-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2024; 14(1): 1-4
doi:10.5923/j.sports.20241401.01
Received: Dec. 30, 2023; Accepted: Jan. 24, 2024; Published: Feb. 5, 2024

The Effects of Kinesio Tex TapeTM Application on Maximal Grip Strength and Rate of Fatigue in Healthy Adults
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJohn W. McChesney1, David Hammons1, Jon Hart2
1Department of Kinesiology, Boise State University, Boise, Idaho, USA
2Jon Hart, Santiam County School District, Mill City, Oregon, USA
Correspondence to: John W. McChesney, Department of Kinesiology, Boise State University, Boise, Idaho, USA.
| Email: |  |
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Muscle fatigue has been proven to be a risk factor for injury. Many athletic training techniques have tried to address this factor. One relatively new technique is the application of Kinesio TapeTM. Previous research suggests that Kinesio TapeTM decreases rate of fatigue in the quadriceps, hamstring and lumbar extensors, however rate of fatigue has not been evaluated in the wrist and hand flexors. The purpose of this study was to determine the effect of Kinesio Tex TapeTM application on isometric grip strength rate of fatigue in healthy adults. A total of 41 healthy subjects were recruited for testing from two North American universities. After a warm-up, isometric grip strength and the rate of fatigue was measured in their dominant (D) and non-dominant (ND) hands using the ForceMapTM system under three conditions. Results showed that there was no significant difference between the control, placebo or Kinesio TapeTM conditions in either hand for rate of fatigue as measured by slope (D: p=0.191, ND: p=0.739) and that there was no significant difference in strength (maximal grip force) between the conditions (D: p=0.985, ND: p=0.974). Results of this study do not concur with previous studies suggesting that Kinesio TapeTM can decrease the rate of fatigue in other muscle groups.
Keywords: Kinesio TapeTM, Grip ForceMapTM, Maximal Grip Strength, Slope, Fatigue
Cite this paper: John W. McChesney, David Hammons, Jon Hart, The Effects of Kinesio Tex TapeTM Application on Maximal Grip Strength and Rate of Fatigue in Healthy Adults, International Journal of Sports Science, Vol. 14 No. 1, 2024, pp. 1-4. doi: 10.5923/j.sports.20241401.01.
Article Outline
1. Introduction
- The use of Kinesio TapeTM (KT) has become very popular in athletics and rehabilitative medicine. KT is a special therapeutic tape and taping method created in 1973 by the Japanese chiropractor Kenzo Kase [1]. Kinesio TapeTM, as well as Kinesio Tex Tape (KTT) is made of elastic cotton fiber and acrylic adhesive in a wavy pattern that is designed to replicate the human finger print. The distinctive design of KTT allows for a longitudinal stretch of up to 40–60% of its original length and evaporation of body moisture. Unlike other types of medically rated tape, such as non-elastic and other elastic tapes, KTT is designed to be lite on the skin, allow full range of motion and, be less restrictive.According to Kase, the KT method can be applied to increase proprioception, reduce pain and edema, decrease muscle spasms, and assist weak muscles [2]. Even with its prevalent use, evidence supporting the purported effects of KT remains limited [3,4,5]. It is the opinion of these researchers that further investigation is warranted regarding KT. Specifically investigating KT’s effect on its ability to assist weak muscles through an assessment of maximal grip strength and rate of fatigue is of interest and forms the basis of this study.In this study, we have chosen to use a novel device for measuring hand strength known as the MMD ForceMapTM (MMD Incorporated, Boise, ID, USA). This grip analyser uses tactile array technology to measure grip strength [6]. Since the ForceMapTM uses a cylindrical transducer it is believed that it may be more generalizable to daily activities such as any tool that has a cylindrical handle, turning doorknobs, grasping cans of food, and/or grasping a steering wheel [7].The purpose of this study is to evaluate the effects of Kinesio Taping on 1) maximal isometric grip strength measured by highest force generated during a maximal voluntary isometric contraction (MVIC) and 2) grip strength rate of fatigue as measured by the slope of the linear least squares regression line. It is Hypothesized that: H1) Grip strength will be increased with the Kinesio Tape condition vs placebo or control. H2) Rate of fatigue will be decreased with Kinesio Tape application vs the placebo or control.
2. Methods
- Fifty-nine healthy subjects were recruited via word of mouth from two North American universities. After initial screening, 18 males and 23 females between the ages of 18 and 30 years participated in the study. Exclusions included any subject with any hand, wrist, forearm, elbow or finger dysfunction in the last year, endocrinological conditions, or a history of smoking. Participants were required to complete a pre-participation health history questionnaire. Part of this questionnaire included demographic information and anthropometric measurements. All subjects underwent and agreed to informed consent form.
2.1. Instrumentation and Procedures
- Isometric grip strength was measured through the data analysis window of the ForceMapTM system (Figure 1) [8].
 | Figure 1. The ForceMapTM grip analysis system data window showing digital pressures (PSI) over time |
 | Figure 2. Kinesio TexTM Tape Facilitation application |
2.2. Data Analysis
- Maximal isometric grip force in pounds and rate of fatigue via regression line slope data were collected during each trial. Maximal Grip force was calculated using the exported data from the ForceMap™ system for each trial of each condition. All calculations were developed using Microsoft Excel. These ranged in value from 49 pounds to 254 pounds. The rate of fatigue data was calculated using the force-time curve of each trial. A linear least squares regression line was created from the data points from maximal force through five seconds post maximal force. The slope of this line was then used to assess fatigue. Values ranged anywhere from -0.41 to -8.6. Data was collected at a rate of seven hertz. Means were calculated between experimental, placebo and control trials and compared for statistical significance using a repeated measure analysis of variance (ANOVA).
3. Results
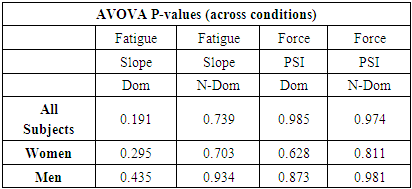
- All data was evaluated in search of significant differences between groups. When the data was compared using a repeated measures ANOVA, results showed there was no significant difference between the control, placebo or Kinesio TapeTM conditions for rate of fatigue (slope) in all subjects (grouped) as well as within genders. There were also no significant differences observed in maximal grip force strength between the groups in all conditions (Table 1.)
|
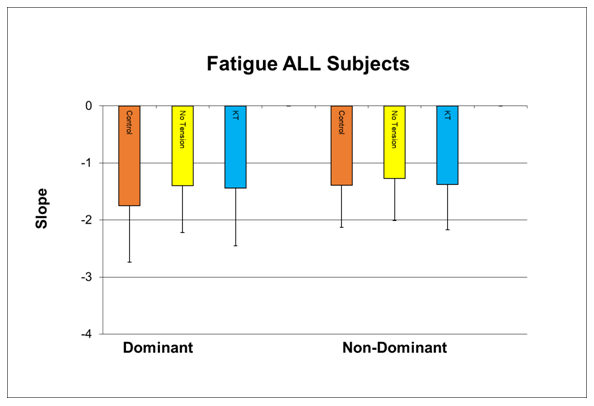 | Figure 3. Fatigue as measured by slope across all subjects and conditions of control, no tension (placebo) and KT (Kinesio TapeTM) |
|

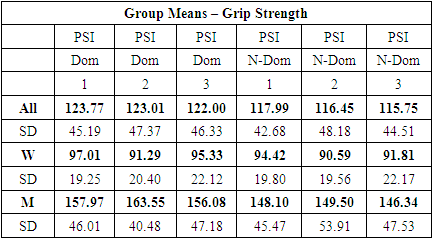
 | Figure 4. Grip strength in all three conditions measured in pounds per square inch and conditions of control, no tension (placebo) and KT (Kinesio TapeTM) |
|
4. Discussion
- Employing the use of Kinesio TapeTM for purposes of facilitating motor performance during athletics and rehabilitation is commonplace. Our results were not supportive of the original hypotheses for either improvement of grip strength or rate of fatigue during an MVIC. In this study, we replicated the recommendations of Kase of applying a pre-stretch to the KT tape by a certified practitioner [1]. Our findings showed that both the control and placebo groups did not differ from the experimental KT group. This lack of an observed treatment effect suggests that pre-stretching the FT tape may not be necessary, as it appears to not have an effect. Alternatively, there may be a need to apply additional pre-stretch to increase the amount of recoil that the tape imparts on cutaneous sensation and the underlying tissues of the forearm. Our results demonstrate that applying the 20% pre-stretch likely does not impact MVIC or rate of fatigue. While this study investigated the use of clinical Kinesio Tape ™ in a healthy population, these findings may be less applicable to a pathologic population. The lack of any changes to grip strength nor the rate of fatigue is clinically significant as grip strength is an important neuro-motor behavior critical to the activities of daily living. Our observations concur with other studies on healthy subjects where no changes were noted between a control group (no tape) and an experimental taped group. However, in the clinical setting, any observed positive effect from the application of KT tape in patients could be due to the effect of a cutaneous tactile response such that the use of KT tape may be justified in this population [11].This study employed an MVIC of 15 seconds to improve the sincerity of effort in comparison to a longer effort, as previously described. Where previous studies have demonstrated that a 30 second effort results in a decrease in the MVIC grip effort, decreasing the MVIC effort time did not impact the rate of fatigue between any of the conditions in this study. On final analysis, the MVIC may not replicate all activities of daily living that require gripping motions and the findings of this study may translate to a limited number of functional activities, at best. Further investigation into the efficacy of tape application to the skin for purposes of increasing motor performance, is warranted.
5. Conclusions
- Kinesio Tape has served as an adjunct to athletic performance and rehabilitative medicine for many years. While the underlying mechanisms of any observed benefit of KT are still under investigation, the contributions of which to its users has been significant and it still grows in popularity. With regard to a benefit to grip strength, this study has shed light on fact that there may not be a positive effect by KT on the metrics evaluated in this study. Without a doubt, more experimentation is needed to discover any effect of KT on motor performance and/or the rehabilitation process.