. Formulation
- Let the random variable T denote the survival time, and t be the realization of T. Again, let T have a probability distribution function (PDF) of f(t), then the Cumulative distribution function of T can be expressed as
 | (1) |
 denotes the probability that a child survives longer than t from first day of birth and is expressed as:
denotes the probability that a child survives longer than t from first day of birth and is expressed as: | (2) |
 | (3) |
 represents the probability that a child dies at time t, on the condition that he survived to that time. It is the instantaneous death rate at which a child survives to time t:
represents the probability that a child dies at time t, on the condition that he survived to that time. It is the instantaneous death rate at which a child survives to time t: | (4) |
 is the instantaneous change.The survival analysis model used to obtain the adjusted effects of the variables in our study was the Cox proportional hazard model (PHM). The PHM is a useful survival analytical technique for accessing the influence of relevant factors on the hazard function. The continuous random variable denotes the lifetime t of a child and X as the vector of explanatory factors. The PHM
is the instantaneous change.The survival analysis model used to obtain the adjusted effects of the variables in our study was the Cox proportional hazard model (PHM). The PHM is a useful survival analytical technique for accessing the influence of relevant factors on the hazard function. The continuous random variable denotes the lifetime t of a child and X as the vector of explanatory factors. The PHM | (5) |
 | (6) |
 is the risk of death for child i at time t;
is the risk of death for child i at time t;  is the baseline hazard function;
is the baseline hazard function;  , are the selected variables;
, are the selected variables;  is the vector of unknown coefficients of the explanatory variables xi.The key assumption of the Cox regression model is that the risk for child i, is proportional to the risk for any other child j. That is, the ratio of their risks (i.e. the hazard ratio) is constant over time t.If the vector
is the vector of unknown coefficients of the explanatory variables xi.The key assumption of the Cox regression model is that the risk for child i, is proportional to the risk for any other child j. That is, the ratio of their risks (i.e. the hazard ratio) is constant over time t.If the vector  then the hazard function for the ith individual becomes the baseline hazard function. However, for any other value of
then the hazard function for the ith individual becomes the baseline hazard function. However, for any other value of  , we can divide both sides of equation (5) above by
, we can divide both sides of equation (5) above by  to obtain
to obtain  | (7) |
3. Results
3.1. Univariate Survival Statistics
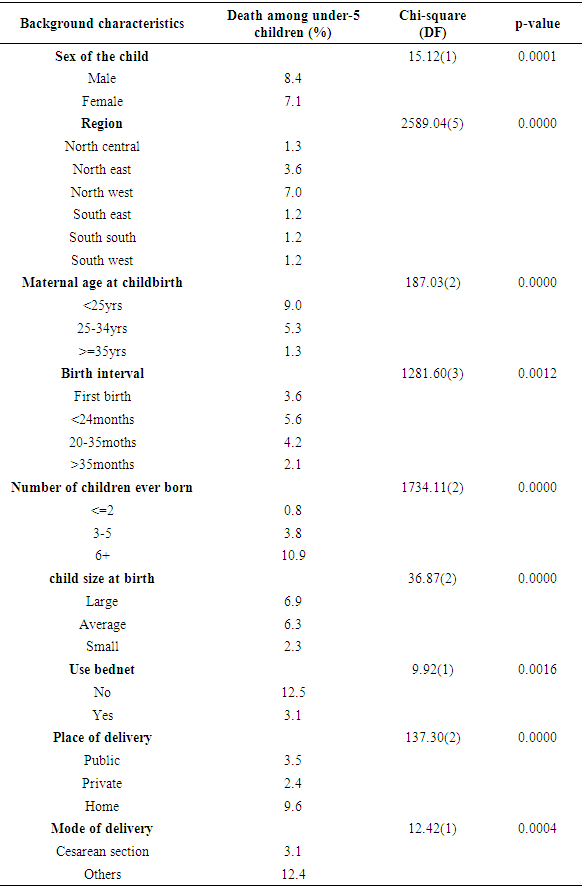
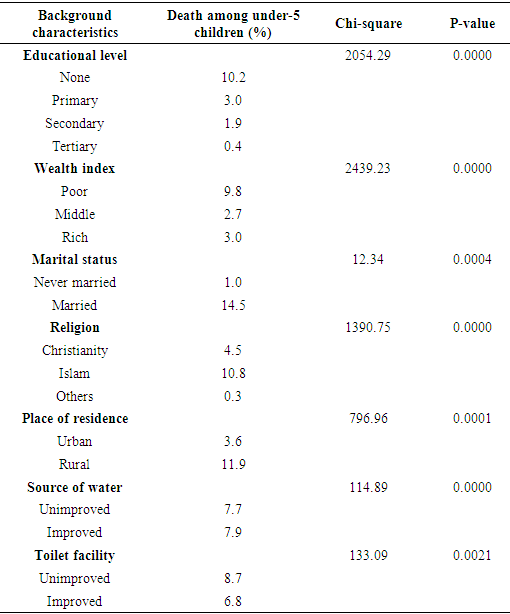
- Table 1a and Table 1b show those among the list of bio-demographic and health-related variables and the socio-economic variables respectively, on which we found evidence of association with the risk of under-five mortality based on the log-rank test (i.e. p< 0.05). The two sets of results suggest the following variables as possibly associated with the risk of death before the age of five: namely, the sex and size of the child, geopolitical region, the maternal age of the mother at birth, the birth interval, number of children ever-born, usage of bednet, place and mode of delivery, the educational level of the mother, wealth index, marital status, religion, place of residence, source of water, and toilet facility as possibly associated with the risk of death before the age of five.
|
|
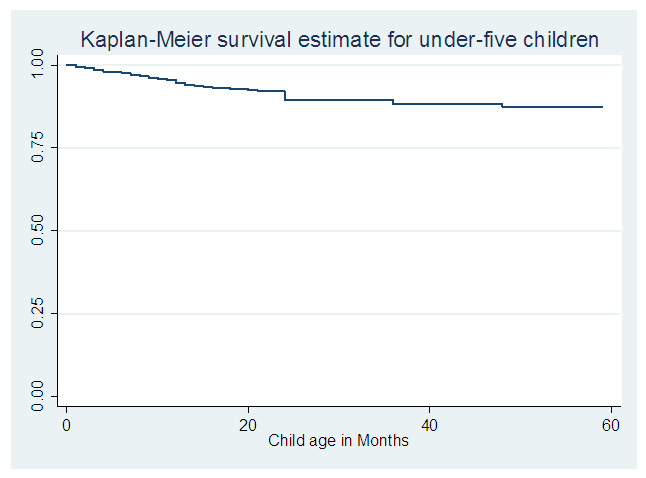 | Figure 1. Plot of the overall Kaplan-Meier estimate of the survivor function for the under-five children in Nigeria |
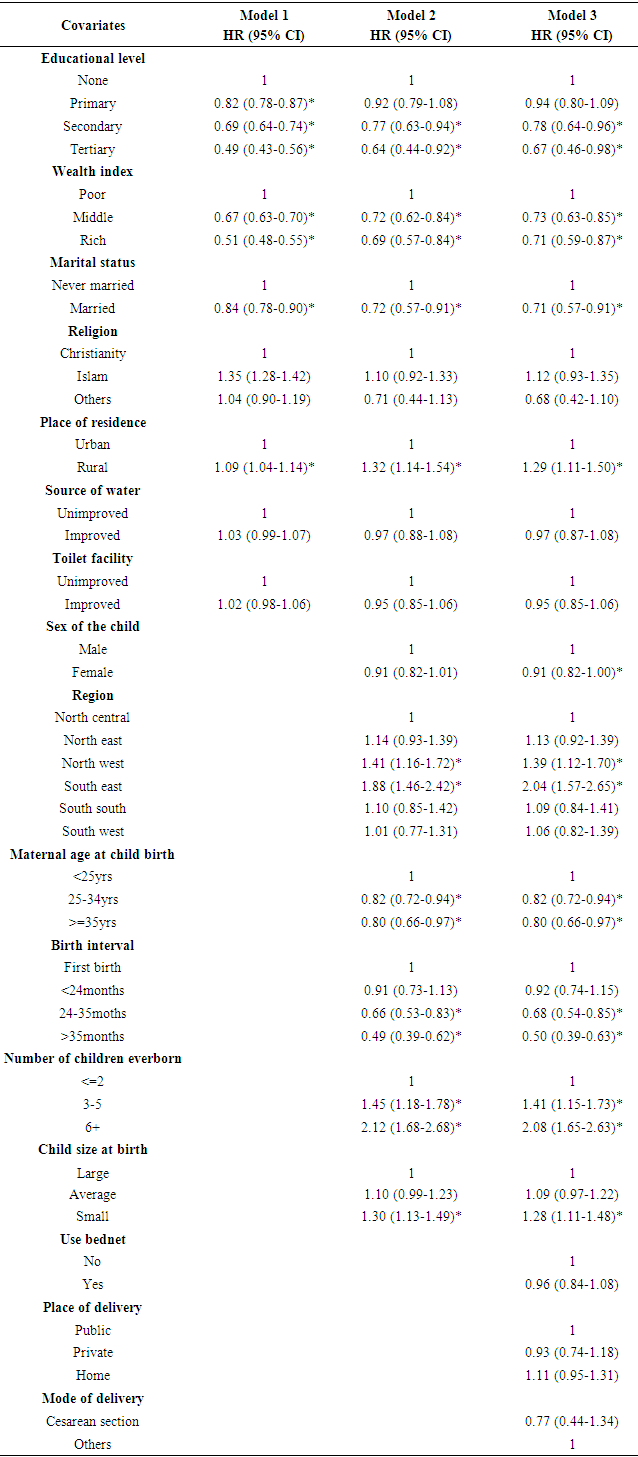
3.2. Risks Factors of Under-Five Mortality
- Table 2 shows the risk factors associated with under-five mortality in Nigeria based on three forms of the Cox proportional hazards model. Model 1 involved only the socio-economic variables, whereas model 2 additionally involved the bio-demographic variables but without the health-related one. Finally, model 3 included all three sets of variables, namely the socio-economic, bio-demographic and health-related types. The results indicate the following as significantly contributing to the risk of under-five mortality in Nigeria: namely, the educational level of the mother, wealth index, marital status, Place of residence, Sex of the child, Geographical Region, Maternal age at childbirth, Birth interval, Number of children ever-born, and the Size of the child at birth.
|
4. Discussion
- In recent years, the under-five mortality rates have been declining consistently in Nigeria which indicates a level of progress in the quality of life. These rates are additionally vital to public health programmes in Nigeria [1, 7, 10]. The results of this study suggest that the risk of Under-5 death depends greatly on a number of socio-economic, bio-demographic and health-related variables, such as mother educational level, wealth index, marital status, place of residence, gender, geopolitical region, mother's age at birth, preceding birth interval, number of children ever born, and the size of child at birth.Mother’s education had a significant relationship with child survival. Higher risks of children death were identified among the illiterate mothers compared with literate mothers: mothers with secondary or higher education mothers. This is consistent with the findings by others [13-17]. A possible explanation could be that educated mothers have better socioeconomic status, better knowledge on family health and childcare, preventive care, effective use of modern health services and good management of child illness [18]. According to O’Toole, education additionally changes the customary and social familial relationships as regards decision making and engages the mothers in several issues like childcare which plays a role in reducing child mortality [19].Substantial disparities in mortality risks were also observed by maternal age at the birth of the child. We found evidence of a higher risk of death for children of younger mothers and this also confirms the findings by previous research [20-23]. Mother’s age at the birth of a child can influence child mortality through different standpoints: the higher risk of child death among younger mothers may be attributed to immature reproductive systems and less stability to handle the complexities of pregnancy [14]. Furthermore, we found the marital status of the mother as related to the risk of child death. There is a low probability of children of married mothers dying compared to those born to never-married mothers- this was also the finding by an earlier study by one of the authors in rural Nigeria [21]. The risk of under-5 mortality was similarly lower for female children. This is in line with the findings of other studies which have suggested girls as more biologically advantaged than boys in terms of many of the causes of death [24-25, 17]. We also found evidence that the length of proceeding birth interval and the number of children ever-born were associated with the risk of death before the age of five. On birth intervals, we found evidence that children delivered within shorter birth intervals were at a greater risk of dying before their fifth birthday. Thus, agreeing with the findings by some previous studies [26-29, 16, 21, 23, 14, 17]. A possible explanation is that shorter length of the birth interval may negatively influence maternal health, by increasing susceptibility of infectious diseases and competition in familial resource among children [27].Our findings showed that survival of children to their fifth year in life was significantly worse among children residing in the north-west and south-east parts of Nigeria than those residing in the North central and other part zones. This high risk might be attributed to social improvement in the community, population density, territorial advancement, as well as regional economic resources [17, 30-32]. We also found evidence that the place of residence of the mother and her wealth index might influence the survival of her child before the fifth birthday. On the wealth status of the household, we also found evidence that mortality risk in this age group might be lower in wealthy households as compared to the underprivileged households. This was consistent with the findings by some previous studies [33-35]. These households have better housing conditions, better nutrition, more empowerment and hence they may be able to afford better medical attention and care thus significantly enhancing the survival probability of all their children [33]. Our study also found evidence that the child’s size at birth might be significantly associated with infant mortality. Although the size at birth may not be so important once a child survives beyond the first year of life, timely intervention in the form of promoting breastfeeding and micronutrient interventions is recommended for stunted and underweight children, particularly during the neonatal period and late infancy [36-38]. Indeed, Uthman had noted that underweight children are more vulnerable to infections and other related diseases [39].The size of the child at birth was found to be associated with high U5M and the evidence also supports the findings by others that small sized children at birth have a higher risk of dying before the age of five [17, 36-39]. This might be due to the immaturity of their organs which makes them find it more difficult to adapt to eternal, independent life. Most premature babies are prone to have sepsis which is one of the major causes of Under 5 Mortality [30].Furthermore, our study suggests that mortality rates are higher in rural areas. This concurs with previous studies in and outside Nigeria [40-43, 30, 17]. This is on the ground that those living in the urban areas have access to improved water supply, improve sanitation facilities, unlimited access to healthcare as well as other social and economic services [30, 43].
5. Conclusions
- The findings from this study have essential policy implications, particularly in monitoring public health interventions which need to ensure a consistent decline in child mortality rates, towards the achievement of the SDG 3. In this study, we explored and then identified the socioeconomic, bio-demographic, and health-related factors that might influence the risk of U5M in Nigeria, using the method of time-to-event (i.e. survival) analysis. The results from the Cox regression models showed that mother educational level, wealth index, marital status, place of residence, gender, geopolitical region, mother's age at birth, preceding birth interval, number of children ever born, and the size of the child at birth might influence the risk of child mortality in Nigeria. In a nutshell, these findings suggest that under-five mortality is greatly associated with socio-economic and bio-demographic factors in addition to those already known as health-related.