-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2020; 10(1): 23-29
doi:10.5923/j.sports.20201001.04

The Effect of Rib Protector Garments on Trunk Kinematics, Performance, and Perceptions of Quarterbacks During an Overhand American Football Throw
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMarika A. Walker1, Yumeng Li2, Christine O. Samson3, Kathy J. Simpson1, Tim Foutz4, Cathleen N. Brown5
1Department of Kinesiology, University of Georgia, Athens, GA, USA
2Department of Health and Human Performance, Texas State University, TX, USA
3Department of Kinesiology and Outdoor Recreation, Southern Utah University, Cedar City, UT, USA
4Department of Engineering, University of Georgia, Athens, GA, USA
5Department of Kinesiology, Oregon State University, Corvallis, OR, USA
Correspondence to: Yumeng Li, Department of Health and Human Performance, Texas State University, TX, USA.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Rib protectors may help reduce serious rib injuries to American football quarterbacks or offer additional protection following injury. However, offensive players may not wear them if perceived to hinder athletic performance. The study’s purposes were 1) to determine if stiffness of two rib protector garments affected trunk axial-rotation kinematics and performance of a football throw, and 2) to determine whether perceptions of mobility and performance were altered before and after the throws. Twelve male quarterbacks completed rib protector perception scales before and after maximal effort throws during each rib protector condition: soft-rib, hard-rib, and control (compression shirt). Trunk kinematics, ball speed, throw error, throw time and perception scores of each rib protector were compared to control using non-inferiority testing. Neither rib protector was inferior to control for trunk kinematics or performance measures. 95% confidence interval of difference scores for most kinematic and performance variables included zero. Hard rib mobility was perceived to be inferior before and after the throws compared to control (difference = 23% - 47%). However, individuals responded differently to each rib protector for perception outcome measures. Both rib protectors can be recommended because neither appeared to hinder throw performance or trunk kinematics. It is important that a given individual quarterback is able to select the one that he feels the most comfortable and confident wearing.
Keywords: Passing, Mobility, Throwing accuracy, Kinematics, Non-inferiority testing
Cite this paper: Marika A. Walker, Yumeng Li, Christine O. Samson, Kathy J. Simpson, Tim Foutz, Cathleen N. Brown, The Effect of Rib Protector Garments on Trunk Kinematics, Performance, and Perceptions of Quarterbacks During an Overhand American Football Throw, International Journal of Sports Science, Vol. 10 No. 1, 2020, pp. 23-29. doi: 10.5923/j.sports.20201001.04.
Article Outline
1. Introduction
- During an American football game, offensive players are subjected to high impacts from defensive players, with momentums of up to 1,215 kg ∙ m/s [1], leading to acute injuries (ranging from mild to fatal) or long-term chronic effects on various locations of the body. Trunk impacts are concerning for two reasons. First, high impact hits by opposing players often occur to the trunk, now the only area on the player’s body where tackles and blocks are not regulated [2]. This may partly explain the increased number of injuries to the spine and axial skeleton in the U.S. National Football League, from an average of 197 per year (2000-2010) to 235 per year (2012 – 2013); total rib injuries during these two periods increased from 86 to 97 [3], [4]. Second, lower-trunk impacts are troubling because they could result in serious injuries, such as rib fractures, costal cartilage ruptures and even potentially fatal solid organ injury (e.g., splenic or kidney rupture) [2], [4]–[7]. Rib and abdominal region protectors could reduce prevalence and/or the severity of aforementioned injuries if more widely used [8], [9]. The severity of an impact could be reduced by padding materials through deformation of structures and increases of impact duration. However, the effectiveness is difficult to ascertain at present, because evidence of injury-prevention efficacy, prevalence of use, and user compliance are not yet known. Consequently, the decision to have athletes wear preventative rib protection is not based on evidence, but on personal experiences and perceptions of the equipment. There are untested concerns that rib protectors may adversely affect performance achievement, the primary goal of an athlete. These concerns likely are based on perceptions that protectors restrict trunk motion, thereby reducing throwing accuracy and speed. Rib protector characteristics, such as compression, rigidity, and/or bulkiness of the protective padding in the compression shirt, likely create these perceptions. In turn, athletes may not wear the protector if these characteristics are perceived negatively, as shown previously for use of other prophylactic injury devices (e.g., joint braces) [10]–[12]. Biomechanics of quarterback throwing has been reported in very few studies that primarily focused on upper extremity (e.g., shoulder and elbow) kinematics and kinetics [13], [14]. The effect of trunk motion on throwing performance is not well understood. Moreover, there is no scientific evidence that performance or performance components (e.g., movement quickness, axial trunk mobility) are adversely affected by rib protectors. Therefore, quantitative evidence for making an informed decision about wearing a device that could improve a player’s safety is needed. It also is crucial, if the athletes’ perceptions of performance and performance characteristics are negative, to begin identifying the characteristics of the rib protection that contribute to these perceptions and to determine if they translate to decreased throw performance and trunk mobility. If they do translate, negatively perceived characteristics may be modifiable in production process or design.Therefore, the first purpose of this study was to determine if stiffness of rib protector garments affected trunk axial-rotation kinematics and performance of a football throw. A second purpose was to determine whether protector stiffness influences quarterbacks’ perceptions of performance and mobility and whether perceptions change after the throw. We hypothesized that trunk kinematics and throwing performance would not be influenced by rib protector garments. We also surmised that prior to performing the throwing task, athletes would perceive the rib protectors to be restrictive and awkward, and thus perceived score mobility (ability to move freely) and throw performance would be lower than the control condition. However, after performing several throws, the perception scores for mobility and performance were anticipated to increase to be comparable with the control condition.
2. Page Layout
2.1. Participants
- Twelve male quarterbacks (age: 23.8 ± 4.4 y, height: 179.9 ± 4.9 cm, mass: 89.6 ± 9.9 kg) were recruited in this study. The inclusionary criteria were (1) having competitive quarterback experience (high school varsity, collegiate, or professional); (2) being physically active; (3) being healthy without history of spinal surgeries, tumor, fractures, scoliosis, or other diagnosed spinal disorders; and (4) have undergone formal rehabilitation and returned to the previous level of play if there was any upper extremity surgeries or injuries to the throwing arm. Institutional approval of protocol and informed consent was obtained before the study was conducted.
2.2. Instrumentation and Materials
- A seven-camera Vicon MX™ motion capture system (Vicon®-MX40, Vicon Motion Systems Ltd., UK) was used to capture marker locations at 240 Hz. Six 14-mm reflective markers were placed on the pelvis (two anterior superior iliac spine, two posterior superior iliac spine and two peak points of iliac crest) (Figure 1) based on previous research [15]. Four-marker (9.5 mm) cluster sets were placed on the T8 and L3 spinous processes. Two markers were placed on the football and one was placed on the 2nd metacarpal head of the throwing hand to detect the instant of ball release. Additional markers (modified Vicon Plug-In Gait), not used in this study, were also placed on the participant. Vertical ground reaction forces (VGRF) were obtained using a force plate (Bertec Corporation, Ohio, USA) at 1200 Hz to later determine the start of the phase of interest. The 45cm-radius circular wood throwing target was chalked to identify ball placement (Figure 2) and was located 9.1 m in front of participants. A radar gun (Bushell Corporation, Overland Park, KS, USA) was used to measure ball speed (km/h) after release and was held by a researcher next to the throwing target.
 | Figure 1. Marker setup. (a) Front view and (b) back view of the full marker set (modified Vicon Plug-In Gait) used for motion capture. Additional markers not used in this study were placed on the participant. (c) An assembled example spinal marker cluster set. (d) An unscrewed spinal marker cluster set. Marker sets placed on the T8 and L3 vertebrae were made of four 9.5 mm-diameter markers attached to a base consisting of a 6.6 mm-diameter vertical plastic rod crossed with a 9.7 mm-diameter horizontal plastic rod; a 3 mm-diameter screw, protruding from the 3-marker plane, covered with black tape; and a 19.1 mm-diameter solid plastic base with a 4 mm-diameter screw projecting from it into the horizontal rod. The base was placed on the skin and fed through a small hole in the garment |
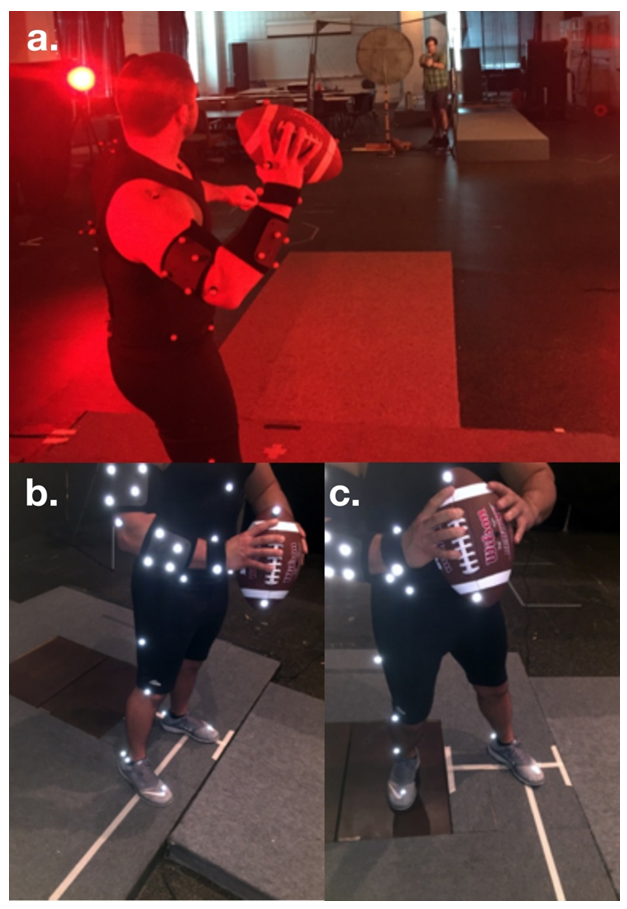 | Figure 2. Experimental setup and tasks. (a) The experimental setup for this study. The participant threw the ball to a target 9.1 m away while a researcher measured ball speed with a radar gun. (b) Starting position for the throwing task. (c) Position after single-step drop-back and before throw |
 | Figure 3. The rib protectors tested in this study: (a) soft-rib and (b) hard-rib. All logos were covered to avoid bias due to brand. Padding on the sternum and along the spine was made of a harm foam, not plastic like the rib inserts. The control condition consisted of the hard-rib compression shirt without the plastic inserts |
2.3. Protocol
- A two-minute throwing warm up and five practice throws were performed before data collection. Rib protector conditions (soft-rib and hard-rib and control) were tested in a counterbalanced order. When switching rib protector condition, the base of the spinal marker cluster was left on the participant’s skin and fed through a 4 mm-diameter hole in the rib protector garment (Figure 3d). The marker cluster was then screwed on the base during data collection. The participants rated mobility (i.e., how mobile do you feel? On a scale from “cannot move” to “can move easier than ever before”) and performance (e.g., how well do you think you could complete a pass with this in a game setting? On a scale from “cannot complete a pass” to “can complete a perfect pass”) for the rib protector condition on a hard-copy 10 cm (0 cm = worst; 10 cm = best) visual analog scale. When an aural signal sounded, participants stepped back on the force platform and threw the ball as quickly and accurately as possible to the target (Figure 2). After each trial, throw error was measured as the distance between the center of the ball mark left on the target to the center of the target. Five acceptable trials were collected. From visual observation, a trial was acceptable if the back foot landed on the force platform, and the ball hit the target, leaving a visible mark for error measurement. After throws for a given rib protector condition were completed, the participant completed the visual analog scale again. A 20-min break was given between two rib protector test conditions. Instructions of the test protocol were given by the same investigator.
2.4. Data Reduction
- The phase of interest was from touchdown of the throwing arm’s ipsilateral foot (i.e., instant when VGRF > 10 N) to ball release. This phase was chosen because it included the time interval when important axial trunk kinematics that contributes to ball speed and accuracy occur. Three-dimensional coordinates of the markers were reconstructed using Vicon’s Nexus software proprietary algorithm (v. 2.4). The axial rotation angle of T8 relative to L3 segment was calculated using the Cardan method (X-Y-Z sequence) as the lower-trunk rotation angle. Only axial rotation direction was analyzed because it was the primary motion in the lower-trunk during a football throw based on our pilot study. We analyzed the relative angle between T8 and L3 because all the padding materials of the rib protectors were located between T8 and L3 and the lower-trunk was the main region restricted by rib protectors. Peak values of angular displacement, angular velocity, acceleration and time to peak angular acceleration were calculated to assess the influence of rib protectors on trunk motion. Performance-related variables including time to complete the throw (time from the aural cue to ball release). Ball release was determined by the change in the distance between ball and finger markers. Ball speed and throw error were used to determine if throwing performance was affected by rib protectors. For perception variables, the distances from 0 cm to the participant’s marks on each VAS were measured manually.
2.5. Data Analysis
- To test if a given rib protector did not have lower values compared to control, non-inferiority tests using the 95% confidence interval (CI) of the difference score (rib protector value - control value) were conducted for each variable. The objective of the non-inferiority tests is to demonstrate that wearing rib protectors is not inferior to that without rib protectors. We utilized the non-inferiority tests instead of traditional comparative tests (e.g., repeated measures), because no significant difference does not imply equivalence or noninferiority [16]. The non-inferiority margin was set at one standard deviation of the control condition, as it was a conservative estimate of typical inter-individual variability of throwing and no prior values of minimal behavioral differences for these spinal motions exist [17]. Statistical power was calculated for each non-inferiority test. In addition, corresponding individual participant non-inferiority tests were conducted to determine if participants were affected differently by the rib protectors. Both pre- and post-throw perceptions were compared to the control condition using non-inferiority tests with 95% CI for the mobility and throw performance.
3. Results
- For the group outcomes, both rib protectors were shown to be non-inferior to the control condition for all performance (Figure 4a) and trunk kinematic (Figure 5a) variables. No outliers were detected in individual or group outcomes. For the soft-rib condition, all difference-score 95% CI included zero. For the hard-rib condition, all difference-score 95% CI included zero except for throw error. However, the 95% CI was still within the non-inferiority margin. For non-inferiority tests of the soft-rib protector, all variables had power above 0.8 except for trunk angular displacement (1-ß = 0.72) and throw error (1-ß = 0.57). For the hard-rib non-inferiority tests, all variables had power above 0.8 except for throw error (1-ß = 0.51).
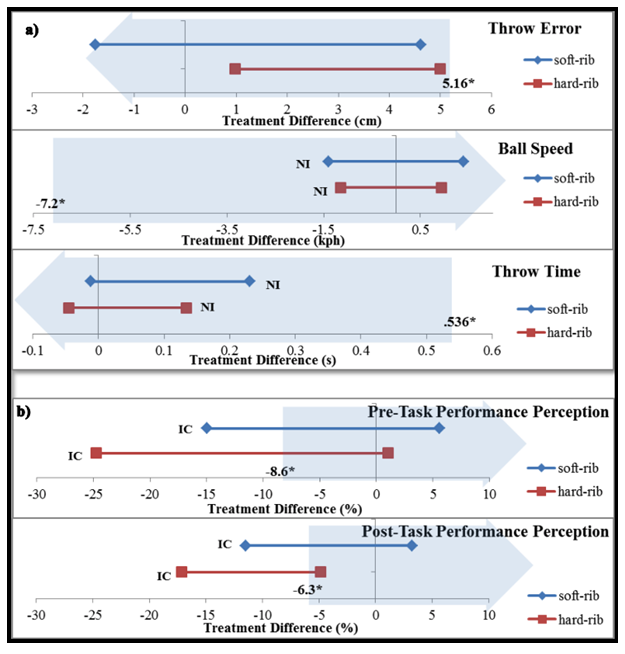 | Figure 4. Group performance non-inferiority testing. (a) Outcomes of group non-inferiority testing for performance variables showed non-inferiority for both rib protectors. (b) Perception of performance was inconclusive at both time points. Thin lines show 95% CI of treatment difference (protector – no-rib) for each rib protector. Large arrow represents the non-inferior range: tail is boundary at the non-inferiority margin (value in bold text and *) and continues infinitely in the more ‘favorable’ difference direction. NI = non-inferior to NO-RIB and IC = inconclusive |
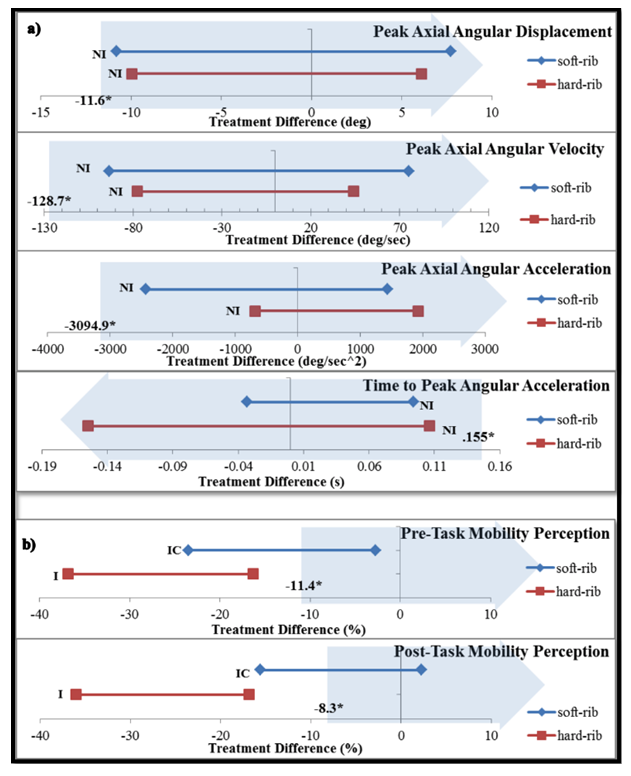 | Figure 5. Group mobility non-inferiority testing. (a) Outcomes of group non-inferiority testing for mobility variables showed non-inferiority for both rib protectors. (b) The hard-rib was inferior to the control in perception of mobility. Thin lines show 95% CI of treatment difference (protector – no-rib) for each rib protector. Large arrow represents the non-inferior range: tail is boundary at the non-inferiority margin (value in bold text and *) and continues infinitely in the more ‘favorable’ difference direction. NI = non-inferior to NO-RIB, I = inferior to NO-RIB, and IC = inconclusive |
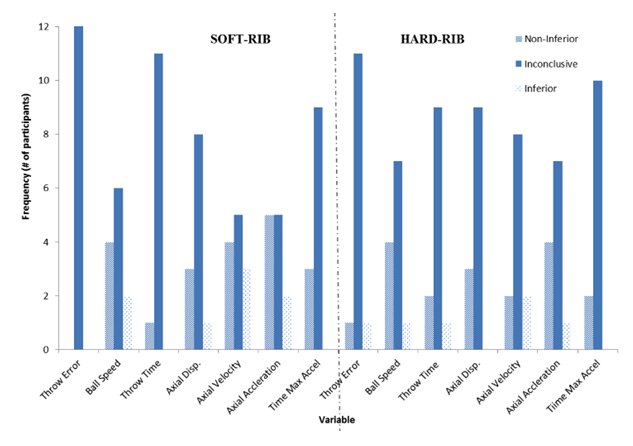 | Figure 6. Frequencies of individual participant non-inferiority testing outcomes |
4. Discussion
- The present study was the first one to determine if stiffness of rib protector garments affected trunk kinematics and performance of a football throw. Overall, we hypothesized that both soft and hard rib protectors would be non-inferior to the control for the trunk kinematics and throw performance. This hypothesis was supported. In addition, it was predicted that participants would perceive both rib protectors to be inferior to the control before completing the throwing task; but perceptions would be improved post-throw. However, this hypothesis was partly supported. Trunk axial rotation could contribute considerably to the total body angular momentum and transfer the angular momentum to the adjacent distal segments (e.g., upper trunk and arm) through a “kinetic chain” [18], [19]. Moreover, trunk rotation is crucial to cause the arm to lag behind the accelerating trunk and this lag could result in greater external rotation of the shoulder beyond its active range of motion. In the present study, lower-trunk rotation was analyzed because it was the main region restricted by rib protectors. Our findings suggest that lower-trunk axial rotation is not influenced by the stiffness of rib protectors during a short-distance football throw. There are two potential explanations of the unaffected lower-trunk rotation. Firstly, intervertebral motion that contribute to trunk motion during the football throw task may not be large enough to be constrained by rib protectors. Secondly, it is possible that trunk muscles (e.g., external oblique) are able to produce the torque necessary to overcome the mechanical restrictions of the rib protectors. Previous research reported that external oblique could primarily contribute to contralateral rotation range of motion and torque generation [20]. Similarly, previous research investigated the effect of a hard, “nearly complete-restriction” torso brace (clavicle to the pelvis) on trunk kinematics and performance during a baseball pitch and observed that wearing the brace showed no changes in peak power, angular velocity, trunk axial rotation torque, and time in the acceleration phase [21]. Therefore, we suggest that the rib protection padding in the lower rib area of each compression shirt does not hinder performance or the ability for a quarterback to move during completion of a short throw, regardless of stiffness of rib protectors. Future research is still warranted to investigate any potential compensational movements (e.g., upper trunk or shoulder motion) caused by rib protectors. It is also beneficial to study other types of throw (e.g., intermediate or long-distance throw). Most performance outcomes were not influenced by rib protectors possibly because of unaffected trunk motion. Even with restricted trunk motion, throw performance may not be significantly influenced by the rib protectors because most of the work required to generate high throw speed is generated at the hips [22], [23]. However, there is some slight indication that the small effects that were experienced when wearing hard-rib protectors may have translated to throw error, because 95% CI of the difference did not include zero. The results indicated that participants exhibited statistically greater throw errors when wearing hard-rib protectors. However, the difference may not be behaviorally significant because it is still within the non-inferiority margin. In addition, non-inferiority testing of throw error was underpowered for the hard-rib (1-ß = 0.51) and insufficient power usually suggests inconclusive results. Pre- and post-throw performance perception results were inconclusive for both rib protectors. The high variability of perception scores likely caused the inconclusive results. Pre-throw mobility perception was inferior to the control. After throwing, all participants again perceived the hard-rib was worse than the control. The hard-rib was perceived to reduce mobility due to the stiffness of the protective insert that felt restrictive because it was molded to their bodies. In addition, greater weights of the hard-rib may play a role in perceived limited trunk motion. Interestingly, perceptions after throwing did not improve for either rib protector. For both perception variables, there was an increase in number of participants (performance: + 5; mobility: + 2) who perceived the soft-rib protector inferior to the control after throwing. Additionally, more participants (+ 2) scored the hard-rib protector lower for post-throw performance perception. However, their perceptions were not supported by our data (i.e., trunk kinematics and throw performance described earlier). Future studies are still needed to confirm our present findings and encourage football players to wear more protection by convincing them that their performance will not be hindered. Then football players may build up confidence due to the feeling of having less risk of sustaining injury and thus perform better [24].There were several limitations in the present study. First, the sample size was somewhat low due to the limited number of eligible competitive quarterbacks in the recruitment area. Among the eleven variables (i.e., trunk kinematic, throw performance, and perception), the small sample size may have resulted in lower statistical power (less than 0.8) for several variables. Second, the ideal method for setting the non-inferiority margin is to use previously reported behaviorally meaningful differences because the margin has an influence on the test outcomes. However, these differences have not been reported by previous research surrounding overhand football throw. Therefore, an alternative method using the variability of the variables (one standard deviation) to set the margin was employed as suggested by previous research [25]. The markers used for trunk kinematics were placed on the skin and therefore the skin motion artefact may affect the kinematic results, as with any motion capture study. However, the bases of the marker clusters were reinforced with Cover-roll® adhesive bandage to minimize motion and using a six-degree of freedom pose estimation optimization method for computing the position and orientation of segments [26]–[29]. Finally, there were some variations in age, skill levels and experience with rib protectors among the participants, which may have affected their throw performance and perception.
5. Conclusions
- In summary, hard-rib and soft-rib protectors were not inferior to the control condition for lower-trunk rotation and throw performance during an overhand football throw. Still, athletes perceived rib protector garments to affect these variables. Our results may be used to convince athletes to wear rib protectors if the protectors are also proven to be efficacious for preventing injury or attenuating rib/abdominal injury severity in American football quarterbacks. As there is little influence of rib protector stiffness on performance or trunk kinematics, it is important that a given individual quarterback is able to try different rib protectors and select the one that he feels the most comfortable and confident wearing.
ACKNOWLEDGEMENTS
- We thank the companies that provided the rib protector garments used in this study and our undergraduate researchers (alphabetically): Julia Dolgetta, Cristian Escalera, Morgan Green, Holly Kapella, Chandler Mulford, Haley Pierce, Jeremy Raiford, Christopher Suter, and James Tyson.