-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2018; 8(4): 128-135
doi:10.5923/j.sports.20180804.04

Different Load Distributions Affect Acute Neuromuscular Responses and Muscle Thickness in Resistance-Trained Men
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLEnrico Gori Soares1, 2, Charles Ricardo Lopes1, 3, Gustavo Zorzi Fioravanti1, Felipe Alves Brigatto1, Willy Andrade Gomes2, Josinaldo Jarbas da Silva2, Lee E. Brown4, Paulo Henrique Marchetti5
1Department of Human Movement Sciences, Methodist University of Piracicaba, SP, Brazil
2Research Group on Neuromechanics of the Resistance Training, Nove de Julho University, SP, Brazil
3Adventist Faculty of Hortolandia, Hortolandia, SP, Brazil
4Department of Kinesiology, California State University, Fullerton, CA, USA
5Department of Kinesiology, California State University, Northridge, CA, USA
Correspondence to: Paulo Henrique Marchetti, Department of Kinesiology, California State University, Northridge, CA, USA.
| Email: |  |
Copyright © 2018 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of the present study was to compare acute neuromuscular responses and muscle thickness of a resistance training session with continuous- vs. grouped-sets. The experimental procedures were performed across three sessions in a crossover and random fashion. During the first session, all subjects were familiarized and the 10RM load was determined for both exercises: biceps curl (BC) and triceps extension (TE). The following two sessions were randomized for continuous- or grouped-sets. For continuous-sets, 8 sets of 10RM for each exercise (BC and TE) were performed sequentially, while for grouped-sets, each exercise was alternated every 4 sets until 8 sets of 10RM for each exercise were completed. Two minutes of rest was used between sets and exercises. Volume load and muscle thickness (biceps brachii, MTBB, and triceps brachii, MTTB) were measured pre- and post-exercise. Peak force and myoelectric activity (iEMG) were measured for each exercise (BC and TE) and each muscle (biceps brachii and triceps brachii) during a maximal voluntary isometric contraction test. Results demonstrated that volume load was significantly greater in grouped-sets for both exercises (P<0.001). MTBB and MTTB increased after both sessions (P<0.001), however, there was a greater effect with continuous-sets when compared to grouped-sets (P=0.001). Peak force decreased for both exercises and sets (P<0.05). iEMG decreased only after continuous-sets for both muscles (P<0.001). In conclusion, continuous- and grouped-sets resulted in specific neuromuscular responses and similar muscle thickness for prime movers. Continuous-sets decreased peak force, volume load, and muscle activity, and increased muscle thickness, while grouped-sets decreased peak force and maintained a high volume load.
Keywords: Neuromuscular fatigue, Muscle edema, Strength
Cite this paper: Enrico Gori Soares, Charles Ricardo Lopes, Gustavo Zorzi Fioravanti, Felipe Alves Brigatto, Willy Andrade Gomes, Josinaldo Jarbas da Silva, Lee E. Brown, Paulo Henrique Marchetti, Different Load Distributions Affect Acute Neuromuscular Responses and Muscle Thickness in Resistance-Trained Men, International Journal of Sports Science, Vol. 8 No. 4, 2018, pp. 128-135. doi: 10.5923/j.sports.20180804.04.
1. Introduction
- The training division of muscle groups on different days is characterized by split routines. It is a common strategy used by experienced lifters in resistance training programs (RT) designed to reach different goals such as hypertrophy or strength. Split routines are utilized to increase volume load, incorporate more exercises per muscle group, and increase variability in RT sessions. In this way, each session may be more efficient [17, 18, 25]. Some studies have shown that RT to concentric muscular failure is required for maximizing exercise-induced muscle hypertrophy [32]. In order to avoid high levels of neuromuscular fatigue and maintain a high volume load during all sessions (per muscle group), several methods can be proposed to manipulate load and sets (i.e. superset, compound sets, etc.) [27]. These methods are based on increasing rest between sets, changing the exercise order or muscle groups [23]. A method called continuous-sets is common in RT programs, and consists of performing all sets of each exercise sequentially with a fixed rest interval. According to previous research, performing continuous-sets may alter muscle activation [7], level of neuromuscular fatigue [16], or transient muscle swelling in prime movers [24]. However, performing multiple sets continuously to muscle failure decreases the number of repetitions and volume load. Both methods are commonly used in RT programs, however, to the best of our knowledge there are no studies comparing these different methods in RT sessions. Therefore, the purpose of this study was to compare the acute neuromuscular responses and muscle thickness in two different RT sessions with continuous- or grouped-sets. It was hypothesized that both distributions would promote a reduction in muscle activity and increase in muscle thickness due to muscular failure, but grouped-sets would promote greater volume load and peak force compared to continuous-sets based on longer rest intervals between blocks of sets.
2. Methods
- SubjectsThe sample size was justified by an a-priori power analysis (G*Power) based on a pilot study where the peak force on a maximal voluntary isometric contraction (MVIC) was assessed as the outcome measure with an effect size of 0.75, an alpha level of 0.05, and a power (1−𝛽) of 0.80 [6]. Sixteen physically active participants volunteered for this study (age 27 ± 6 years, total body mass 81.8 ± 7.8 kg, height 174 ± 5cm, BC 10RM 61 ± 11 kg, and TE 10RM 70 ± 12 kg). All subjects were regularly engaged in RT for more than one year (at least 3 times a week), and familiar with standing biceps curl (BC) and triceps extension (TE) exercises. They had 3±1 years of experience in hypertrophy-type RT, no previous surgery or history of injury with residual symptoms (pain) in the upper limbs within the last year. The University research ethics committee approved this study (#67/2016), and all subjects read and signed an approved informed consent document.ProceduresSubjects were instructed not to perform any RT for 48 hours prior to each of three testing sessions. All tests were randomized and counterbalanced across subjects for exercise order, and distributions. In the first session, upper limb dominance and anthropometric measures were taken. All subjects were right-arm dominant based on their preferred arm to write. Then, subjects were instructed in the proper technique for the BC and TE. For BC, all subjects were positioned standing in front of a cable-pulley machine and were instructed to use a supinated grip on a straight bar. They lifted the weight stack from complete elbow extension to complete elbow flexion (concentric phase), then returned to full elbow extension (eccentric phase). For TE, they were positioned standing in front of a cable-pulley machine and were instructed to use a pronated grip on the same bar. They lowered the weight stack from complete elbow extension to complete elbow flexion (eccentric phase) then returned to full elbow extension (concentric phase). All subjects underwent 10RM testing (according to guidelines established by the National Strength and Conditioning Association [NSCA] [4]) to determine individual initial training loads for each exercise, and the cadency was self-selected. Three to five minutes rest were used between attempts and 30 minutes between exercises. For both exercises BC and TE, no trunk movement was allowed during the repetitions and partial repetitions were not counted by the researchers.Two sessions were randomly assigned for each subject, exercise order, and distribution (Figure 1). Initially, a pre-test was conducted with measurements of muscle thickness from biceps brachii (MTBB) and triceps brachii (MTTB) via ultrasound. Sequentially, all subjects performed three trials of five-second MVICs for both exercises with elbows positioned at 90º, with 10-sec rest between trials. During MVICs, data were collected via a load cell and surface electromyography (sEMG) from elbow flexors (biceps brachii) and elbow extensors (lateral head of triceps brachii).
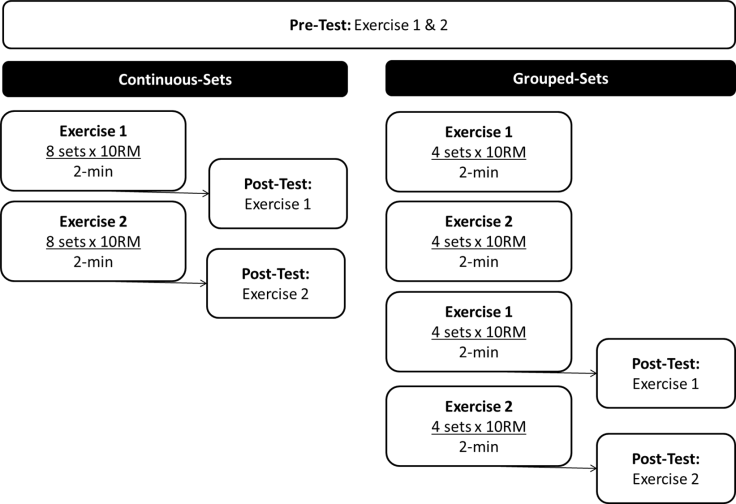 | Figure 1. Design of the experimental procedures |
3. Results
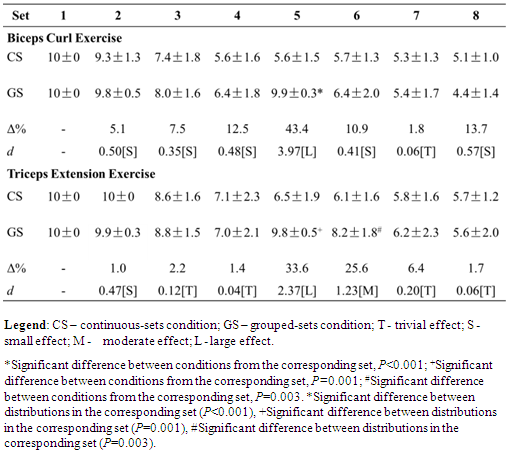
- Maximal Number of repetitions: There was a progressive reduction in the maximal number of repetitions performed during continuous-sets (P<0.05; d=0.96 [small effect]; Δ%=49%). However, for grouped-sets, there was a progressive reduction in the maximal number of repetitions performed from the 1st to the 4th set (P<0.05; d=0.81 [small effect]; Δ%=36%), and from the 5th to the 8th set, with no difference between 1st and 5th set (P<0.05; d=0.93 [small effect]; Δ%=55.6%) (Table 1).
|
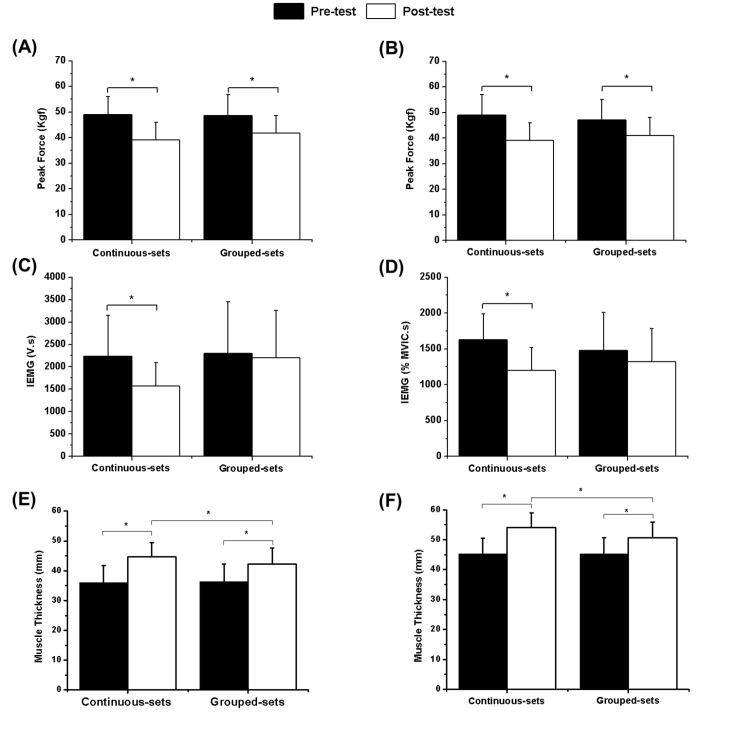 | Figure 2. Mean ± standard deviation of peak force performed on (A) biceps curl exercise, and (B) triceps extension exercise; muscle activity of the (C) biceps brachii, and (D) triceps brachii; and muscle thickness of the (E) biceps brachii and (F) triceps brachii for all experimental conditions.*Significant difference, P<0.05 |
4. Discussion
- The current study aimed to compare acute neuromuscular responses and muscle thickness between two different RT sessions with continuous- or grouped-sets. The findings were that acute neuromuscular responses and muscle thickness increased significantly between continuous- and grouped-sets in a single RT session. The results of the present study are partially in accordance with the main hypotheses. Continuous- and grouped-sets demonstrated similar reductions in peak force after a single RT session. Continuous-sets presented a reduction in the maximal number of repetitions and volume load when compared to grouped-sets. Muscle activity was reduced only after continuous-sets. Finally, muscle thickness was greater after continuous-sets versus grouped-sets. Several studies have demonstrated a progressive decrease in the maximal number of repetitions with continuous-sets, even with long rest intervals between sets and exercises [19, 26, 35, 36]. Willardson and Burkett [36], Scudese et al., [26], and Ratamess et al., [19] reported a reduction in the maximal number of repetitions performed during the bench press exercise (80%1RM, 3RM, and estimated 10RM, respectively) from 2nd to 5th set with 2 minutes rest between sets. In general, reduction in the maximal number of repetitions was observed in previous studies with similar results (continuous-sets: 49%, and grouped-sets: 43%). However, based on characteristics of grouped-sets, a higher volume load was observed (~10%,) when training was divided into two moments (4sets+4sets), and separated by longer recovery times. This result is in accordance with previous studies that demonstrated a time-efficient strategy with the use of alternate exercises aiming to sustain the maximal number of repetitions over multiple sets [13, 14, 16, 21]. It is well accepted that a combination of central and peripheral fatigue is responsible for the reduction in strength over multiple sets [3], and the rest interval is the main acute variable responsible for removing its deleterious effects [33, 34]. Previous studies have indicated that an increase in the rest interval between sets promotes removal of byproducts from the glycolytic system, restores adenosine triphosphate and phosphocreatine, and increases intracellular pH [22, 33, 34]. Therefore, grouped-sets presented higher volume load when compared to continuous-sets, and maintenance of the maximal number of repetitions across multiple sets. Even with different effects of the recovery interval between conditions, peak force was reduced in both conditions because all sets reached muscular failure.Muscle activation (iEMG) of the biceps brachii and triceps brachii decreased after continuous-sets, and remained unchanged after grouped-sets. Previous studies have reported reductions [2] and maintenance [12, 15] of muscle activity after multiple sets. They are in agreement with the present study regarding continuous-sets, even with different load strategies and exercises (single-joint [11, 28], and multi-joint [29, 30]). McCaulley et al., [15] did not observe differences in IEMG after 4 sets of 10 repetitions at 75% of 1RM in the squat exercise. On the other hand, Ahtiainen et al., [2] reported a significant reduction in iEMG after 4 sets of 12RM of leg press, 2 sets of 12RM of squats, and 2 sets of 12RM of knee extensions. However, all these studies used continuous-sets, making it difficult to compare with the grouped-sets condition in the present study. In addition, the present study design (agonist/antagonist) may have contributed to stimulating reciprocal inhibition, and reducing muscle activation in both muscles and distributions. Results of the present study directly demonstrate characteristics of each condition. Grouped-sets allowed more time for recovery between groups of sets, while continuous-sets induced a higher level of neuromuscular fatigue, due to less recovery time between sets. Therefore, byproducts of glycolysis can directly impact excitation-contraction coupling and action potential velocity, or indirectly inhibit output from Type III (quimioceptors) and IV (mechanoreceptors and nociceptors) afferents [9, 31] primarily after maximal voluntary contractions. Therefore, training strategies that aim to achieve a high degree of neuromuscular fatigue and muscle damage could choose continuous-sets, based on reduced recovery intervals between sets [8]. In this way, grouped-sets allow greater recovery between blocks of sets enabling maintenance of the load across sets of a single session.In regards to muscle thickness, continuous-sets presented greater values for both muscles when compared to grouped-sets. Transient edema in specific muscles is maximized, particularly after exercises until muscle failure and continuous-sets [8, 10]. Therefore, muscle thickness (MT) can be considered as a potential marker for metabolic stress including metabolite accumulation and muscle damage [8]. Additionally, during muscle contraction, the veins and capillaries are compressed, while the arteries continue to deliver blood to the working muscles causing a flow of plasma into the muscle cells. Therefore, it is possible that the shorter rest intervals in continuous-sets caused muscle transient edema when compared to grouped-sets.We recognize that this study has some limitations. Firstly, the total time of each session could be useful to understand the metabolic effect of each distribution, however all subjects performed both conditions in similar times (Continuous-Sets:~38-min and Grouped-Sets:~42-min). Secondly, measurements of lactate removal, hormonal responses, and muscle damage could be useful to fully understand the differences between continuous and grouped-sets. Finally, the present study design may have affected the results between distributions. However, the main idea was to evaluate and report acute differences between distributions in order to allow professionals to choose the best option for specific situations. Also, the number of sets and intensity used was chosen to match the practices of recreationally trained individuals aiming to increase hypertrophy. Therefore, the results of the present study cannot be generalized to other population or training goals.
5. Conclusions
- In conclusion, acute neuromuscular responses and muscle edema differed significantly when the sets of a single RT session were distributed differently (continuous- or grouped-sets). Continuous-sets resulted in a reduction in peak force, maximal number of repetitions, volume load, and muscle activity, but had the greatest increase in transient edema. On the other hand, grouped-sets showed a similar reduction in peak force but allowed greater volume load, and maintained muscle activity.