Yahya Doğar1, Abdulvahit Doğar2, Sevim Atila Kabasakal3
1İnönü University, Sports Science Faculty, Malatya, Turkey
2Atatürk University, Vocational School of Health Services, Erzurum, Turkey
3Republic of Turkey, Minisitry of Health, Ankara, Turkey
Correspondence to: Yahya Doğar, İnönü University, Sports Science Faculty, Malatya, Turkey.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The aim of the study is to compare the results of patients with chronic lumbar disc herniation whose type of treatment did not come to an agreement. The results will be compared in terms of pain and lower back range of motion by Nottingham Health Protocol (NHP) (pain, physical capacity, fatigue, sleep disorder, social isolation and emotional status). The patients have been given medical treatment along with resting for two weeks. What is more, patients have been applied physiotherapy and they have been informed about a healthy lower back. Twenty-eight patients were divided into two groups. The first group (DD group) were applied the hot pack (HP) + ultrasound (US) + diphase current (DF) + curt period (CP) and the second group (IF group) were applied HP + US + vacuum with interferential current. Their superiority to each other have been analyzed. SPSS 6.0 software has been used to evaluate the recorded data. At the end of the study, significant differences have been found in terms of recovery, pain relief, improvement of physical activities and psychosocial recovery among patients treated with interferential currents and diadynamic currents. It is concluded that the combination of IF currents and vacuum, combined with US, is an effective treatment method for patients with chronic lumbar disc herniation.
Keywords:
Lower Back Pain, Diadynamic Current, Physiotherapy, Interference Current, Intervertebral Disk Displacement
Cite this paper: Yahya Doğar, Abdulvahit Doğar, Sevim Atila Kabasakal, Differences of Treatment Effectiveness between Diadynamic Currents and Interferantial Currents in Patients with Lumbar Disc Herniation1, International Journal of Sports Science, Vol. 9 No. 3, 2019, pp. 54-60. doi: 10.5923/j.sports.20190903.02.
1. Introduction
High prevalence of low back pain (lumbar pain), which may cause long lasting functional losses and affect negatively the quality of life has increased the importance of specific assessment and treatment methods used for it [1]. The treatment of low back pain, which affects both the individual and the society, is important to increase economic and social efficiency. It is as important as the treatment of the disease that the most effective methods in the treatment of low back pain are revealed and presented to the patients in a short time. In this respect, a rapid, correct and effective treatment of low back pain is important to find out which diadynamic and interferential currents are more effective in the treatment of low back pain. Disability is defined as reduced capacity in daily activities and a limitation in the patient's performance compared to a person of the same age and gender. The most widely used disability scales for low back pain are Roland, Oswestry, Million, Waddell and Sickness Impact Profile [2].In addition to medical treatments, superficial heaters, deep heaters and electric current treatments are also used in the treatment of lumbar disc hernias. Besides the muscle relaxant, pain-relieving properties of the heat, it accelerates the repair process of tissues by accelerating the feeding of the applied tissues and the elimination of metabolic residues [3].The main flow types used in the treatment are Hot Pack (Hot Water Packs), Deep Heaters, Ultrasound, Diadynamic currents from low frequency currents, Interference currents from medium frequency currents [4].The most important advantages of diadynamic currents compared to old currents are that they have much stronger hyperemia and pain relief effects. The main advantages of the interfering currents are that the current under the electrodes, i.e., the current in the skin, is pure medium frequency (MF). As is known, the higher the frequency, the less the resistance of the skin. Therefore, because the skin irritation will be reduced very much, the patient will not be uneasy and will have the opportunity to obtain a deeper effect by using higher current intensity [5].In one-year and two-year prospective and controlled studies by Hazard and Mayer, functional restoration treatment was evaluated according to individual pain assessment, physical capacity and measurements of the return to work, in patients with chronic low back pain. Improvements in all parameters were observed at one and two-year follow-up. Active functional restoration program did not increase the risk of back pain and attacks. In these studies, where the rate of return to work was very high, the functional restoration program was administered for three weeks, 53- 57 hours per week [6].In a one-year prospective controlled study by Sachs, the work boosting program for patients with chronic low back pain included muscle stretching and relaxation exercises, as well as dynamic strengthening exercises for back extensors and abdominal muscles. Cycling, walking and gymnastics program was also applied in every session. In this study, it was found that the program for increasing work resilience increased the rate of return to work when considered objective measurements [7].In the study by Kraus et al over the patients with chronic low back pain, the effect of a 6-week exercise program, including strengthening, stretching and relaxation exercises, was investigated and a healing rate of 80% was observed in all patients including those with back pain after spinal surgery. In this study, the decrease in pain was found to be associated with increased muscle strength and waist elasticity [8].In a randomized and one-year prospective study by Gundeval et al., nurses and nurse assistants are given exercises that increase the muscle strength, endurance and muscle coordination for 13 months during work hours and about 20 minutes each day except holiday and off days. In the exercise group, there was a significant decrease in the number of the days with compliance of low back pain on off days and the intensity of pain and the strength of back extensors increased by 20% [9].Koes et al. evaluated 16 randomly controlled studies covering the period between 1965 and 1990 and selected by medline review considering the exercise therapy in patients with low back pain. In the evaluation where the highest score was 100, in only four studies the score was above 50 [10].Schönle emphasized that randomly controlled studies on the traditional treatment of low back pain could not demonstrate the superiority of any treatment method over the others and that treatment success was not better than spontaneous recovery rate [11].In the study of Deyo evaluating 59 studies on traditional treatment of low back pain based on 11 methodological criteria, it was found that most of the studies were not reliable enough to provide adequate scientific support [12].The most important risk factors were reported in a three-year study of Frymoyer conducted over 1221 (male) cases to be recurrent lifting heavy loads, motor vehicle driving, full-body vibration, and the time spent in the position of bending forward [13].Burton conducted a study over 958 cases. All of the cases were selected from people who are currently doing or did amateur sports in the past. It was determined that doing amateur sports in childhood or youth is not related to the occurrence, frequency and age of the onset of back pain [14].No difference was found between gender and disability in accordance with the study conducted by Tuncer et al. As a result, the most effective factor in disability was found to be advanced age following pain. Severity of pain and disability score were not associated with MRG findings. As a good linear correlation was determined between VAS (Visual Analog Scale) and Oswestry scores, an opinion was obtained related only to VAS measurement and Oswestry scale parameters and the level of disability could be determined in this way [15].
2. Method
This study was carried out over a total of 28 patients (19 females, 9 males) diagnosed with lumbar disc herniation who were admitted to İnönü University, Turgut Özal Medical Faculty, Physical Therapy and Rehabilitation Department polyclinics.Selection criteria of patients were in 20-64 age group. Other selection criterias included diagnosis of the disc herniation through computed tomography examination, absence of findings of spinal stenosis, absence of significant degenerative changes, unrelieved pains in spite of two-week bed rest and medical treatment. Age, gender, occupational status and educational status of the patients were recorded.The patients were divided into two groups, 14 in DD (diadynami) and IF (interference) groups, and the 15-day physical therapy and rehabilitation program, which forms the basis of the present research, was started.DD and FF groups received 15 sessions of hot pack each session of which lasted 20 minutes, and a total of 15 sessions of ultrasound, each session of which lasted 10 minutes at 1.5 watts/cm. In these applications, DD group was subjected to 10 sessions of dipase flow which is among diadynamic current varieties and each session of which lasted 2 minutes and 4 minutes lasting curt period current.The isoplanar flows from the interferential currents (together with the vacuum) were applied to the IF group for 20 minutes for 12 sessions. Therefore, the research is an experimental research.Statistical analysis of the recorded data was conducted using SPSS 6.0 package program. Mann-Withney U was used as a test statistic.Lumbar Extensors: The patient is in a long sitting position at the knee extension.Patients were asked to touch their tiptoes by extending their arms forward. In the cases where subjects were able to touch their tiptoes, lumbar extensors were considered to have no shortness of muscle in the lumbar extensors and vice versa. Hamstrings: Patients lie in a supine position with their arms in reverse T form and their legs are in extension position. The physiotherapist holds the leg to be tested from its heel with one of his/her hands while flexing the leg with other hand by maintaining the knee extension position. If the hip flexion is 70 degrees or above, the hamstring muscle length is considered to be normal while if less then it then the hamstring muscle is accepted to be short and stiff.Hip flexors: The patients lie with their legs hanging from the table edge or their hips and legs are in extension in supine position. When a leg is pushed to the chest in knee – flexion position by a physiotherapist, the other leg to be tested should be stuck in bed and hip should maintain the extension of the hip. If the leg is away from the bed, the hip flexors are accepted to be short. It is accepted to be normal if the leg is stuck on bed [16].Flexion: The patient is standing upright. In the measurement of back flexion, the goniometer is placed on the pivot point, trochanter major of the femur. The upper part of the goniometer is placed parallel to the body and the lower part is to the femur. The subject is asked to bend forward. The degree of bending of the subject is recorded.Extension: The subject is asked to move the upper body back while standing straight and again measurement by goniometry is conducted and the degree of flexion back is recorded.Lateral Flexion: The subject is asked to bend to the left and right side while standing steadily. The degree of bending of the subject is measured with a goniometer and the degree of bending is recorded [16].Visual Analog Scale (VAS): On the Visual Analog Scale, a ruler with numbers from 0 to 10 is defined, and a patient with a pain of maximum severity at 10 with no pain in 0 is described and the patient is asked to express the severity of pain with a number between 0 and 10. Severity of pain in the subject is considered to be increasing as the pain intensity increases to 10 and reach maximum at 10 [3].Nottingham Health Protocol: Nottingham Health Profile (NHP) is a questionnaire form designed to measure the social and individual effects of a disease. This form is used to measure quality and maintenance of wellness. The main purpose of using the form is to define the social and psychological problems and quality of life of patients with chronic low back pain.Patients are evaluated with NHP questionnaires which contain 38 questions in six areas on pre-treatment, post-treatment, energy (fatigue), pain, emotional state, sleep, social isolation and mobility (physical activity). Patients are asked to answer questions in the form of yes / no. NHP has been developed for a wide range of applications. Pregnant women, patients with fractures, osteoarthritis and peripheral vascular diseases are used in many different groups [17].Test of Raising Leg Straight (TRLS): The subject, lying on his back, bends his leg up without bending the knee. If the subject's back pain occurs below 70 degrees, the diagnosis of disc herniation is considered positive [3].Lumbar Shober: Lumbar Shober: Spina Iliac is marked 10 cm above and 5 cm below the anterior superior. The patient is asked to lean forward. An increase in the distance of 15 cm is measured with a tape measure. A distance 5 to 10 cm is accepted to be normal and if a measurement is performed below these values, it is pathological [3].Distance of Hand to floor: The patient is asked to lean forward and the distance between the tip of the third finger and the floor is measured with a tape measure. Normally, hand - floor distance should be 0 cm in subjects, but it differs from 0 in patients with disc herniation [3].Oswestry Low Back Pain Disability Questionnaire: Modified Oswestry Disability Questioning, which is divided into 10 sections, is performed in order to evaluate the various limitations of pain in daily life activities of patients with chronic low back pain in the conditions such as liftingheavy loads, sleeping and traveling. The severity of pain, the degree of pain change, personal precautions, liftingheavy loads, walking, sitting time, standing, sleeping, social life changes and travel sections are represented by a figure between 1 and 6 on the scale (1 - no limitation, 6 - maximal limitation).
3. Results
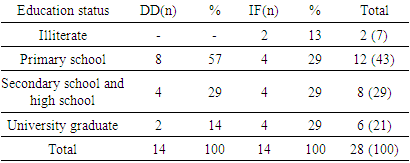
Data obtained from the subjects through questionnaire and the examination tried to be expressed and interpreted by transforming it into tables in order to make it more comprehensible.Table 1. Education status of the patients in the groups
 |
| |
|
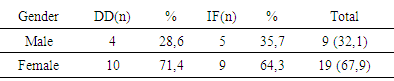
It is seen in Table 1 that 43% of the subjects are primary school graduates followed by secondary school + high school graduates (29%), university graduates (21%) and illiterate (7%). According to these data, as the levels of education of individuals increase, lumbar disc herniation reduces.Table 2. Gender distribution of the subjects
 |
| |
|
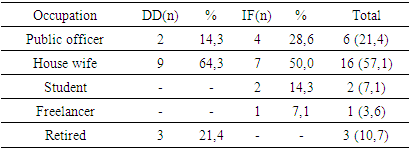
In Table 2, it is seen that the females in both groups have a lumbar disc herniation disease with 68%, which is more frequent than males.Table 3. Occupation distribution of the subjects
 |
| |
|
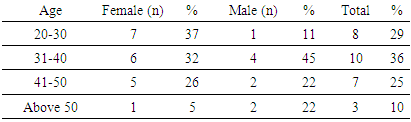
The findings obtained in Table 3 support those in Table 2. However, public officers rank the second (21%) among the patients with lumbar disc herniation.Table 4. Gender and age groups
 |
| |
|
The disease is more common in the age group of 31-40 years. However, lumbar disc herniation is more frequently seen among males between 20 and 30 years old and females between 31 and 40 years old.Table 5. Disc levels of patients
 |
| |
|
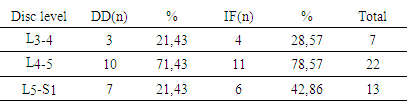
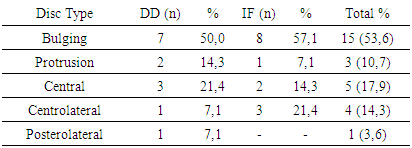
Pathology frequency is L4-5, L5-S1, L3-4. Lumbardisk herniation is seen more frequently at L4-5 levels. Table 6. Disc types among patients
 |
| |
|
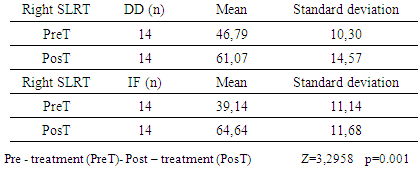
It is seen from the patient groups that bulging is the most prevalent disc type among them. Bulging attracts the attention with its frequency rate 53.6% higher than all other pathologies. Table 7. Mean values of pre and post treatment right straight leg raising test (SLRT) in DD and IF groups
 |
| |
|
It is understood that patients included in the IF group responded more positively to treatment, and perform the expected straight leg raising movements more successfully than those performed by DD group. (Z = 3,0443 p = 0,0017).Table 8. Mean values of pre and post treatment left straight leg raising test (SLRT) in DD and IF groups
 |
| |
|
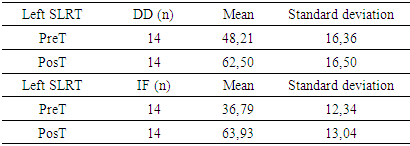
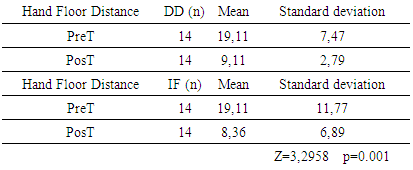
It is seen that patients included in the IF group also responded more positively to treatment, and perform the expected straight leg raising movements more successfully than those performed by DD group (Z=3,4837 p=0,0003).Table 9. Mean values of pre and post treatment hand floor distance in DD and IF groups
 |
| |
|
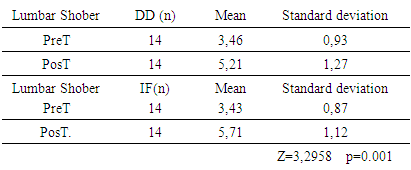
The treatments of both groups were found to be significant. According to the statistical results of the difference between the groups in order to evaluate whether there is a difference between the activities of the group, the IF group did not give a more meaningful result compared to the DD group (Z = 0.9001 p = 0.36). In other words, there is no difference in the efficacy of treatment in both groups.Table 10. Mean values of pre and post treatment Modified Lumbar Shober measurements in DD and IF groups
 |
| |
|
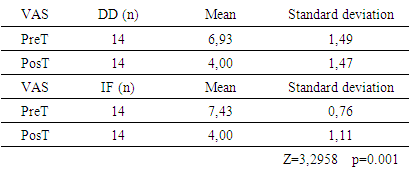
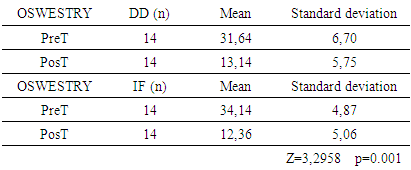
IF group showed more significant results than DD group. (Z = 2.2060 p = 0.02). In other words, the IF group where interferential currents are applied is more successful than the DD group in the low back movement range.When we look at the statistical results of the difference between the groups, it was recorded that the IF group gave more meaningful results than the DD group (Z = 1,8876 p = 0.05). IF group was more successful than DD group.It is understood that the interferential currents applied to the IF group give more positive results than the diadynamic currents applied to the DD group (Z = 2,3374 p = 0,01).Table 11. Mean values of pre and post treatment VAS measurements in DD and IF groups
 |
| |
|
Table 12. Mean values of pre and post treatment Oswestry measurements in DD and IF groups
 |
| |
|
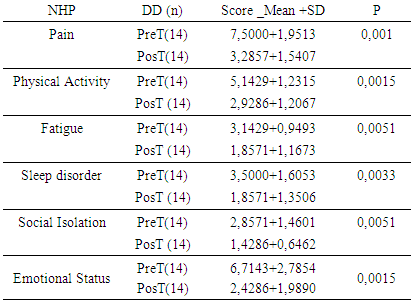
Table 13. Mean values of pre and post treatment NHP measurements in DD group
 |
| |
|
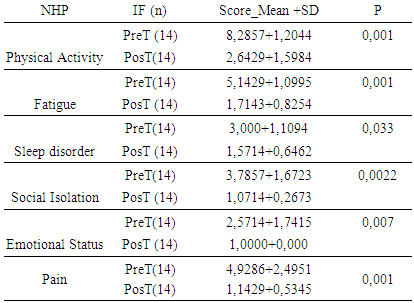
Tablo 14. Mean values of pre and post treatment NHP measurements in IFgroup
 |
| |
|
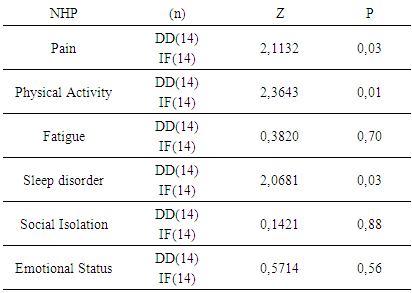
Table 15. P values of NHP measurements for the groups
 |
| |
|
According to the statistical results of the difference between the groups in order to evaluate whether there is a difference between the activities of the IF group gives more meaningful results in terms of pain, physical activity, sleep disorder than DD group, but in terms of fatigue, social isolation, emotional status the two groups did not exhibit significant differences.
4. Discussion and Conclusions
43% of the subjects are primary school graduates according to their educational background, and this is the determinant of the risk of developing the disease. From this point of view, there is an adverse relationship between education level and prevalence of the disease. Therefore, it is understood that individuals with higher education levels are sensitive to the conservation of their health.For the gender status, females included in the DD and IF groups (68%) were more likely to have lumbar disc herniation than men were (32%). It may be because women work in heavy household and heavy agricultural conditions compared to men.According to occupational status of the subjects, the results show that the rate of housewives with lumbar disk herniation disease is 57%, which is significant. This may be considered natural in living conditions of Turkey. When considered occupational groups, public officers rank the second row with a prevalence rate of 21%. This may result from the fact that officers spend their worktime on a desk without doing any physical activities and sitting in a suitable position.When considered age groups, it is seen that the women in the age range of 20-30 years old had lumbar disc herniation disease in the rate of 36% while men in the 33-40 years old range had the disease in the rate of 40%. Such a difference between women and men in terms of age groups may result from the fact that women, especially in pregnancy and postpartum periods may not have a healthy life. However, it does not seem to be possible to say whether the age group is decisive or not for the prevalence of the disease among males.Pathology frequency of the subjects in their discs was seen most in L4-5 level. The most important reasons for the occurrence of the hernia at this level are more loading at these levels, the diameter of the central canal is narrower and the amount of movement is higher. Patients in both groups exhibited bulging disk type.The efficacy of diadynamic currents and interferential currents in the treatment of DD and IF groups was found to be significant in themselves. However, it was found that IF group gave more significant results than DD group (Z = 3,0443 p = 0,0017). Interferential current therapy was more effective than diadynamic current therapy.The mean values of the straight leg-raising test were found to be significant in terms of treatment. However, IF group was found to be more effective than DD group (Z = 3,4837 p = 0,0003). Interferential current therapy was more effective than diadynamic current therapy.Although there was a significant difference between the IF and DD groups in the evaluation of pre and post-treatment hand-floor distance, no significant difference was found between each other in terms of efficacy (Z = 2,2060 p = 0,02). The mean values of the VAS measurements before and after treatment were significant in the DD and IF groups. However, it was found that IF group had more effective results than DD group (Z = 1,8876 p = 0,05).The mean values of the Oswestry measurements in the DD and IF groups before and after treatment were found to be significant. However, it was found out that the IF group was more effective in the values of Oswestry measurements before and after treatment, compared to the DD group (Z = 2,3374 p = 0,01).The mean values of the NHP measurements of the DD and IF groups before and after the treatment were found to be significant. According to the statistical results of the differences between the groups, IF groups gave more effective results in terms of pain (Z = 2,1132 P = 0,03), physical activity (Z = 2,3643 p = 0,01) and sleep disorder (Z = 2,0681 p = 0,03 ). However in terms of fatigue (Z = 0.3820 p = 0.70), social isolation (Z = 0.11421 p = 0.88) and emotional state (Z = 0.5714 p =0,56), there was no significant difference between the groups. A similar case was seen in a study by Murat on the effect of Lumbar Traction on Clinical and Functional Status in Patients with Subacute Lumbar Disc Herniation. No change was observed in general mental health, role limitations due to emotional problems, energy / vitality and general health perception in both groups before and after treatment. There was no difference between two groups in terms of change in these parameters [18].As a result, gender, age and occupational factors are the determinants of lumbar disc herniation and the treatment with diadynamic currents is more effective than the treatment interferential currents.
Note
1. This study was accepted as a master’s thesis in İnönü University, Institute of Health Sciences, Physical Education and Sports Department
References
| [1] | Koç, M. & Kılıçhan, B. (2017). Fonksiyonel Bel Ağrısı Skalası’nın Türkçe uyarlaması: geçerlik ve güvenirlik çalışması, Journal of Exercise Therapy and Rehabilitation, 4 (2): 82-89. |
| [2] | Çubukçu, S., Adıç, F., Kılıç, A., Coşkun, E., Topuz, O., Pakdemirli, E., & Akkoyunlu, N. (1996). “Torakolomber Disk Dejenerasyonunda Klinik, MRG ve Osvestry Disabilite Skoru”, Ege fig. Tıp. Reh. Der. 2 (4): 255-260. |
| [3] | Çağlar, N., & Kanuran, Y. (1997). “Lomber Disk Hernisine Bağlı Radikülopatilerin Tedavisinde Epidural Steroid ve Fizik Tedavi Uygulamalarından Alınan Sonuçların Karşılaştırılması” Fizik. Tıp Rehabil. Derg. XXII. 3, 126-130. |
| [4] | Sengir, O. (1989). Alçak Frekanslı Akımlar, Fizik Tedavi Kitabı, Sengir O. (Editors), İstanbul Üniversitesi, İstanbul Tıp Fakültesi Yayınları, Bayrak Matbaacılık. 1. İstanbul. |
| [5] | Tuna, N. (1989). Diyadinamik Akımlar Elektroterapi, Tuna N. (Editor). İstanbul, Nobel Tıp Kitabevi, 97. |
| [6] | Hazard, R.G., Fendwick, J.W. & Kalisch, S.M. (1989). Functional Restoration with Behavioral Support: A One Year Prospective Study of Patients with Chronic Low Back Pain, Spine, Vol 14, No: 2, pp 157-161. |
| [7] | Sachs, B.L., Davis, J.F., & Olimpio, D. (1990). Spinal Rehabilitation by Work Tolerance Based on Objective Physical Capacity Assesment of Dysfunction: A Prospective study with Control Subjects and Twelve Month Review, Spine, Vol 15, No: 12, pp 1325-1332. |
| [8] | Kraus, H., & Nağler, W. (1983). Evaluation of an Exercise Program of Back Pain, AFP, Vol 28, No: 3, pp 153-157. |
| [9] | Gundewall, B., & Liljequist, M. (1993). Primary Prevention of Back Symptoms and Absense from Work, Spine, Vol 18, No: 5, pp 587-594. |
| [10] | Koes, B.W., Bouter, L.M., & Beckermann, H. (1991). Physioyherapy Exercises and Back Pain: A Blinded Review, BMJ Vol 302, pp 1572-1575. |
| [11] | Schönle, C. (1993). Die Effektivitat Konservatier Therapien Bei Chronischen Rückenschmerzen İmspiegel Der Literatür, Gesundh-Wes. 55 pp 227-233. |
| [12] | Deyo, R. A. (1983). Conservative Therapy for Low Back Pain, Jama, Vol 250, No: 8 pp 1057-1062. |
| [13] | Frymoyer, J.W., et al. (1983). Risk faktors in low back pain, J Bone J Surg, 1983; 65 A, 2: 213-219. |
| [14] | Burton, A.K., & Tolitson K.M. (1991). Does Leisure Sports Activity Influence Lumbar Mobility on the Risk of Low Back Trauble, J spinal Disoral, 4 (3): 329-336. |
| [15] | Tuncer, S., Arasıl, T., & Alpar, R. (1992). Kronik Bel Ağrısı Sendromunda Ağrı-Spinal Mobilite Disabilite İlişkisi, J Rheum Med Rehab. 3 (3): 2-9. |
| [16] | Otman, A., Saadet H., & Demirel, A. S. (1995). Tedavi Hareketlerinde Temel Değerlendirme Prensipleri, H. Ü. Fizik Ted. ve Reh. Yüksekokulu Yay: 16 Ankara, s. 37-39. |
| [17] | Saraç, A., Ferda, J., Erdoğan, K. N., Ataoğlu, S., Gür, A., Çevik, R., & Akkuş, Z. (1997) “İnmeli Hastalarda Nottingham Sağlık Proilinin Kullanımı” Fizik. Tıp Rehabil. Derg. XXII.3, 110- 117. |
| [18] | Murat, S. (2007). Trakya Üniversitesi Tıp Fakültesi Fiziksel Tıp Ve Rehabilitasyon Anabilim Dalı, Lomber Traksiyonun Subakut Lomber Disk Hernili Hastalarda Klinik Ve Fonksiyonel Durum Üzerine Etkisi, Uzmanlık Tezi, s. 60. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML