Bukola Badeji – Ajisafe
Department of Mathematical and Computer Sciences, University of Medical Science, Laje Rd, Ondo City, Nigeria
Correspondence to: Bukola Badeji – Ajisafe, Department of Mathematical and Computer Sciences, University of Medical Science, Laje Rd, Ondo City, Nigeria.
| Email: |  |
Copyright © 2018 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
It has been recorded that family planning was in practice for a long time ago, even though high premium was placed on giving birth to many children. This was because the possession of children is regarded not only as a powerful tool but as a mark of wealth in the community. Increase in population in Nigeria has created a lot of havoc in which Ekiti State shared in this predicament. Therefore this study examined the attitude of Ekiti State inhabitant to Family Planning. The study adapted non – experimental type of research. It was a descriptive research. Five research question guided the study. Purposive sampling technique was used to select 150 men and women and 10 family planning health officers as participants. Two validated research instruments were used to collect data which are: questionnaire for men and women, interview schedule for family planning health officers. Data were analysed using qualitative method (thematic approach) frequency counts percentages, and ANOVA. Result shows that people living in urban area have better attitude to family planning:  than those in rural area
than those in rural area  with the significant F(2,149) =(2235.688, P < 0.05). It was also reprinted that university graduated have better attitude to family planning
with the significant F(2,149) =(2235.688, P < 0.05). It was also reprinted that university graduated have better attitude to family planning  than secondary school graduate
than secondary school graduate  The result further reveal that socio – economic level do not have much effect on people attitude to family planning F(2,149) = 4.596, P < 0.05. also result showed that religion belief do not have influence on people attitude to family planning. Christianity
The result further reveal that socio – economic level do not have much effect on people attitude to family planning F(2,149) = 4.596, P < 0.05. also result showed that religion belief do not have influence on people attitude to family planning. Christianity  Islam
Islam  and traditional
and traditional  Result also reveals people in urban area are more aware about family planning that other location. Urban
Result also reveals people in urban area are more aware about family planning that other location. Urban  semi – urban
semi – urban  Rural
Rural  Based on the finding it was concluded that the attitudes of Ekiti people on Family Planning is negative/poor. It is recommended that individual should key into Family Planning in order to increase their standard of living and boost their economy status. Also, the government at all levels should intensify efforts in creating more awareness on Family Planning to Ekiti people.
Based on the finding it was concluded that the attitudes of Ekiti people on Family Planning is negative/poor. It is recommended that individual should key into Family Planning in order to increase their standard of living and boost their economy status. Also, the government at all levels should intensify efforts in creating more awareness on Family Planning to Ekiti people.
Keywords:
Family Planning, Prevention, Birth Control
Cite this paper: Bukola Badeji – Ajisafe, Attitude of Ekiti State Inhabitants to Family Planning, International Journal of Statistics and Applications, Vol. 8 No. 3, 2018, pp. 133-143. doi: 10.5923/j.statistics.20180803.04.
1. Introduction
Family planning is one of the components of primary health care that is supposed to reduce maternal and child mortality rate and prevents unwanted or unplanned pregnancies. It is a way of spacing and limiting the number of children in the family set up. Family planning could be defined as the deliberate influence adopted by individuals and couples in order to limit birth in such a way that wanted births supercede unwanted births. Ritz (2013) said the health benefits of family planning associated with child spacing and the use of specific methods can play a major role in protecting the lives of infants, children, women and the family as a whole.The death of a mother is one of the most traumatic events that can befall a family and has an immense impact on the emotional well being of the family members that survive her. It may also affect the physical health of survivors since a 3rd of African women earn a living and since woman are directly involved in the hygiene and sanitation of children, child spacing can protect a woman in significant ways. Lindesay (2013) said during the process of receiving family planning services, illnesses can be detected and treated early which can reduce the likelihood of long term debilitating problems. Also if family planning services are linked to other family health or maternal/child health services, high risk pregnancies can be detected and referred for special assistance.Moreover, by spacing the children, a woman can avoid high risk pregnancies when women use. Contraceptive method effectively, she is less likely to result to dangerous illegal abortions. In Nigeria, the problem of uncontrolled fertility has increasingly become a burden although the federal government believes that the countries population problem is unlikely to be such that calls for extensive emergency. Nigeria is by far the most populous in Africa and among the ten most populous countries in the world. It was established in 1992 that the population had reached about 140million, an increase of 76% over the past 22 years. Then the projection indicated that the population could reach about 165 million by the year 2000 and 280 million by the year 2015.Uncontrolled population has consequence and implication for mortality:-(1) On agriculture – there will be no sufficient land to cultivate thereby resulting in shortage of food / starvation and malnutrition.(2) Education- the current high birth rate and the momentum of population growth also tend to increase phenomenally. It is obvious that as more pupils are, much larger expenditure will be required to pay for the increasing needs for teachers, school administrators, managers, school building, equipment and class rooms.(3) Employment- with the current economic situation in the country, it would be most difficult to create enough jobs for such a large number of people, thus the nations problem of unemployment especially in the modern sectors of the economy may be further aggravated.(4) Health – the goal of the federal government is to provide adequate health care services for the entire population through the expansion of primary health care by the year 2000, but the continued rapid growth of the population is likely to make the achievement difficult or perhaps impossible. Though the total population will increase tremendously but also the number of high health risk persons (such as children under 5 years of age and women in their child bearing years) will grow rapidly, therefore making it difficult to provide enough basic health services and facilities for entire population.(5) Environment the present high rate of population growth is already contributing to over crowding, scarcity of food and variety of diseases resulting from inadequate food. Such as malnutrition and anaemia.Statement of problemReactions or attitude of the inhabitant of Ekiti community to family planningDefinition of termsThese are the operational definitions of the concepts used in the work in other to ensure uniform understanding and interpretation of tenses.1. Family planning: is a method of spacing children, prevention of unwanted pregnancy and prevention of sexually transmitted diseases.2. Contraceptives: various methods used to prevent unwanted pregnancies.3. Sterilisation: this is the sexual ligation of the fallopian tubes in the female and tying and cutting of vas – deferences in the male, to prevent union of both the ovum and the spermatozoa.4. Abstinence: keeping away from sexual intercourse in order to prevent pregnancy.5. Charm: substance believed to possess magical powers capable of preventing pregnancy.6. I.U.C.D: foreign objects introduced into the uterus of women to prevent embedding of the ovum.7. Injectables: these are chemical substances given intramuscularly to women to prevent fertilization from taking place.8. The pills: both combined and mini pills are chemical substances in tablet form taken by women to prevent pregnancy.
1.1. Purpose of Study
The purposes are:1. To examine the attitude of Ekiti state inhabitants to family planning techniques or programme.2. To examine the influence of sex on attitude of the inhabitant of Ekiti state on western oriented family planning technique.3. To examine the effect of age and level of education on the attitude towards western oriented family planning.4. To assess the level of success of western oriented family planning technique in Ekiti state and finally to investigate how the programme can be improved upon.
1.2. The Importance of the Study
Information to be derived from this study will not only help in educating planning literacy and health education for people of Ekiti state but will also help in updating our knowledge about family techniques as practiced in Ekiti state thereby helping the ministry of health to reformulate the best policy to make the programme more acceptable to people of Ekiti and similar socio cultural communities in Nigeria.
1.3. Limitations
The study has its limitations such as:-1. Time- the time allocated was short fours weeks is not enough to collect adequate information.2. Financial constraint- there was a financial problem since a lot of money was needed for the project as the study was limited to Ado Ekiti local government area. As a result of increase in transport fare and the economy of the clients, the researcher had to carry out the research in the hospital, local government maternity to get enough clients for the study.
1.4. Basic Assumption
The researcher assumed that the people’s response to the truth and reality.
2. Literature Review
It was widely accepted in the past that the larger the family, the more the people to cultivate the land. The more the people to cultivate the land, the more the males in the community, the stronger the ability to resist inter-tribal attacks, and the more females, in the community, the larger the yearly birth rate of children Hansen Z 2005. These benefits coupled with the fact that infants death rate was very high necessitated a general desire to produce many children. High parity was thus the rule because it was conceived that since many infants were likely to die, some others would at least be available to survive. Today there is a gradual change. The impact of advanced medical care, sanitation, good water supply and good nutrition has led to more infants surviving rather than dying. This change for better implies that a couple can afford to have fewer children because they are confident that all would survive and be reared to puberty.Theoretically the above statement is true for the more affluent society but it is not entirely true for underdeveloped or developing countries. High birth rate is still the rule among the poorer class for example, the poorer and lower educational background of a couple, the higher the birth rate while the higher the income and the more civilised and urbanised a couple, the smaller is their desired family. History has it that men’s ability to control their fertility date back to the stone age where various practices of limiting the growth of the population were used. Birth therefore is as old as mankind. Our fore fathers recognised the need for spacing child birth through traditional methods that were applicable to them.In the early days, all efforts to control birth were directed to the women because babies were considered the product of the woman. Several number of birth methods were used which proved that control is nothing new in the world today especially in the developed countries. People may ask about God’s will about family planning. It is a matter of conscience, it is the motive which counts before God not the methods or means. The important thing is that the father and mother together make such a decision. Both have to examine their conscience before God as to their motive because they are both responsible to God. This is what is called “responsible parents”. If anyone fails to provide for his family, disowned the faith, and is worse than unbeliever.
2.1. Why do We need Family Planning
Family planning is very important to health, survival and development of the family. The woman who bears too many children or does not leave enough time between child bearing tends to suffer adversely both physically and mentally. Gupta et. al., 2004. It is therefore very important for a woman to have an interval of two and half to three years between pregnancies and also 3 – 4 children in order to avoid unnecessary complication during pregnancy, labour and delivery. This enables the woman to have healthy children who will stay alive, to play her role as a mother and wife and also contribute to national development.The effect of too many children on health of the father is very grave. The father have to over work himself in order to provide for the family needs and this results in stress / anxiety tiredness and general debility mental strain and hypertension all these combine to reduce the fathers chance of survival or living a normal life. Richardson et. al., 2011 said that the socio economical reasons good living for a family is an enough reason for family planning.Ritz (2013) in the journal said that having many children is really a great burden that drains the financial resources of the family with subsequent poverty, drop in the standard of living and economic hardship. This results in poverty in old age and absence of the traditional expectation of charity contributions from the children who were probably set up in life to assist in maintaining their parents. Family planning enables parents to save and plan for their old age.Good education yields the best interest and it is one of the greatest and most precious gifts any parent can bestow on their children. This calls for equal love devotion, commitment, guidance and understanding on the part of responsible parents. It is a fact that marriage is not only for procreation but for love, companionship which is the highest expression of physical love which is peculiar to human being would be well adjusted. The fear of unwanted pregnancy which could lead to abortion maternal death and psychological stress would be avoided. Family planning helps to keep the family happy and affords the family/couple the opportunity and leisure to enjoy each others company. Family planning promotes self respect and contentment. It allows the individual to set a goal and achieve it.The role of family planning in any community or nation cannot be over emphasised Bhasin et. al., 2005 says when the population increases fast, provision for socio amenities like electricity, housing, good health services, education, good water supply, employment and improved technology cannot meets of the people. The economic recession which now plaques the developing countries could have been minimised partly if adequate steps have been taken to educate the masses about the consequences of a rapidly growing population. It is therefore important that family planning be considered to attain stability, even though family planning does not solve all problems but without it solutions to some problems may be impossible.Methods of birth control used before the advent of this modern family planning techniques:- these are sub divided into main headings:a. Use of herbs and plantsb. Behavioural practices.(1) Use of herbs and plants - this includes women drinking concursion made from various kinds of roots, weeds, trees and leaves to prevent pregnancy.(2) Gbere - (Scarification) these are marks made on the skin into which powdery concursion is rubbed. The concursion is stored in a special small gourd.(3) Rings - this is made of metal or copper kept in paw-paw to mature, when the pawpaw ripens, the ring is taken out and worn either by the man or woman to prevent pregnancy.(4) Igbadi or ifunpa - this is a waist or armlet charm made of leather worn by the woman to prevent pregnancy.(5) Teso - this is a device (charm) placed on the floor to make a woman pass over rendering her impenetrable. It may be feather or a piece of string.(6) Akaraba - this is a padlock in which incantations used during sexual intercourse, it means the womb of the woman is open and can become pregnant when the padlock is open but when it is locked(7) Esu – this is made of horn of animal with a special feather. It is placed under the pillow, or around the house or handled by man during sexual intercourse to prevent pregnancy.(8) Omolangidi – this is a wooden doll in which incantation have been made. It is placed on the door post in the room or under the pillow during coitus.These are some of the ways they use in the past and some are still in use. Most of the methods unpredicatable and unscientific. There is an element of faith healing and a lot of myth surrounding their efficacy like in many traditional beliefs of the people.Behavioural practices includes –1. Polygamy2. Prolonged lactation3. Separation of pregnant woman from their husbands.(i) Polygamy – this enables the husband to satisfy his sexual urge with another wife who is not nursing a baby thus allows the nursing mother to abstain from intercourse as she can be isolated from her husband.(ii) Separation of pregnant woman from their husband – once the woman is pregnant, she can be sent to the village or farm to stay with the mother inlaw until she delivers and the childs age is about three years old when the woman will be sent back home to the husband for possible pregnancy.(iii) Prolonged lactation – it is a taboo for nursing mother to resume sexual activities after child birth until the child is twpo or three years old. This led to adequate spacing of birth.(iv) Total abstinence – avoidance of sexual intercourse is the most effective method of birth control provided, it is strictly and honestly practiced. It is by personal choice or culturally or religiously enforced.The above available information on traditional methods of birth control indicates beyond reasonable doubt that family planning is not new in the African continent. It is of interest to know that the world health organisation in collaboration with some traditional healers embark on various studies designed to find out about traditional method of birth control and other traditional medications.Through intensive research both experimental and clinical, modern methods of birth control emerged in an attempt to minimise complications, develop effective non injurious, convenient reliable, palatable easily accessible and accepted method that would meet the need of individual of couple.A variety of modern methods of contraception’s is currently available with minimal side effect, religious and cultural resentments.The knowledge and use of modern contraceptives – the knowledge of various type of modern family planning is very important because it will assist the individual or couple to choose any one they like.i. The following points should be considered when deciding family planning methods –What is it?How does it work? Who should use if? How is it used? Side effect, Advantages and disadvantages, Complications, Availability,ii. Various methods of family planning –WithdrawalSafe periodSpermicidesDiaphragm with spermicidesCondom with spermicidesIntra uterine deviceOral contraceptivesInjectables contraceptivesImplantSterilization1. Withdrawal methods – this is the oldest method of birth control, it involves the man withdrawing his penis from the virginal during intercourse just before ejaculation. The semen is then discharged outside making sure it does not discharge into the virginal.2. Contraindication – failure to withdraw in time and inability to control ejaculation.3. Side effect – there tension anxiety and sexual dissatisfaction.4. Advantages – it is better than nothing. It cost less, it needs no preparation and no prescription.5. Disadvantages – it creates emotional disturbance for both male and female partners. The female is always in fear that the male may not withdraw in time and the man must be very vigilant so as separate. It is one of the desirable features of intercourse which is unavoidable tension which may result in impotent in the male and frigidity in female or a state of nervous tension in both.6. Complications – unwanted pregnancy.7. Safe period – this means that the woman should know ovulation period and abstain from sexual relationship during the period. This is a natural family planning which needs a high measure of intelligence.8. Contra – indication – inability to identity the signs and symptoms of ovulation. Irregular menstrual cycle. Lack of cooperation from partner. Inability to remember or learn the technique.9. Point to know – you must know the ovulation period which is the middle of each cycle, i.e. 14 days before the next period is considered as ovulation day.- That the life span of the ovum is 36 – 48 hours.- That the sperm can only survive in either the tube or uterus for 48 – 72 hours after ejaculation into the virginal.The woman must be able to keep a menstrual diary for a period of 6 – 12 months. She must be able the calendar method. For a woman with 26 – 28 days regular cycle, you substract 18 from the shortest cycle to determine the first unsafe day and 11 from the longest menstrual cycle to determine the last unsafe day, that is (26 – 18 = 8) the safe period during (29 – 11 = 18). The first 7 days and the last 10 days of menstrual cycle is the safe period.iii. Spermicides or vaginal contraceptives –These are preparations composed of materials which physically block the sperm and active spermicidal agent which chemically destroy the sperm.Types: there are four types:1. Foaming tablets2. Cream3. Jelly4. SuppositoryVirginal contraceptives even though useful in many situations, they are nevertheless not advocated as a primary method of family planning programme.Advantages: it is simple to use and is portable. It is easy to purchase without prescription. It decreases the transmission of sexually transmitted disease.Disadvantages: it is very messy it has to be reapplied each time there is need for intercourse.Complications: none as at now.iv. diaphragm – it is a mechanical barrier mother of birth control made of soft done shaped rubber resembling a cap with a flexible metal spring at the outer edge. It is introduced into the virginal before intercourse to prevent the sperm from entering the cervical canal thereby preventing pregnancy. The spermicidal cream and the jelly should be applied along in the diaphragm.Side effect: allergy to rubber or reaction to spermicidal, Irritation from spermicidal use. Virginal discharge if it stays long before it is removed or if it is not well cleaned.Advantages: it protects against sexually transmitted diseases. It is portable. It can be controlled by the user. It is inexpensive if well taken care off.Disadvantages: the user must be measured so as to have the correct size by the family planning doctor or nurse.v. Condom: This is also known as durex or sheath. It is rubber like balloon worn over the man’s erected penis before intercourse to prevent pregnancy by collecting and preventing the entry of the spermatozoa into the virginal.Condom prevents both man and woman free of sexually transmitted diseases. The side effect is minimal; the failure rate is about 10%. There is no need for supervision.vi. Intra – uterine coil device (I.U.C.D): It is made of variety of materials such as silver, copper, and plastic, some contains progesterone and some do not. It is in form of a spiral or sling form of non – medicated lipped loop and medicated copper “T” (C U T) coils of various types and sizes of various types and size to be placed inside the uterus to avoid implantation of the fertilized ovum and prevent conception. It is most widely used in Africa and throughout most of the rest of the world. They are used by some 60 million women throughout the world. It is highly effective. It does not interfere with intercourse and does not interfere with breast feeding.The possible side effect: it needs an expert to insert it. It is not meant for young girls who have never been pregnant but are sexually active, but should use another method unless it is absolutely necessary and it is the only method that can be used.viii. Oral contraception: the pills are in two forms, one contains progesterone only and the other contains progesterone and oestrogen. They are used by some 50 million to 100 million women throughout the world. In many Africa countries, the pill is the most popular method of contraception. It is reliable if taken as prescribed.They suppress ovulation, they make uterus unsuitable for attachment of the fertilised ovum. It makes the cervical secretions thicker thereby prevents the spermatozoa from entering the uterus.It is taken orally for 21 – 28 days to prevent pregnancy. Sides effects is mainly nausea and vomiting, weight gain, fullness of breast and palpitation.viii. The injectables: this contains long acting progestron given at intervals varying from 2 to 3 months.The common ones are: (1) Mechroxy – progesterone acetate (Depo – Provem or DMPA).(ii) Norethindrone enanthate (Net or Nonsterat). The use of injectables progestives has been effective and popular in a number of African countries due to the fact that it has been found convenient, allows for privacy and furthermore there is a traditional belief that injections have a greater effect than oral medication.xi. The implantation: the progesterone is impregnated into 6 tiny sialastic capsules are implanted beneath the skin of the arm of the woman to provide her with effective protection against pregnancy for 5 years or longer. The major problem however is that the placement and removal involves minor outpatient surgery under local anesthesia once it is in place, the implants are barely visible beneath the skin.x. Impregnation: this could either be impregnated into I.U.D known as progesterone T to increase the contraceptive effectiveness and decrease uterine cramp and total menstrual blood loss, or progesterone is impregnated into virginal ring pessary, worn by the woman for 21 days. The ring releases progesterone: that are systematically absorbed. The round ring slightly smaller than the regular diaphragm is placed into the virginal vault each month after menses, like diaphragm and left in place for 21 days, after 3 months of effective use, the ring is replaced. Both the impregnated I U D and the virginal ring are still being experimented on at some universities in Nigeria.xi. Virginal spouse: is a small pillow shaped poly – urethane sponge which contains 1 gram of nonoxynol 1-9 spermicidal. It is concave dimple in one side which fits over the cervix and increases the chance of dislodgement during intercourse. It is available in one size only and provides 24 hours continuous protection without additional measures for repeated intercourse. It should be used once and discarded. Mechanism of action: it provides mechanical barrier between sperm and cervix while the chemical barrier destroys the sperm trapped within the sponge. It is available only in developed countries.xii. Sterilization: it is a surgical intervention and permanent method of birth control performed on the woman or on a man who has decided to put an end to the child bearing. It is the cutting and closure of the fallopian tube in the woman and the cutting and tying of the vas – deference of the man. This prevents the ovum from entering the uterus and also in men the sperm cannot gain entry into the virginal. Both the ovum and the sperm are absorbed into the body without any adverse effect.It is once and for all methods. It does not carry any risk of life. It does not interfere with health nor does it have any adverse effect on sexual activity.It is highly effective. The decision to use this method must be strictly that of the couple and it is mandatory that the client be counselled and consent, obtained in view of its irreversibility.Lastly, it is clearly evident that contraceptives methods are not 100% effective, except for total abstinence. However, researchers are intensifying efforts all over the world to find a method that would meet the criteria of an idea contraceptive.It is very important for all health workers to keep abreast with contraceptives technology in order to be able to provide detailed information and guidance to clients Delano (1989). This would assist the clients in a decision on the choice of contraceptive bearing in mind that the best method is the one that not only agrees with the user but that makes her feel comfortable.
3. Research Design
This study adopted a non – experimental type of research. It was a descriptive research. This design was deemed appriopriate because the study considered the attitude of Ekiti State inhabitant to Family Planning. And there was no random assignment or manipulation of variables (Kelinger and Lee, 2008).
3.1. Population
The population of the study consisted of the health officer, of Ekiti State and men and women of Ekiti State.
3.2. Sample and Sampling Technique
A purposive sampling technique was used in select participant for study. From Ekiti senatorial district ten health officers of the state hospital were chosen. On e hundred and fifty (150) men and women were randomly selected for the study.
3.3. Research Instruments
Two research instruments were used to collect data for the study. These were properly validated and their cronbach Alpha reliability coefficients established statistically before they were used for data collection.The instruments were:1) Questionnaire for men and women on family.2) Interview schedule for family planning health officers.
3.4. Data Collection
The researcher collected data from three locations (rural, urban and semi-urban) with the research instruments.
3.5. Method of Data Analysis
Data for the research where analyzed using qualitative and qualitative methods make use thematic area, an qualitative. Multiple regression were used to analyse resulting data in order to answer the state research questions
4. Results and Discussion
4.1. Research Questions 1
Does the environment affect the attitude of people to family planning.Predators (constant) urban location reason for family planning, location family planning, semi location family planning, urban location awareness, rural location type of contraceptive, urban location problem of contraceptive, semi location problem of contraceptive, rural location awareness, semi location reason for family planning, semi location type of contraceptive, urban location type of contraceptive, urban location family planning, semi location awareness, rural location reason for family planning, rural location problem of contraceptive.Multiple regression analysis was conducted in order to show how environment affect the attitude of people to family planning Chaithanya et. al., 2014. The result in table 4.1 an 4.2 show the multiple regression coefficient [R] which indicate that a linear relationship exists, between fifteen predictors [Rural awareness, Semi urban awareness, urban awareness, Rural types of contraceptive use, semi types of contraceptive use, urban type of contraceptive use, rural problem of contraceptive, semi problem of contraceptive, urban problem of contraceptive, rural family planning, semi family planning, urban family planning rural reason for family planning sem iurban reason for family planning urban reason for family planning] and the criterion variable (Attitude of people to family planning). In this model they significantly predict the criterion Variable F (15, 14a) 1.947, and jointly account for 17.9% observe variance in people attitude to family planning.Table 4.1. Model Summary
 |
| |
|
Table 4.2. Regression ANOVA
 |
| |
|
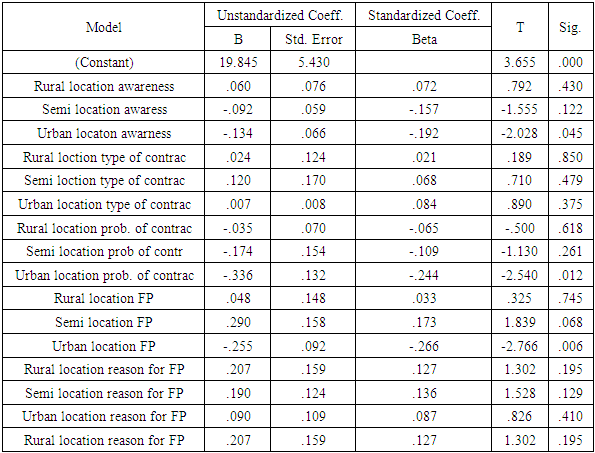
Table 4.3
 |
| |
|
Further result in Table 4.3 shows clearly that four predictor semi awareness (β = -0.157 t (150) = 0.122, p<0.05), semi problem of family planning (β = -0.109, t (150) = 0.195 p<0.05) semi urban reason for family planning (β = 0.136 t (150)= 0.129 p<0.05) have significant effect on this prediction model this mean that each all of them are related variable that do allow significant prediction of attitude of people to family planning. However, rural type of contraceptive use did not contribute significantly to this model. Urban Awareness, urban problem of contraceptive, semi urban location of family planning an urban family planning are the most potent in predicting attitude of people to family planning.Multiple regression analysis was conducted in order to show how environment affect the attitude of people to family planning. The result in table 4.1 an 4.2 show the multiple regression coefficient [R] which indicate that a linear relationship exists, between fifteen predictors [Rural awareness, Semi urban awareness, urban awareness, Rural types of contraceptive use, semi types of contraceptive use, urban type of contraceptive use, rural problem of contraceptive, semi problem of contraceptive, urban problem of contraceptive, rural family planning, semi family planning, urban family planning rural reason for family planning sem iurban reason for family planning urban reason for family planning] and the criterion variable (Attitude of people to family planning). In this model they significantly predict the criterion Variable F (15, 14a) 1.947, and jointly account for 17.9% observe variance in people attitude to family planning.Further result in Table 4.3 shows clearly that four predictor semi awareness ( β = -0.157 t (150) = 0.122, p<0.05), semi problem of family planning (β = -0.109, t (150) = 0.195 p<0.05) semi urban reason for family planning (β = 0.136 t (150) = 0.129 p<0.05) have significant effect on this prediction model this mean that each all of them are related variable that do allow significant prediction of attitude of people to family planning. However, rural type of contraceptive use did not contribute significantly to this model. Urban Awareness, urban problem of contraceptive, semi urban location of family planning an urban family planning are the most potent in predicting attitude of people to family planning.Research question 2: Does status affect attitude of people to family planning.Table 4.4. Model Summary
 |
| |
|
a. Dependent Variable: attitude of peoplePredictors: (Constant), religion, number of children, child status, occupation, marital status, qualification.Table 4.5. Regression ANOVA
 |
| |
|
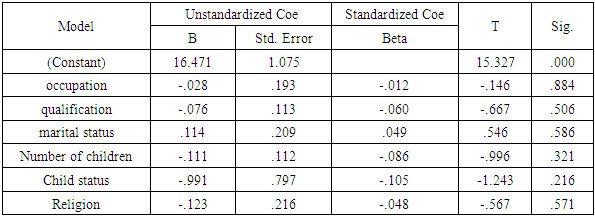
a. Dependent Variable: attitude of peoplePredictors: (Constant), religion, number of children, child status, occupation, marital status, qualification.Table 4.6. Regression Coefficients
 |
| |
|
Multiple regression analysis was also conduct to show show the status affect attitude of people to family planning.Result in table 4.4 an 4.5 review the multiple regression coefficient [R] which indicate the linear relationship exist between the six prediction [religion, number of children, child status, occupation, marital status a qualification] and the caterior variable attitude of people to family planning. In this model they significantly predict the caterion variable F (6,148) = 0.591 and jointly account for 1.57% observed variance in attitude of people the family planning.The table 4.6 further show the result that respond qualification (β -0.060, t (150) = 0.06 p<0.05) marital status of respondent (β = 0.049, t (150) = 0.586 p<0.05), number of children ((β= 0.86, t (150) = 0.321 p<0.05) an religion belief (β= -0.048 t (150) = 0.571 p<0.05) have significant effect in this prediction model. This mean all of them are related variables that do allow significant prediction of attitude of people to family planning. Therefore, occupation of the respondent did not contribute significantly to this particular model. Child status of the respondent is the most potent in predicting attitude of people to family planning.Research Question 3 How does awareness, method use, availability of personnel and clinic affect attitude of people to family planning from the structured interview show in that the health officers disseminate family planning awareness through town hall meeting, market (most especially in the rural area) and media (Radio, Television) for those in semi – urban and urban.The generality of the respondents mentioned injectible contraceptive measure, nor plant method, Voluntary surgical and the best methods depend on individual body system. But the method comes up with side effect such as bleeding, unwanted pregnancy when someone misses daily dosage.Virtually all respondents said family planning clinic are available with qualified personnel in every local government of the state. It is rare for rural people to visit the clinic, semi – urban people fairly visit the clinic, but there is little improvement in the altitude of urban people in visiting family planning clinic. The respondent’s ascertain that everybody was allowed to visit family planning clinic. But most of the time, it is only elite (civil servant), literate market women and literate farmer that often visit the family planning.Nearly all the respondents said family planning materials are not really available in rural area. Few materials are present in semi – urban but a lot of the materials are available in urban area.
4.2. The Graphical Analysis of the Bio Data
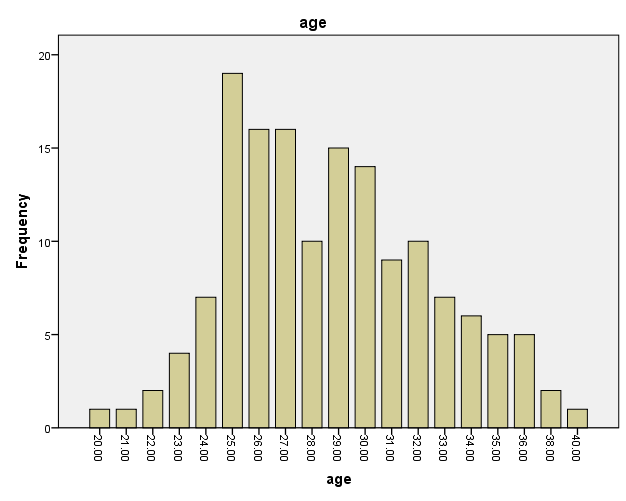 | Figure 1. The table shows frequency distribution of respondent’s age where the highest age is 25 years follows by 26 and 27 years |
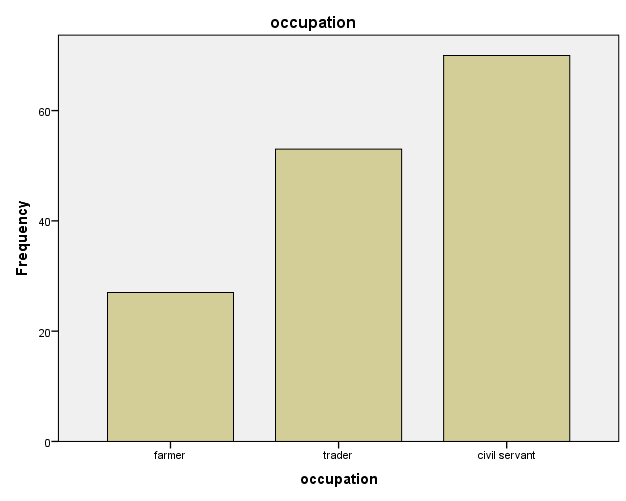 | Figure 2. The graph of frequency distribution of Respondents occupation. The graph revealed that most of the respondents are civil servant (70), trader (53) and the least respondents is farmer (27) |
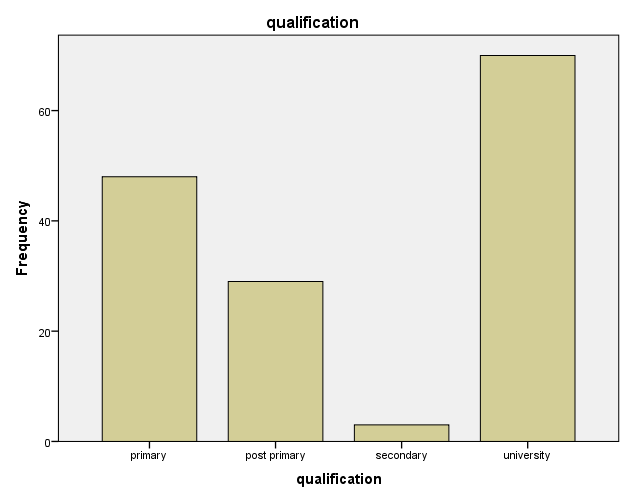 | Figure 3. The graph of frequency distribution of Respondents qualification. The graph shows that most of the respondents are university graduate (70) follow by primary (48), where post primary (29) and the least qualification of the respondents is secondary (3) |
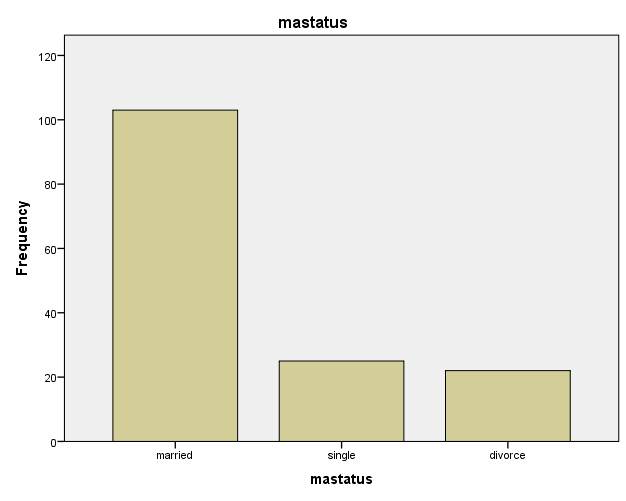 | Figure 4. The graph of frequency distribution of respondent’s marital status. The revealed that most of the respondents are married (103), 25 respondents are single and 22 are divorcee |
5. Summary, Conclusions and Recommendations
This section presents Summary, Conclusion and Recommendation.
5.1. Summary
1. People are aware about family planning through hall meeting, market (in rural) and media (television, radio) in urban. Different family methods are available which have side effect, bleeding, unwanted pregnancy when misses daily dosage.2. Family planning clinic are available in all area with qualified health officer but people rare visit the clinic in rural area, fairly in semi urban but there is improvement in urban area.3. Family planning materials are not available in rural area, few materials are present in semi – urban but lot of materials are in the urban area.4. People in urban area have better attitude to family planning  than those in rural area
than those in rural area  5. Educational level affect people’s attitude to family planning as university graduate have better attitude to family planning
5. Educational level affect people’s attitude to family planning as university graduate have better attitude to family planning  than secondary school graduate
than secondary school graduate  6. Socio – economic level affect people’s attitude to family planning as civil servants have better attitude to family planning
6. Socio – economic level affect people’s attitude to family planning as civil servants have better attitude to family planning  than traders
than traders  7. Religion belief did not affect the attitude of people to family planning. As the mean scores reveal Christianity
7. Religion belief did not affect the attitude of people to family planning. As the mean scores reveal Christianity  Islam
Islam  and traditionalist
and traditionalist  8. Awareness affect people attitude to family planning, urban
8. Awareness affect people attitude to family planning, urban  semi – urban
semi – urban  and rural
and rural  Implications of the finding in this study to various stakeholders are enumerated. The government at all levels should ensure that strong awareness of family planning in all area of the country and provide more family planning clinic equipped with materials and qualified health personnel.People, irrespective of socio economic level, religion, educational level, location should key into family planning by attending regular seminars, workshop, town hall meetings on family planning to enhance their knowledge. This is necessary for them in order to control the number of children they will give birth to.
Implications of the finding in this study to various stakeholders are enumerated. The government at all levels should ensure that strong awareness of family planning in all area of the country and provide more family planning clinic equipped with materials and qualified health personnel.People, irrespective of socio economic level, religion, educational level, location should key into family planning by attending regular seminars, workshop, town hall meetings on family planning to enhance their knowledge. This is necessary for them in order to control the number of children they will give birth to.
5.2. Conclusion
Based on the findings in this study it could be concluded that the attitude of people to family planning is poor. Moreover if government at all levels can intensify efforts on awareness, building of more family planning clinic with qualified health personnel, provision of materials people will have positive attitude towards family planning.
5.3. Recommendation
Based on the findings of this study, the following recommendations are made:1. Health education – there should be an effective health education on the dangers inherent in the misuse of family planning by those who are already using it; now that AIDS and other venereal diseases are rampart. Teaching of sex education should be introduced in schools to enable students learn about family planning early.2. The individuals hawking family planning contraceptives should be discouraged since they don’t have approved clinics and are likely to be administering the contraceptives under unhygienic conditions.3. Government should build more family planning clinics to avoid clients travelling from rural areas to urban areas before obtaining family planning services Harvey (2004). 4. The government should subsidize the cost of the contraceptives or make it duty free so as to make it less expensive to enable more people to take the advantages of family planning services.
6. Questionnaire
This study is designed to assess the attitude of Ekiti community of Ekiti state to family planning.It is an independent academic exercise; the information required will be treated confidently.To ensure anonymity, names are not required.Your candid opinion and cooperation will be highly appreciated.Thank you.Section AInstruction:- please tick the appropriate box.1. Sex: Male ( ) female ( )2. Age: 15 – 25 ( ) (B). 26 – 35 ( ) (C). 46 and above ( ).3. Occupation: (A) Farmer ( ), (B) Trader ( ), (C) Civil servant ( ), (D) House wife ( ), (E) Oth er specify ( ).4. Educational qualification:- (A) Primary Six ( ), (B) Post Primary ( ), (C) Secondary ( ), (D) University ( ), (E) Nil ( ).5. Marital status: (A) Married ( ). (B) single ( ),(C) Divorce ( ), (D) Widow ( ).6. Religion: (A) Christianity ( ), (B) Islam ( ), (C) Traditionalist ( ), (D) other specify ( ).7. Number of pregnancies: (A) 1 - 2 ( ), (B) 2 – 4 ( ), (C) 5 – 6 ( ), (D) 7 and above ( ).8. Number of miscarriages: (A) 1 – 2 ( ), (B) 3 – 4 ( ), (C) 5 – 6 ( ), (D) 7 and above ( ).9. Number of children (A) One ( ), (B) Two ( ), (C) Three ( ), (D) Four ( ), ( ) Five and. above ( ).10. State of children (A) alive ( ), (B) Dead ( ).Section BDisagree - (1), strongly disagree - (2)Agree - (3), strongly Agree – (4)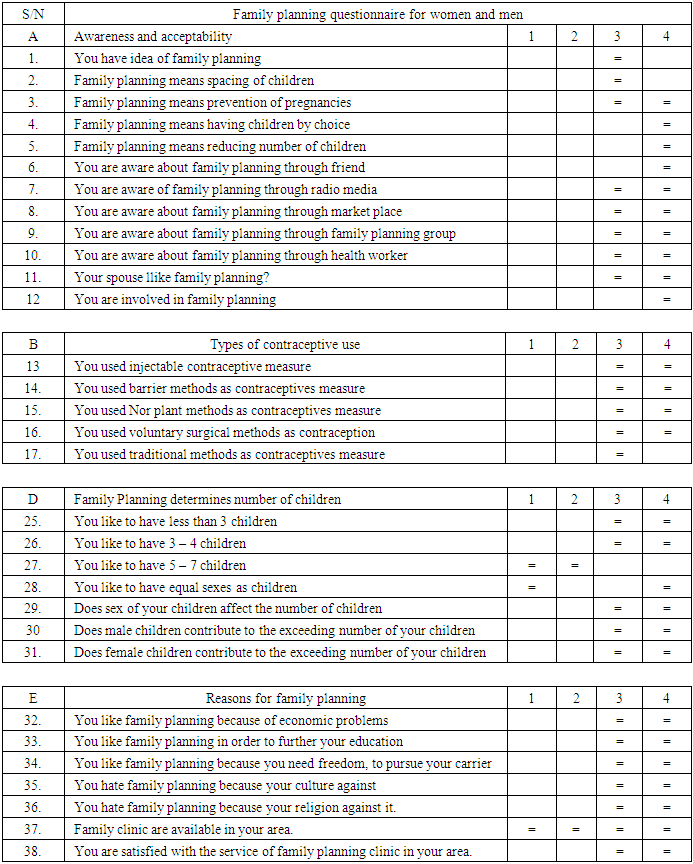
6.1. Interview Schedule for Family Planning Health Officers
Dear RespondentThis formal interview schedule is designed to collect information of……………………………….Kindly supply needed information which will be used for research purposes. This shall be treated with utmost confidentiality. Thank you for your time.Section ASEX: (A) Male ( ), (B) Female ( )Academic Qualification: …………………………Working Experience (A) 1 – 5 years ( ), (B) 6 – 10 years ( ), (C) 11 – 16 years and above ( ).SECTION B Kindly supply appropriate responses as briefly as possible.Question 1: Please explain the concept family planning.Response: Question 2: How does your clinic disseminate family planning awareness?Response:Question 3: What is the different methods/measure can be use in carryout family planning.Response:Question 4: What method / measure are the best?Response:Question 5: Does a family planning method have side effects?Question 6: does family planning clinic available in every local government of the State. (Ekiti State)Response:Question 7: How often people visit family planning clinic?Response:Question 8: Do people show interest in family planning?Response:Question 9: what type of people visit family planning clinic?Response:Question 10: does family planning material available in all FP dispenser outlets?Response:
ACKNOWLEDGEMENTS
I would like to acknowledge the support received from the African-German Network of Excellence in Science (AGNES), the Federal Ministry ofEducation and Research (BMBF)/the Alexander von Humboldt Foundation (AvH) and The World of Academy of Sciences (TWAS) as sponsor(s) in this publication, I am indeed grateful. Thank you very much.
References
| [1] | Z. Hansen 2005. Population growth and Family Planning in India: An analysis. http://www.hsph.harvard.edu/grht/SAasia/suchana/0100/ho45.html. (Retrieved on 5 May 2006). |
| [2] | N. Gupta, A. K. Mathur, M. P. Singh, N. C Saxeena (2004): Reproductive Health awareness of school-going unmarried, rural adolescents. Indian Journal of Pediatrics, 71: 797-801. |
| [3] | S. Bhasin, M. Pant, M. Mehta, S. Kumar (2005): Prevalence of usage of different contraceptive methods in East Delhi – A cross-sectional study. Indian Journal of Community, 30(2): 331-336. |
| [4] | G. Kaur and T. R. Singh (1982): Acceptance of family planning practice among rural women clientele. Indian Journal of Public Health, 26(3): 194-199. |
| [5] | S. Richardson, R. Emma and T. Birn Ann-Emmanuelle (2011): Sexual and reproductive health and rights in Latin America: an analysis of trends, commitments and achievements. Reproductive Health Matters 19(38): 183-196. |
| [6] | S. Ritz, and S. Lindsay. (2013): Access to medicine publication in developing countries: A bibliometric. |
| [7] | L. Harvey (2004): Analytic Quality Glossary, Quality Research International. Available online at: www.qualityresearchinternational.com/glossary/ (accessed on 22 January 2015). |
| [8] | T. J. Chaithanya, B. Vetveja and P. Parveen (2014): Total quality assurance (TQA). International Journal of Management & Social Sciences Research, 3(7), 25-29. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML