-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2023; 13(1): 8-13
doi:10.5923/j.sports.20231301.02
Received: Jan. 27, 2023; Accepted: Feb. 10, 2023; Published: Feb. 28, 2023

Energy Expenditure and Relative Intensity of a High-Intensity Functional Training Regimen in Postmenopausal Females with Obesity
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLTrent Yamamoto1, Phillip Goldman1, 2, Bilal Pandit1, Mitchell S. Mologne1, Corinne McCabe1, David Gomez1, Brett A. Dolezal1
1Airway & UCFit Digital Health-Exercise Physiology Research Laboratory, David Geffen School of Medicine, University of California Los Angeles, CA, USA
2Baylor College of Medicine, Houston, Texas, TX, USA
Correspondence to: Trent Yamamoto, Airway & UCFit Digital Health-Exercise Physiology Research Laboratory, David Geffen School of Medicine, University of California Los Angeles, CA, USA.
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The potential of high-intensity functional training (HIFT) has yet to be realized in the treatment of obesity and weight-loss exercise programs, specifically within postmenopausal females with obesity. Twelve postmenopausal obese females (BMI 33.0 ± 1.9 kg/m2, 63.3 ± 4.8 years) participated in a 35-minute group-based HIFT session while donning a portable breath-by-breath gas analyzer and heart rate monitor to measure energy expenditure and exercise intensity, respectfully. The HIFT session elicited the following measurement results: Mean ± SD caloric expenditure of 509 ± 79 kcal, maximum heart rate of 173 ± 5 bpm and %HRmax of 93%, and metabolic equivalents (METS) of 12.1 ± 1.4 kcal/kg/hr. All participants reported that the HIFT session was “enjoyable” yet “challenging”. Implementing this high exercise intensity and energy expenditure session twice weekly would comport with Physical Activity Guidelines for Americans weekly vigorous-intensity physical activity recommendations.
Keywords: High Intensity Functional Training, HIFT, Postmenopausal, Obesity, Exercise intensity
Cite this paper: Trent Yamamoto, Phillip Goldman, Bilal Pandit, Mitchell S. Mologne, Corinne McCabe, David Gomez, Brett A. Dolezal, Energy Expenditure and Relative Intensity of a High-Intensity Functional Training Regimen in Postmenopausal Females with Obesity, International Journal of Sports Science, Vol. 13 No. 1, 2023, pp. 8-13. doi: 10.5923/j.sports.20231301.02.
Article Outline
1. Introduction
- Obesity remains at the forefront of a myriad of public health issues, as the prevalence of obesity has continued to increase at an alarming rate in the United States [35]. The complications associated with obesity, such as comorbid type II diabetes, coronary artery disease, and other cardiovascular issues [21], demonstrate a strong correlation with significantly lower life expectancy as well as quality of life [25]. Women, in particular, have a disproportionate predisposition to develop obesity in comparison to men, especially those in postmenopausal years [16]. This increased likelihood can be attributed to a combination of factors such as hormonal changes, increased adiposity, and decreased energy expenditure [3]. Common interventions used in the treatment and prevention of obesity include behavioral counseling and pharmacotherapy, which have been shown to yield low-to-moderate health benefits [33]. Primary care providers also prescribe modest aerobic exercise in the form of walking. However, research suggests that due to their relatively low VO2max, obese women tend to have a greater level of perceived exertion when walking, thus making it difficult for patients to adhere to this form of exercise [17]. Moreover, brisk walking on its own may be less effective than hypocaloric diets in producing energy deficits required for weight loss [34]. In order to address the ineffectiveness of these standard exercise recommendations for this sub-clinical and clinical population, alternative exercise strategies must be considered. With many interventions for obesity being focused on a case-by-case basis, very few are targeted across group and/or community levels. Recent research has examined the influence of social networks on obesity but has inadequately addressed how to incorporate social components into the treatment of obesity itself [15]. One viable solution is through the use of high-intensity functional training (HIFT). HIFT is a method of training that is often referred to as a CrossFit derivative that employs the use of multimodal, functional resistance exercise weaved in with cardiovascular exercises to improve fitness and performance [8]. Given that HIFT is generally conducted in a group setting, participants often report an increased sense of community, enjoyment, and motivation in the presence of others [28]. Additionally, the physical benefits of HIFT include increased endurance, muscular strength, and lean body mass [14,4]. Similarly structured forms of exercise, such as high-intensity interval training, have produced reductions in visceral adipose tissue and inflammatory markers in obese postmenopausal women [22]. While these results are promising, a paucity of research is available with HIFT and postmenopausal obese females. The purpose of this study is to objectively measure and characterize energy expenditure and intensity of a group based HIFT class offered at a popular commercial fitness boutique within postmenopausal obese females. In doing so, this may determine the feasibility of implementing HIFT as an adjunct prescription for treating obesity and obesity-related diseases in this under representative cohort. We hypothesize that the unique structure and components of this HIFT session will allow it to meet the national exercise guidelines for weekly vigorous-intensity activities, as outlined by the Physical Activity Guidelines for Americans.
2. Methods
- ParticipantsA cohort of twelve postmenopausal female adults (63.3 ± 4.8 years) that met the World Health Organization definition of obesity (body mass index (BMI): 33.0 ± 1.9 kg/m2,) and with memberships at a local fitness boutique (Basecamp Fitness®, Basecamp Fitness LLC, Woodbury, MN) were recruited via word-of-mouth. Exclusion criteria screened out potential participants that had cardiovascular, musculoskeletal, pulmonary, or other disorders that would prevent participation in high-intensity exercise. Written informed consent was obtained from every participant at the beginning of the study. This research was approved by the UCLA Institutional Review Board and carried out fully in accordance with the ethical standards of the Helsinki Declaration. Protocol This was a scoping descriptive study using postmenopausal obese females with different levels of HIFT exercise experience. Height and weight were measured at the facility with a Physician’s Beam scale (Detecto, Webb City, MO) and the history of participation in HIFT classes was acquired through computer records. Participants were instructed to adhere to their typical diet and refrain from strenuous exercise for at least 24 hours prior to testing. All participants completed one session of a signature group based HIFT class at a Los Angeles location. A group instructor facilitated the 35-minute class, which consisted of thirty 1-minute rounds of exercise with 10-second rest intervals and a transition in between. Exercise rounds rotated between 15 functional upper and lower body resistive exercises and 15 seconds on an Assault Airbike® (Assault Fitness, Carlsbad, CA) (averaging 55-65 rpm interspersed with 10-sec sprints halfway through). The resistive exercises were completed with TRX Suspension Training® equipment (Fitness Anywhere LLC, San Francisco, CA), barbells, dumbbells, kettlebells, and the participant’s body weight (Figure 1). Participants chose their starting weights, and the group instructor prompted them to progressively increase their weights after each exercise.
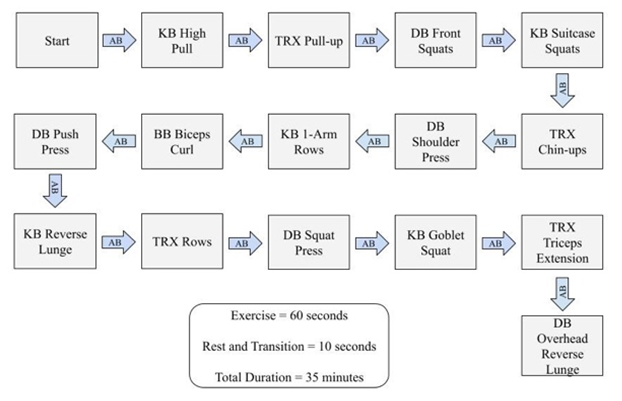 | Figure 1. Example of a signature group based HIFT class (5). AB = Assault Bike; KB = Kettle Bell; TRX = Total Resistance Exercise Suspension Trainer; DB = Dumbbell; BB = Barbell |
3. Results
- All twelve participants successfully completed the HIFT session. The cohort mean ± SD was age = 63.3 ± 4.8 years, weight = 92.8 ± 1.9 kg, height = 167.6 ± 5.2 cm, and body mass index (BMI) = 33.0 ± 1.9 kg/m2. Prior HIFT history averaged 12 sessions with a range of 2 to 35 performed in the past 12 months. The HIFT session elicited the following measurement results: Mean ± SD caloric expenditure of 509 ± 79 kcal, maximum heart rate of 173 ± 5 bpm and %HRmax of 93%, and metabolic equivalents (METS) of 12.1 ± 1.4 kcal/kg/hr.Per participant interviews, all reportedly “enjoyed” the HIFT, felt it was “challenging” yet not prohibitive as an exercise modality and would include it as part of their comprehensive weight-loss program.
4. Discussion
- High intensity exercise regimens similar to HIFT have conferred significant health benefits, including improvements in cardiovascular fitness and reductions in body fat located in the trunk and lower extremities in a number of longitudinal research studies [31,32]. The present study is among the first to determine objective measures of energy expenditure and exercise intensity from a single bout of HIFT in postmenopausal females with obesity.Postmenopausal females typically struggle with exercise for several reasons. Recent research has found age to be a significant determining factor in the efficacy of exercise, as older participants tend to be less trainable and less responsive to exercise [11]. Furthermore, Aiello et al. examined the effects of a yearlong, moderate-intensity exercise program on postmenopausal women that had not received hormone therapy for at least six months [1]. Exercise was found not only to have a negligible effect on reducing menopausal symptoms, but may have even exacerbated others, such as hot flashes [1]. In consideration of compliance, postmenopausal females report higher perceived exertion during cardiovascular exercise, which makes adhering to consistent exercise especially difficult [17]. To that end, there is a significant amount of variability in VO2max responses for postmenopausal females that do adhere to traditional cardiovascular exercise [29]. However, alternative training modalities of high-intensity aerobic and resistance exercise similar to HIFT have been shown to confer improvements in VO2max [4]. Coupled with the benefits of higher self-esteem and intrinsic motivation in women associated with group-based exercise classes [24], HIFT may provide a feasible alternative. The mean energy expenditure for this study was 509 kcal. This exceeds almost two-fold the average energy expenditure (270 kcal) measured from another HIFT session in a study conducted by Smith et al. [30]. Additionally, the energy expenditure measured from this study was higher than that of high-intensity interval (HIIT) and moderate continuous (CONT) training sessions [27]. Schaun et al. examined the energy expenditure produced by 11 healthy female adults when participating in either HIIT consisting of eight 20 second intervals at 130% of the cadence corresponding to maximum oxygen consumption or CONT consisting of 30 minutes of exercise within 90-95% of the second ventilatory threshold [27]. The average energy expenditure corresponding to HIIT and CONT was found to be 39.91 ± 4.24 kcal and 227.62 ± 31.69 kcal, respectively [27]. Finally, based on this studies energy expenditure results, two HIFT sessions per week would satisfy the 75-150 minutes of vigorous exercise recommendations from the Physical Activity Guidelines for Americans. Metabolic equivalents (METs) refer to the quantity of oxygen consumed while sitting at rest [13]. Standard exercise recommendations dictate that 40% or 60-70% of maximum METs should be achieved during aerobic training for poorly conditioned and typical healthy individuals, respectively [7]. The mean METs from the present study were measured to be 12.1 ± 1.4 kcal/kg/h. This slightly outperforms the average METs of 11.5 ± 0.91 kcal/kg/h measured in healthy women from a similar HIFT class conducted by Browne et al. [6]. Given that METs greater than or equal to 6 correspond to vigorous exercise intensity parameters [36], the results of this study support the hypothesis that HIFT can meet necessary exercise guidelines. Conversely, Nakagata et al. [19] measured the METs corresponding to several of the movements used in our study with longer rest periods in between both reps and sets. In a body weight resistance training (BWRT) slow-exercise program, participants completed a randomized circuit of squats, lunges, push-ups, crunches, hip-lifts, and heel-raises for three sets of 10 reps with a 30-second rest period in between sets [19]. Overall, the sum of the METs corresponding to each individual exercise (16.8 ± 2.5) from the BWRT program [19] was higher in comparison to the present study. However, the additional rest in the BWRT program may have mitigated fatigue and decreased the exercise intensity. The reduced rest periods within the present study’s HIFT regimen, which incorporated a fast-paced cadence of the exercises, produced METs in the same vigorous intensity range as the BWRT program, but in a more time-efficient manner (35 minutes vs. 48 minutes [19]). The potential metabolic benefits may be attributed to the low-intensity transitions interspersed between the high-intensity exercises throughout the HIFT session. Recent research suggests that incorporating intermittent active recovery can increase lactate thresholds higher than those relative to passive recovery [18]. Furthermore, continuous high-intensity exercise may stimulate less efficient fat oxidation, as optimal levels occur during exercise intensities between 47% to 75% [26]. The thirty, 1-minute rounds of exercise interspersed with 10-second low-intensity or rest periods may have been sufficient to confer maximal rates of metabolism.Additionally, the intermittent 1-minute rounds on an Assault Airbike, which includes an upper body ergometer component to its lower body ergometer, undoubtedly added to the unique feature of this HIFT session. Compared to leg pedaling bikes alone, the Assault bike’s upper body ergometer provides additional muscle mass and subsequent stress to the cardiovascular system than leg pedaling alone, as evidenced by the increased heart rate rates (173 ± 5 bpm) found in this study. The average % HRmax of 93% in these women exceeded the cutoff for high intensity exercise (60-84%) as described by the Physical Activity Guidelines for Americans.Several distinctive social components of the HIFT class may have contributed to the high, tolerable energy expenditure in this study cohort. All participants reported the HIFT class to be enjoyable and that they would be able to adhere to it as a standard exercise prescription in their weight-loss program. The social connections and community-oriented gyms where HIFT classes take place can provide a supportive environment that encourages and motivates participants during exercise [28]. Consequently, such an environment can facilitate a positive feedback loop wherein motivational increases result in more enjoyment [9]. As enjoyment increases, HIFT participants have reported a much stronger sense of belonging and desire to adhere to a consistent exercise routine [2]. Given that middle-to-older-aged women cite concerns about their safety exercising outdoors and a lack of companionship during exercise [12], HIFT classes are a viable alternative that will address these concerns and encourage regular exercise. Several study limitations should be addressed. Since the participants for the present study were recruited from only one fitness boutique, these results could be skewed in the event that participants came from other gyms or training experiences. Additionally, a larger sample size could bolster the results of this study and improve the quality of the data given that this is an underrepresented population. Future research should aim to obtain a larger sample size in a multitude of locations to determine if these results are replicable. With the growing necessity for exercise to be incorporated into daily routines and clinical treatment, group based HIFT may offer a viable solution. The results from the present study support our hypothesis that the specific exercises, order, and time-intervals can induce maximal energy expenditure and exercise intensity in postmenopausal obese females. Additionally, the time-efficiency and enjoyability of HIFT programs may lead to increased public participation. Furthermore, the HIFT regimen within the present study fulfilled national exercise guidelines for weekly vigorous-intensity activities, as outlined by the Physical Activity Guidelines for Americans [10]. These results provide a framework for the future implementation of effective HIFT design in postmenopausal females with obesity.
ACKNOWLEDGEMENTS
- We are appreciative of the willingness of devoted participants to give so generously their time to support this work.
Conflicts of Interest
- We declare no conflicts of interest and had no funding for this study. Basecamp Fitness had no role in the study design, data collection, analysis, interpretation, or role in writing the manuscript.