-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2026; 16(1): 1-6
doi:10.5923/j.sports.20261601.01
Received: Dec. 31, 2025; Accepted: Jan. 26, 2026; Published: Feb. 26, 2026

The Effects of Eccentric and Concentric Exercise on Joint Position Sense at the Ankle
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSandy Meador1, John W. McChesney2
1Saint Luke’s Center for Orthopedics and Sports Medicine, Boise, Idaho, USA
2School of Kinesiology, Boise State University, Boise, Idaho, USA
Correspondence to: John W. McChesney, School of Kinesiology, Boise State University, Boise, Idaho, USA.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Joint position sense is generally accepted as an important contributing factor to motor performance and is likely an important component to address regarding injury prevention and rehabilitation. Research has shown that light to moderate exercise may improve reproductive joint position sense (RJPS) at the ankle and shoulder whereas exercise leading to fatigue has been shown to reduce threshold joint position sense (TJPS) in the shoulder and RJPS in the knee. The purpose of this study was to examine the effects of eccentric exercise versus concentric exercise of the dorsiflexor muscles on RJPS at the ankle. It was hypothesized that following a fatiguing exercise protocol, absolute error of RJPS at the ankle would be worsened in both the eccentric and concentric groups when compared to control group levels. A second hypothesis asserted that constant error of RJPS would be significantly greater in the exercised subjects than in the control group subjects. Our third hypothesis stated that eccentric exercise to fatigue would cause impairments in ankle RJPS absolute error to an extent significantly greater than that of concentric exercise. The final hypothesis stated that the eccentric exercise group would demonstrate significantly greater constant error of RJPS than the concentric exercise group. Subjects consisted of 30 young adults randomly assigned to either a concentric or eccentric exercise group or a control group. Using a repeated measures design, both experimental groups of subjects were tested for RJPS prior to exercise and after a prolonged bout of exercise. Results demonstrated no significant decrease in RJPS in the experimental groups when compared to the control group. There was no difference found between eccentric and concentric contractions on RJPS at the ankle. There was a significant difference found in RJPS at the ankle when comparing the eccentric group to the control group in the plantarflexion measurement, with the eccentric group demonstrating an improvement. This effect may be due to some warmup benefits of exercise on either the dorsiflexor or plantarflexor muscle group. Neither muscle fatigue nor eccentric exercise was shown to have a negative effect on RJPS at the ankle.
Keywords: Eccentric, Concentric, Reproductive Joint Position Sense, Fatigue, Proprioception
Cite this paper: Sandy Meador, John W. McChesney, The Effects of Eccentric and Concentric Exercise on Joint Position Sense at the Ankle, International Journal of Sports Science, Vol. 16 No. 1, 2026, pp. 1-6. doi: 10.5923/j.sports.20261601.01.
Article Outline
1. Introduction
- Proprioception is well accepted as an important contributing factor to motor performance and is an important component to address regarding injury prevention and rehabilitation. It is essential to have a good sense of body position in athletics, which often requires agility and complex body movements. Not only is proprioception necessary for optimal motor performance, but a decline in proprioception may also influence injury occurrence. Payne and colleagues suggested that proprioceptive deficits were predictive of ankle injuries in collegiate basketball players while other studies have demonstrated the efficacy of proprioceptive training in significantly reducing the incidence of athletic injuries [1,2,3]. There has been very little research done on the role exercise plays in affecting proprioception. This void in the literature and the theory of an exercise effect on proprioception are the compelling factors underlying this study.Current literature reports two divisions of proprioception: kinesthesia and position sense. Kinesthesia describes the sensation of joint movement, while position sense represents the perception of joint position.Somatosensory mechanoreceptors have been identified in the soft tissues around joints, including muscles, tendons, ligaments, joint capsules, and skin. These various sensory receptors combine to provide optimal proprioception [4,5]. It has been reported that cutaneous receptors respond mainly to kinesthesia, with a lesser contribution to joint position. Furthermore, joint capsule and ligament mechanoreceptors have been identified as contributing most significantly at the end ranges of motion, a long standing and robust concept in neuroscience [6].Researchers generally use any of three methods to measure proprioception. These methods are threshold to detection of passive motion (TTDPM), reproductive joint position sense (RJPS), and matching joint position sense (MJPS). TTDPM is explained as a subject’s threshold to detection of passive joint movement. This paradigm involves very slow passive movement of a limb (0.4°/sec) while the subject responds when he/she first detects joint motion. This type of measurement is used to assess kinesthesia [7].RJPS can have a few different variations. It begins with the examiner positioning the limb by moving from the starting position to the target position. This initial target positioning is most commonly done passively by an experimenter. After returning to the starting position, the subject then attempts to reproduce the target position via either active or passive limb motion. Both muscle and joint receptors are stimulated by active positioning while passive positioning isolates joint receptors [8].Considering the conptribution of muscle afferents to proprioception, it seems logical to examine the effects of exercise on joint position sense and kinesthesia. Little research has been done on this topic, but studies suggest that exercise may enhance proprioception [9,10]. It is the premise of this study to examine the effect of exercise on proprioception. While moderate exercise may enhance proprioception, fatiguing exercise has been shown to worsen both kinesthesia and position sense [11,12,13,14]. In order to achieve a level of fatigue, many researchers employ maximal intensity concentric contractions. In addition, fatigue has been shown to decrease proprioception at the knee as well as the shoulder [14]. Because fatigue would be expected to have a greater impact on muscle receptors than joint receptors, the effects of fatigue on position sense lends support to the conclusion that muscle mechanoreceptors provide the primary feedback in joint position sense.Research suggests that eccentric exercise causes damage to muscle fibers, leading to the observable effects of delayed-onset muscle soreness and decreased strength [15,16,17]. It has been suggested that eccentric contractions recruit fewer motor units, leaving more force and tension to be placed on each activated fiber. If eccentric exercise produces muscle damage, it would be expected that eccentric exercise would also damage muscle mechanoreceptors, thereby reducing proprioception. The literature on eccentric exercise and joint position sense is inconclusive. Furthermore, the nature of the relationship between eccentric exercise and joint position sense compared to that of concentric exercise and joint position sense, and whether the current research findings are determined by the type of exercise or by some other variable, such as fatigue, is still unclear.The purpose of this study was to examine the effects of eccentric versus concentric exercise to fatigue of the dorsiflexor muscles on joint position sense at the ankle during dorsiflexion and plantarflexion measurements. This study examined the concept that fatiguing exercise has detrimental effects on joint position sense. It was hypothesized, based on the findings from previous studies [10,14] that following a fatiguing exercise protocol, absolute error of RJPS at the ankle would be worsened in both the eccentric and concentric groups when compared to control group levels. A second hypothesis asserted that constant error of RJPS would be significantly greater in the exercised subjects than in the control group subjects. A third hypothesis stated that eccentric exercise to fatigue would cause impairments in ankle RJPS absolute error to an extent significantly greater than that of concentric exercise. The final hypothesis stated that the eccentric exercise group would demonstrate significantly greater constant error of RJPS than the concentric exercise group.
2. Methods
2.1. Apparatus and Procedures
- Thirty young adults (15 male, 15 female) were recruited to participate in this study. The subjects were recruited by word of mouth and ranged in age from 18-30 years. Participants were randomly assigned to one of three groups: a control group, a concentric exercise group, or an eccentric exercise group. Prior to participation, each subject was informed of the possible risks involved, asked to complete a medical history questionnaire and undergo a pre-participation physical examination of the ankle. Subjects were excluded if they demonstrated significant decrements in muscular strength or neurologic sensation when compared bilaterally, had less than 20° of dorsiflexion and 40° of plantarflexion, or had a current injury to either ankle.Ankle RJPS was measured using an instrumented apparatus with an adjustable, mobile footplate, as described by Walters and McChesney [10]. The experimental foot was situated flat on the footplate to allow full, unresisted range of motion in plantar flexion and dorsiflexion. An electrogoniometer attached to the footplate was aligned with the center of the axis of motion of the talocrural joint, corresponding with a line drawn between the midpoints of the medial and lateral malleoli [18]. A lever attached to one corner of the footplate was positioned to allow the experimenter to passively move the subject’s foot. All subjects wore a blindfold and listened to low-level white noise through headphones to exclude auditory and visual cues during testing. The researcher communicated with the subjects through a microphone attached to the system.Ankle RJPS was assessed in each subject over two experimental sessions. RJPS was tested in the experimental groups prior to exercise and following a fatiguing period of either eccentric or concentric exercise. The control group underwent an RJPS pre-test and a second test following a period of no physical activity. Each subject’s dominant leg was used for all portions of the study. Leg dominance was determined by instructing the subject to step down from a bench and designating the first leg used to step down as the dominant leg.Subjects were placed in a seated position with the dominant bare foot positioned flat on the footplate of the testing apparatus. The experimenter then passively moved the foot through one complete plantarflexion or dorsiflexion range of motion to familiarize the subject with the apparatus and allow the subject to practice relaxing during the passive movement. RJPS testing began with the ankle in a neutral starting position (0°). The foot was then passively moved to a random test angle and the subject was told to memorize the position. The foot was held at that angle for 5 seconds and then passively returned to the starting position. From there, the subject was prompted to actively reproduce the test angle within a ten second period and press a hand-held signal switch when they had reached the desired position. RJPS was tested in both dorsiflexion and plantarflexion. Five trials were performed in each range of motion with absolute error and constant error recorded for each. The error scores for the five trials were averaged to create a mean score to be used in data analysis. Test angles were randomly chosen in the ranges of 5-15° dorsiflexion and 5-30° plantarflexion and varied in order from pre-test to posttest.Subjects were randomly placed into either a concentric or eccentric exercise group or a control group, allowing for 10 individuals in each group. All exercise was done on a modified Orthotron II apparatus which had been converted to an isotonic exercise system using external weights attached to a swing arm for resistance. Following the RJPS pre-test, members of both exercise groups were tested for his/her concentric one repetition maximum (1RM) in ankle dorsiflexion. Two minutes were allowed between each 1 RM trial for recovery. To facilitate testing, each subject was placed in a seated position with the experimental leg extended and a small bolster under the knee. The subject’s foot was secured onto a footplate that allowed unrestricted motion in dorsiflexion and plantarflexion.To familiarize each subject with the exercise apparatus and protocol, the experimenter began by passively moving the secured foot through a complete range of motion. The subjects were then instructed on the exercise protocol. Subjects were seated in the same position as for the 1 RM testing. The starting foot position for the concentric exercise group was with the foot in full plantarflexion. The subject was then instructed to dorsiflex the foot as far as possible. Next, the experimenter verbally instructed the subject to relax and passively moved the foot back to the starting position. A movement from starting position to starting position was considered one repetition. Three sets of repetitions to fatigue were performed moving through dorsiflexion at 80% 1RM until they were unable to actively move their ankle back to ankle neutral (the point of fatigue) while under weight. Subjects were given a 30-second rest period between each set. Following completion of the exercise protocol, the subject was instructed to immediately remove his/her shoe and be transferred to the RJPS apparatus for the second session of position sense testing. The transfer to the RJPS apparatus required that the subject simply pivot 90 degrees while remaining seated. The average time elapsed from completion of the concentric exercise to the beginning of the posttest was 43 seconds.Subjects in the eccentric exercise group performed a similar protocol, but they began with the foot statically held in full dorsiflexion (~20°) while weighted. Subjects were then instructed to actively lower the foot through the complete plantarflexion range of motion over a three-second period. A mechanical stop was provided at 50° of plantarflexion in order to avoid the risk of being stressed past the normal end range of motion. At the end of the plantarflexion range, the weight was released and the examiner again instructed the subject to passively moved the foot back to the starting position to complete one repetition. This group performed three sets to fatigue at 120% of the 1RM weight with 30-second rest periods between each set. This ECC exercise weight percentage of the 1RM was determined from data that shows a muscle can produce 40 percent more tension eccentrically than it does concentrically [19]. Fatigue was determined as the point at which the subject could no longer actively hold the weight in the static starting position prior to commencing to lower the weight back through the plantarflexion range. Following completion of the exercise protocol, the subject immediately removed his/her shoe and was transferred to the RJPS apparatus for the second trial of position sense testing. The transfer occurred in the same method as the concentric group. The average time elapsed from completion of the eccentric exercise protocol to the beginning of the posttest was 44 seconds. The control group subjects read for ten minutes between RJPS trials.
2.2. Data Analysis
- Mean absolute error (AE) and mean constant error (CE) were measured in degrees to an accuracy of 0.10° and analyzed to assess RJPS at the ankle. Absolute error is defined as the number of degrees the actively reproduced position differs from the reference position. Constant error involves the direction of difference and is defined as the number of positive or negative degrees the actively reproduced position is from the reference position.This study involved a pre-test, post-test, control group design. The independent variables consisted of eccentric and concentric fatiguing exercise and no exercise. The dependent variable was ankle RJPS measured in degrees. AE and CE scores were calculated, and differences were compared to assess the effects of fatiguing exercise on RJPS. Differences between groups were calculated and compared to assessing differing effects between concentric and eccentric exercise. RJPS scores were compared using independent t-tests as well as a repeated measures analysis of variance (ANOVA) with statistical significance at the 0.05 level.
3. Results
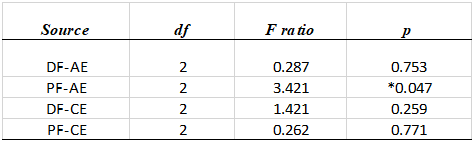
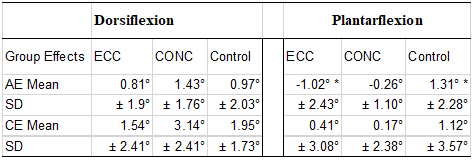
- Independent t-tests were used to analyze group difference scores in both absolute error (AE) and constant error (CE). This analysis revealed no significant differences of AE in dorsiflexion between the control and concentric groups, the control and eccentric groups, and the eccentric and concentric groups. The repeated measures ANOVA was used to compare RJPS mean error score differences between each of the three groups. The ANOVA revealed a significant difference in AE in plantarflexion in the ECC (M= -1.02° ± 2.43°) versus control (M= 1.31° ± 2.28°) at 95% confidence Interval (CI) group analysis (p=0.04) with a raw effect size nearing 0.3°. No differences were found between the CONC and control or the ECC and CONC scores in plantarflexion (Figure 1). (Table 1).
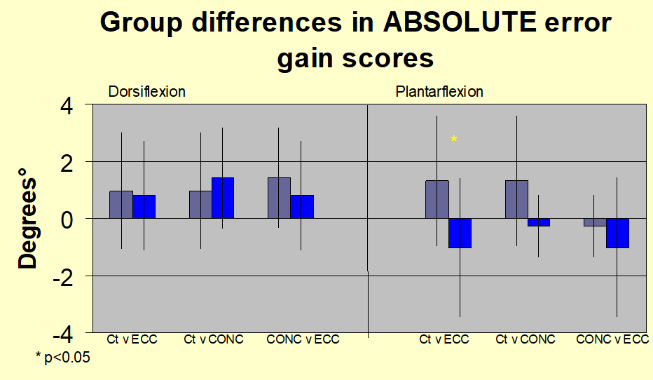 | Figure 1. Group comparison of absolute error gain scores across the three groups of Control (Ct), Eccentric (ECC) & Concentric (CONC) in both the ankle dorsi and plantarflexion ranges at a confidence interval (CI) of 95% |
|
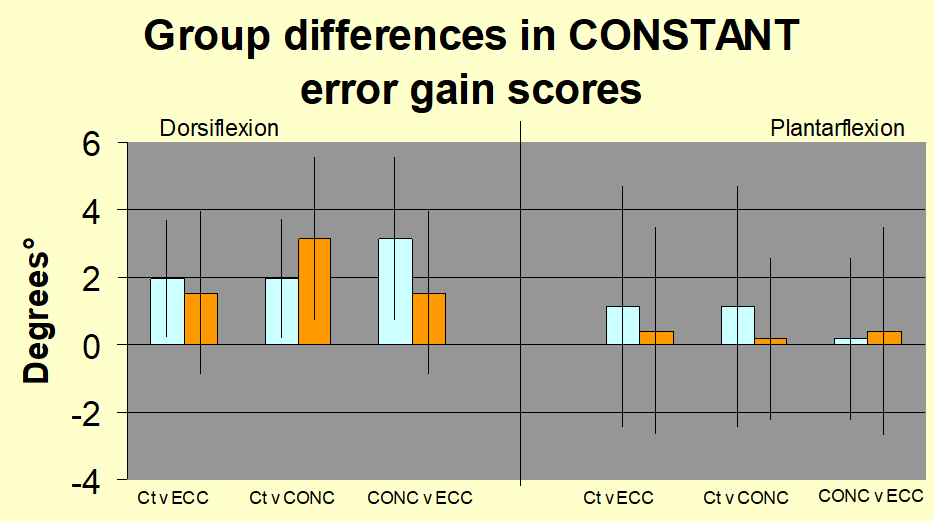 | Figure 2. Group comparison of constant error gain scores across the three groups of Control (Ct), Eccentric (ECC) & Concentric (CONC) in both the ankle dorsi and plantarflexion ranges. No significant difference was observed at the CI of 95% |
4. Discussion
- The purpose of this study was to examine whether ankle reproduction joint position sense (RJPS) would be affected by fatiguing exercise involving concentric or eccentric contractions of the dorsiflexor muscles. By analysing the results, we hope to increase the understanding of the effects exercise and muscle fatigue have on proprioception.Gain scores were analysed between each exercise group and the control group to determine the effects of muscle fatigue on RJPS. Because it is generally agreed in recent literature that muscle mechanoreceptors play a primary role in joint position sense, especially in the mid-ranges of motion [4,20]. It was hypothesized that muscle fatigue would worsen the ability of the subjects to reproduce a target angle. These results fail to support this hypothesis. The only significant effect was found in the eccentric exercise group versus the control group comparison in plantarflexion. Instead of a worsened RJPS, the treatment group demonstrated an improvement. The findings of this study do not demonstrate any worsening of joint position sense due to fatigue.We observed an improvement of AE of RJPS following fatigue in the ECC group when measured in plantarflexion. While moderate exercise has been shown to enhance proprioception [9,10], no previous study has demonstrated an improvement following muscle fatigue. This occurrence is most likely due to the fact that only the dorsiflexor muscles were fatigued. The improvement following exercise was noted in the plantarflexion motion, which would initiate a stretch of the dorsiflexor muscles, but actively used the gastrocnemius-soleus complex. Each of the previous studies measured active contractions of the fatigued muscle(s) only. This reasoning may not necessarily explain why the ECC group demonstrated a significant improvement in RJPS from pre-exercise to post exercise levels in plantarflexion. We can only hypothesize about reasons behind the observed improvement in RJPS. One possible reason could be that eccentric exercise of the dorsiflexor muscles served as a warm-up which then enhanced RJPS when those muscles were placed on a passive stretch. Another possible reason could be that the plantarflexor (antagonist) muscles may have undergone some contractions during the eccentric exercise. This activity may have resulted in the same benefits to RJPS seen following moderate exercise.Constant error score differences were also analysed to determine the direction of error. A positive constant error translates to a tendency to overshoot the target while a negative constant error is interpreted as a tendency to undershoot the target angle, both of which appear not to be affected by exercise. Research suggests that eccentric muscle contractions lead to damage of muscle fibers, creating muscle soreness and decreases in strength and range of motion [15,16,17]. It is not known if this muscle damage would influence the muscle mechanoreceptors that are fundamental to proprioception. If so, one would expect to see an impairment in RJPS following prolonged eccentric exercise. Group differences in error scores from pre-exercise testing to post exercise testing of the ECC group and the CONC group were compared in order to determine if eccentric contractions were more harmful to proprioception than concentric contractions. Data analysis revealed no significant difference between the two exercise types. Eccentric exercise also had no effect on the direction of error.This lack of an observed effect supports previous studies in which it was demonstrated that eccentric exercise of the elbow flexors had no effect on RJPS at the elbow joint [15,18]. Eccentric exercise may create mechanical changes in muscle tissue, but evidence does not support the concept that eccentric exercise differs from concentric exercise in its effects on proprioception.
5. Conclusions
- One purpose of this study was to determine the effects of muscle fatigue on RJPS at the ankle. This study did not demonstrate any negative effect on RJPS at the ankle due to muscle fatigue. The hypotheses, H1 and H2, which stated fatiguing exercise would increase AE and CE scores of RJPS were not supported by the data.These results both support and contradict previous studies on the effects of fatigue on proprioception [9,12,13,14]. It is a robust concept that muscle mechanoreceptors play a vital role in proprioception, but the degree to which fatigue influences these proprioceptive receptors is still in question and further investigation is needed.The second purpose of this study was to determine if eccentric exercise produced effects different from those following concentric exercise. There was no difference found either in amount or direction of error. The data failed to support H3 and H4, which stated that AE and CE scores of RJPS would increase by a greater degree following eccentric exercise than following concentric exercise. This study examined only the immediate effects of eccentric exercise on RJPS. However, eccentric exercise has been known to produce lingering effects to muscle for several days following the actual exercise. More research is warranted as to the consequences of these lingering effects on proprioception at all joints of the body.
References
| [1] | Payne KA, Berg K, Latin RW. Ankle injuries and ankle strength, flexibility, and proprioception in college basketball players. JAthlTrain. 1997; 32: 221-225. https://pubmed.ncbi.nlm.nih.gov/16558453/. |
| [2] | Rivera MJ, Winkelmann ZK, Powden CJ, Games KE. Proprioceptive Training for the Prevention of Ankle Sprains: An Evidence-Based Review.JAthlTrain. 2017; 52(11): 1065-1067. doi: 10.4085/1062-6050-52.11.16. |
| [3] | Schiftan GS, Ross LA, Hahne AJ. The effectiveness of proprioceptive training in preventing ankle sprains in sporting populations: a systematic review and meta-analysis. J SciMed Sport. 2015; 18(3): 238-244. doi: 10.1016/j.jsams.2014.04.00. |
| [4] | Salamanna F, Caravelli S, Marchese L, et al. Proprioception and Mechanoreceptors in Osteoarthritis: A Systematic Literature Review. J Clin Med. 2023; 12(20): 6623. Published 2023 Oct 19. doi: 10.3390/jcm12206623. |
| [5] | Purves D, Augustine GJ, Fitzpatrick D, et al., editors. Neuroscience. 2nd edition. Sunderland (MA): Sinauer Associates; 2001. Mechanoreceptors Specialized for Proprioception. Available-from: https://www.ncbi.nlm.nih.gov/books/NBK10812/. |
| [6] | Proske U. A reassessment of the role of joint receptors in human position sense. Exp Brain Res. 2023; 241(4): 943-949. doi: 10.1007/s00221-023-06582-0. |
| [7] | Strong A, Arumugam A, Tengman E, Röijezon U, Häger CK. Properties of tests for knee joint threshold to detect passive motion following anterior cruciate ligament injury: a systematic review and meta-analysis. J Orthop Surg Res. 2022; 17(1): 134. Published 2022 Mar 4. doi: 10.1186/s13018-022-03033-4. |
| [8] | Gonzales Tomas I. , Goble Daniel J. Short-Term Adaptation of Joint Position Sense Occurs during and after Sustained Vibration of Antagonistic Muscle Pairs. 2014 Frontiers in Human Neuroscience 2014 (8) https://www.frontiersin.org/journals/human-neuroscience/articles/10.3389/fnhum.2014.00896. DOI 10.3389/fnhum.2014.00896. |
| [9] | Yılmaz O, Soylu Y, Erkmen N, Kaplan T, Batalik L. Effects of proprioceptive training on sports performance: a systematic review. BMC Sports Sci Med Rehabil. 2024; 16(1): 149. Published 2024 Jul 4. doi: 10.1186/s13102-024-00936-z. |
| [10] | Walters AC, McChesney J. An Analysis of the Effects of Ankle Taping on Proprioception: A Comparison Before and After Exercise. Copyright Boise State University Thesis; 2002. |
| [11] | Roditi EE, Tsatalas T, Sakkas GK, Koutedakis Y, Giakas G, Karatzaferi C. Effects of Muscular Fatigue on Position Sense in Two Phases of the Menstrual Cycle. J Funct Morphol Kinesiol. 2024; 9(3): 115. Published 2024 Jun 29. doi: 10.3390/jfmk9030115. |
| [12] | Hadjisavvas, S., Efstathiou, M.A., Themistocleous, IC. et al. Effect of eccentric exercise-induced fatigue on proprioception, motor control and performance of the upper limb in handball players. Sport Sci Health 21, 1821–1835 (2025). https://doi.org/10.1007/s11332-025-01404-y. |
| [13] | Allen TJ, Leung M, Proske U. The effect of fatigue from exercise on human limb position sense. J Physiol. 2010; 588 (Pt 8): 1369-1377. doi: 10.1113/jphysiol.2010.187732. |
| [14] | Chen Z, Zhao T, Shen Y, Ren S, Sun L. The effects of muscle fatigue on shoulder proprioception and forehand stroke accuracy in Chinese elite table tennis athletes. BMC Sports Sci Med Rehabil. 2025; 17(1): 199. Published 2025 Jul 12. doi: 10.1186/s13102-025-01204-4. |
| [15] | Proske U, Morgan DL. Muscle damage from eccentric exercise: mechanism, mechanical signs, adaptation and clinical applications. J Physiol. 2001; 537 (Pt.2): 333-345. doi: 10.1111/j.1469-7793.2001.00333.x. |
| [16] | Vila-Chã C, Hassanlouei H, Farina D, Falla D. Eccentric exercise and delayed onset muscle soreness of the quadriceps induce adjustments in agonist-antagonist activity, which are dependent on the motor task. Exp Brain Res. 2012; 216(3): 385-395. doi: 10.1007/s00221-011-2942-2. |
| [17] | Konrad A, Kasahara K, Yoshida R, Yahata K, Sato S, Murakami Y, Aizawa K, Nakamura M. Relationship between Eccentric-Exercise-Induced Loss in Muscle Function to Muscle Soreness and Tissue Hardness. Healthcare. 2022; 10(1): 96. https://doi.org/10.3390/healthcare10010096. |
| [18] | Walsh LD, Hesse CW, Morgan DL, Proske U. Human forearm position sense after fatigue of elbow flexor muscles. J Physiol. 2004; 558(Pt 2): 705-715. doi: 10.1113/jphysiol.2004.062703. |
| [19] | Nuzzo JL, Pinto MD, Nosaka K, Steele J. The Eccentric: Concentric Strength Ratio of Human Skeletal Muscle In Vivo: Meta-analysis of the Influences of Sex, Age, Joint Action, and Velocity. Sports Med. 2023; 53(6): 1125-1136. doi: 10.1007/s40279-023-01851-y. |
| [20] | Vaughan G Macefield, The roles of mechanoreceptors in muscle and skin in human proprioception, Current Opinion in Physiology, Volume 21, 2021, Pages 48-56, ISSN 2468-8673, doi.10.1016/j.cophys.2021.03.003. |