-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2018; 8(2): 55-62
doi:10.5923/j.sports.20180802.03

Influence of Gender and Different Sporting Disciplines on Cardiac Adaptation in Highly Trained Black Cameroonian Athletes
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNgongang OC 1, 2, Tsambang L 3, Azabji KM 2, Eyoungou LR 4, Mbou S 4, Chendjou KLO 5, Bitchou M 1, Wandji J 1, Jonte P 1, Tachim K 3, Kuate-Mfeukeu L 2, Mekoulou J 6, Nganou CN 1, Hamadou 1, Boombhi J 1, Ndongo AS 1, 2, 3, Kenfack M 1, 3, Essono A 3, Kaze FJ 1, Ouankou MD 7, Kingue S 2, Ngu BK 2, Mandengue HS 6
1Internal Medicine and Specialities - Yaounde University Hospital Center, Cameroon
2Faculty of Medicine and Biomedical Sciences - University of Yaounde I, Cameroon
3Higher Institute of Medical Technology Nkolondom Yaounde, Cameroon
4National Institute of Youth and Sport Yaounde, Cameroon
5Université Des Montagnes: Institut Supérieur des Sciences de la Santé (ISSS), Cameroon
6Douala University: Faculty of Sciences, Cameroon
7Centre de Cardiologie et Médical, Cameroon
Correspondence to: Ngongang OC , Internal Medicine and Specialities - Yaounde University Hospital Center, Cameroon.
| Email: |  |
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

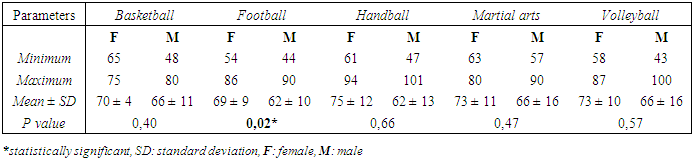
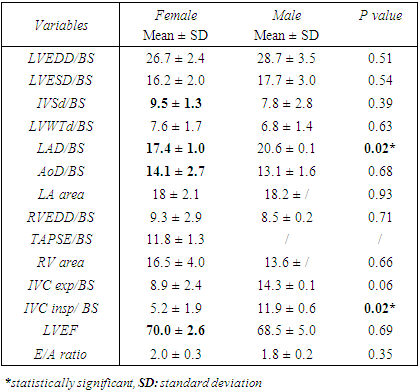
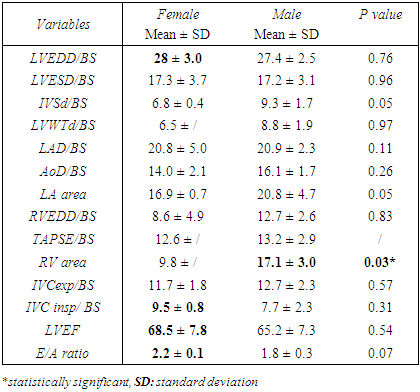
Background: Features of cardiac adaptation with practice of intense regular physical activities are described in athletes, but little focus is carried on the particular differences female athletes present as compared to male athletes especially in black African. Our study focused in bringing out the differences in Cameroonian athletes. Methods and Results: We enrolled 151 participants, 56.95% male and 43.05% female athletes for a male to female ratio of 1.3:1 and a mean age 25.87±3.33 years. Participants were professionally trained athletes, aging from 20 to 35 years and with at least one year of high intensity practice of physical activity. Sporting disciplines comprised Basketball, Football, Handball, Martial arts and Volleyball. We excluded pregnant or breast feeding women and subjects with cardiovascular diseases. The study was conducted at the National Institute of Youth and Sports. Ethical clearance and research authorization were obtained. Data collected from consenting participants was compiled using CSPro version 6.0 and the statistical analysis done with SPSS version 20 and Microsoft Excel 2010. The Chi square test for comparison of proportions, the ANOVA test (analysis of variance) and student test for comparison of means. Statistical significance was set at p = 0.05. Female (75.4%) and male (83.7%) athletes trained over 10 hours weekly. Mean anthropometric parameters were greater for men compared to women respectively, with Body weight (Kg) of 73.5± 11.7 against 67.6±13.3 (p=0.005); Body surface area (m2) of 1.87±0.18 against 1.73± 0.20 (<0.001) and BMI (Kg/m2) of 24.40±2.70 against 24.27±3.72. Left ventricular hypertrophy (LVH) were recorded in male athletes, with 28.6% from Basketball; 34.8% from Football; 61.5% from Martial arts; 12.5% from Volleyball and from Handball was noted 25% men versus 8.7% women with LVH. The mean heart rate (beats/ minute) was slower in men throughout the different sporting disciplines, with 66±11 versus 70±4 from Basketball; 62±13 versus 75±12 from Handball; 66±16 versus 73±11 from Martial arts; 66±16 versus 73±10 from Volleyball and 62±10 versus 69±9 from Football (p=0.02). Most male and female athletes were respectively in regular sinus rhythm. Accounting for 85.7% against 80% from Basketball; 71.1% against 94.7% from Football; 83.3% against 56.5% from Handball; 84.6% against 87.5% from Martial arts and 100% against 70% from Volleyball. Comparing echocardiographic parameters adjusted to body surface area between female and male athletes showed greater dimensions for men with some statistically significant. This statistically parameters were LAD/BS with 17±1.0 for women against 20.6±0.1 for men (p=0.02) and IVC insp/BS with 5.2±1.9 for women against 11.9±0.6 for men (p=0.02) from the Basketball discipline and RV area was 9.8 for women against 17.1±3.0 for men (p=0.03) in the Football discipline. Conclusion: This study has enabled to have precisions on the Athletes heart syndrome. The striking particularity exhibited by Black athletes show no gender particularity in our study population. Clear differences were demonstrated between male and female athletes, with more pronounced adaptation changes being exhibited by male athletes.
Keywords: Athlete’s heart syndrome, Gender, Sporting discipline, Cameroon
Cite this paper: Ngongang OC , Tsambang L , Azabji KM , Eyoungou LR , Mbou S , Chendjou KLO , Bitchou M , Wandji J , Jonte P , Tachim K , Kuate-Mfeukeu L , Mekoulou J , Nganou CN , Hamadou , Boombhi J , Ndongo AS , Kenfack M , Essono A , Kaze FJ , Ouankou MD , Kingue S , Ngu BK , Mandengue HS , Influence of Gender and Different Sporting Disciplines on Cardiac Adaptation in Highly Trained Black Cameroonian Athletes, International Journal of Sports Science, Vol. 8 No. 2, 2018, pp. 55-62. doi: 10.5923/j.sports.20180802.03.
Article Outline
1. Introduction
- The science on cardiovascular adaptations to exercise conditioning has expanded considerably with the improvement in examinations technics, through the use of electrocardiography (ECG), holter monitoring, echocardiography, cardiac magnetic resonance imaging and even invasive electrophysiological studies [1]. The graded benefit of exercise on cardiovascular health and mortality has been recognized and demonstrated in several observational and cohort studies [2]. Influential factors such as: age, gender, ethnicity and sporting discipline have shown substantial impact on the magnitude of cardiac adaptation [3-7]. Studies carried brought up evidences of differences in cardiac adaptation. Men exhibiting greater increases in cardiac dimensions compared to women practicing intense physical activity [5, 8]. The extent of left ventricular adaptation is influenced by the type of sporting discipline, with the most marked increases in cavity dimensions encountered in athletes engaging in endurance trained sporting disciplines [8-11]. Although, black athletes are known to exhibit particular striking repolarisation abnormalities and left ventricular hypertrophy when compared to Caucasian athletes which may be regarded as an ethnic variant of the athlete’s heart [12, 6, 7], the particular differences in cardiac adaption in the Black population between female compared male athletes in their individual sporting disciplines have been little documented worldwide. There is no focus on black African athletes and on Cameroonian athletes most specially. In this study we improve the knowledge on particularities exhibited by black African female compared to black African male athletes to prevent the globalization of the athlete’s heart adaptation.
2. Materials and Methods
2.1. Study Design and Population
- We carried out a descriptive cross sectional study on athletes from the National Institute of Youth and Sport (NIYS) at Yaounde, over a period 6 months from the 15th of January to the 20th of June 2017. We prospectively recruited after informed consent, professionally trained athletes aged from 20 to 35 years of both genders registered in the different sporting disciplines and practicing high intensity regular physical activity of at least a year duration at high level. Were excluded from the study all athletes who did not consent to participate, those with past history of cardiovascular diseases and pregnant or breast feeding athletes. We carried out a non-exhaustive consecutive sampling, targeting a minimum of 10 athletes per gender and from a minimum of 5 sporting disciplines.
2.2. Study Procedure
- A questionnaire was administered to everyone who concern to participate. Questions on their: age, gender, sporting discipline, duration of training per week and numbers of years of training. Then performance and endurance were evaluated by the Ruffier-Dickson test, which help exclude poorly trained athletes. Then, clinical and para-clinical data collected. - Measurement of weight: The participants climbed on a digital weighing scale (Omron HN289) with a layer of clothing and their corresponding weight recorded.- Measurement of height: The participants stood up erect and looked straight ahead with their back against the board. Then the movable headpiece of a mounted height rod was brought onto the uppermost point and the corresponding height was noted.- Measurement of blood pressure: The participant was admitted to rest for about 10 minutes. We used a calibrated electronic oscillomeric device (Boso-medicus uno). With a correct cuff size placed at heart level and 2cm above the elbow, we measured the Blood pressure at right arm three times and the average recorded [13, 14]. - Cardiac auscultation: The participant in a calm quite examination room had a physical examination. After inspection and palpation, auscultation was done with a Littman classic M3. Low pitch heart sounds S3 and S4 were researched using the bell of the stethoscope, with the participant lying.- An electrocardiographic tracing: a 12 leads standard ECG using MEDICAL ECONET Cardio M Plus was recorded for each participant after they observed a 5 minutes rest. Indexed data to common training-related ECG changes such as Sinus bradycardia, first-degree atrio-ventricular block, incomplete right bundle branch block, isolated QRS voltage criteria for LVH and to uncommon training-related ECG changes such as T-wave inversion, ST-segment depression, left atrial enlargement, left axis deviation/left anterior hemiblock, right axis deviation/left posterior hemiblock, Ventricular premature contractions, complete left or right bundle branch block [15-17]. - A Doppler echocardiography assessment: all echocardiography assessments were done by the same cardiologist (C.N.O) using ESAOTE TM Mylab 30CV and Cardiac Probe PA 240/2.5GHz. Indexed data were morphologically: LVEDD/BS, LVESD/BS, IVSd/BS, LVWTd/BS, LAD/BS, AoD/BS, LA area, RVEDD/BS, RV area, IVC exp/BS, IVC insp/ BS and functionally: TAPSE/BS, LVEF and E/A ratio [1, 12].
2.3. Data Management
- All the filled questionnaires were verified and validated on the field. The data entry sheet was developed using CSPro version 6.0. The data was double-entered, compared, cleaned and analyzed using SPSS version 20 and Microsoft Excel 2010. Quantitative variables are expressed as mean ± standard deviation. Meanwhile, qualitative variables were expressed as effective and percentages. The Chi square test for comparison of proportions, the ANOVA test (analysis of variance) and student test for comparison of means. Statistical significance was set for P value less than 0.05.
2.4. Ethical Consideration
- Ethical clearance was obtained from the Douala University Institutional Ethic Committee to carry out this study. The study procedure was explained to each participant before they were given the opportunity to sign a written consent form. They had the right to withdraw from the study at any point in time without prejudice. All the information obtained or used in the study was treated as confidential.
3. Results
3.1. General Characterization of the Study Population
3.1.1. Demographic Characterization
- A total of 200 athletes were contacted of both genders from different sporting disciplines, but were included 151 athletes. There were 86 (56.95%) male and 65 (43.05%) female athletes, for a male to female sex ratio of 1.3:1. Most participants were aged below 30 years, with the highest number between 25 to 29 years consisting of 29 (44.61%) of female and 42 (48.84%) of the male participants. It was followed by those from 20 to 24 years, with 26 (40%) female and 33 (38.37%) male athletes. Whereas, the least represented age group was that from 30 to 35 years with 10 (15.39%) female and 11 (12.79%) male participants. The mean age for the study population was 25.87±3.33 years. The sporting disciplines involved were Basketball, Football, Handball, Martial arts and Volleyball. The highest number of female participants was from the Handball discipline, with 23 (15.23%) athletes and the least represented was from the Basketball discipline with 5 (3.31%) athletes. For male participants, the most represented was from the Football discipline, with 46 (30.46%) athletes and the least represented was Basketball with 7 (4.64%) athletes. The overall most represented sporting discipline was Football (43.05%) and the least represented was Basketball (7.95%). As show in figure 1 below:
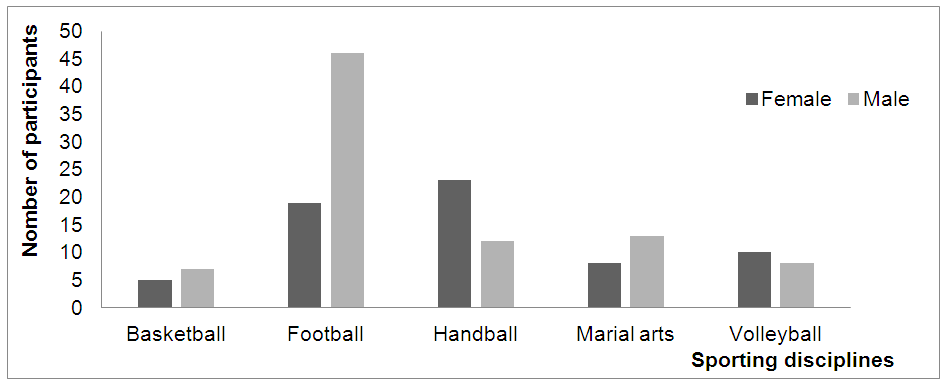 | Figure 1. Genders distribution in sporting disciplines |
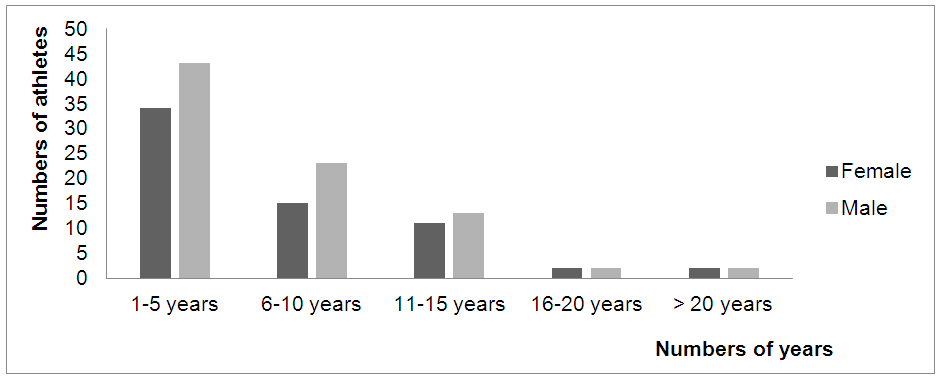 | Figure 2. Distribution of training duration with respect to gender |
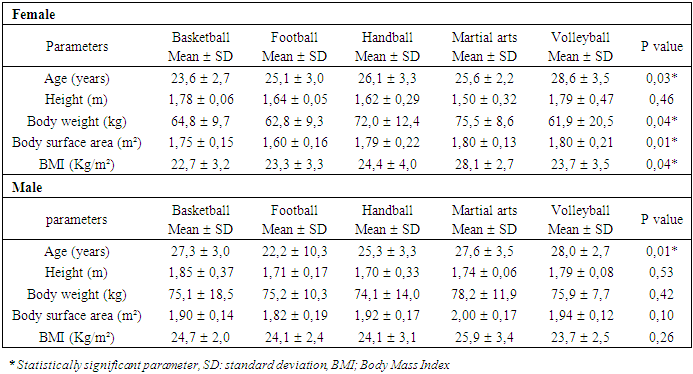
3.1.2. Anthropometric Parameters from Different Sporting Disciplines
- From the female population, was noted in Volleyball the highest height (p=0.46); from Martial arts the highest body weight (p=0.04), body surface area (p=0.01) and BMI (p=0.04). From the male population was noted in Basketball the highest height and highest body weight; from Martial arts the highest body surface area and BMI. All were statistically not significant. Results shown in table 1 below:
|
3.2. Paraclinical Pattern of the Study Population
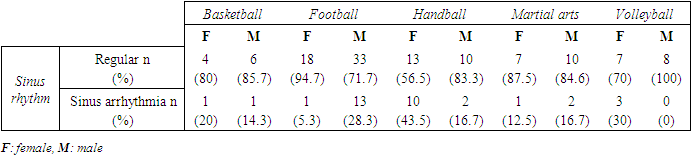
3.2.1. Electrocardiographic Parameters
- I) Rhythm disturbances
|
|
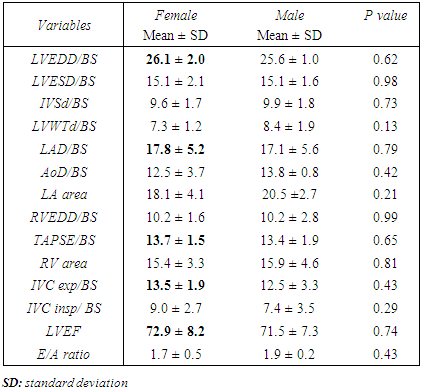
3.2.2. Transthoracic Echocardiography Pattern
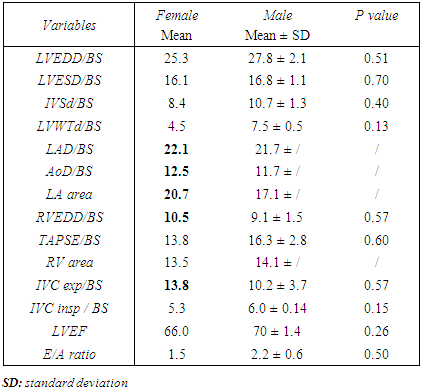
- I) Cardiac morphological and functional pattern with respect to genders in same sporting discipline a) Cardiac morphological and functional differences in Basketball
|
|
|
|
|
4. Discussion
4.1. Characteristics of the Study Population
4.1.1. Demographic Characteristics
- Our study enrolled 151 athletes from both genders and sporting disciplines. The male athletes represented 56.95% and female athletes 43.05% of the study population. The mean age was 25.87±3.33 and ranging from 20 to 35 years. This differs from results reported by documented studies carried in sporting population. Most studies recruited participants through advertisements and flyers distributed at the training sites [18]. Also differ from results of studies carried in sporting institutions, as that from Pellicia A and al, who recorded 78% male and 22% female athletes, with a mean age of 22 years [17] and from Maron B and al who recorded a mean age of 24 years. In these studies the participants were all training for Olympic competitions with consequent age restriction and specific training regimes [19]. Whereas, our study carried on subjects from a university sporting institution and had a lesser degree of age restrictions and had generalised training regimes. Most of our participants trained over 10 hours weekly. These accounted for 75.4% and 83.7% of the female and male study population respectively. The minimal duration of practice was set above on year. This greatly corresponds to the athlete’s definition by most literatures [20, 21, 22].
4.1.2. Anthropometric Characteristics
- Statistically significant differences were obtained for most of the anthropometric (body weight and body surface area) between genders, which were more, pronounce for male athletes. These results are similar to those found by Brunkhorst L et al in their study on 93 volunteer of both genders and from two sporting disciplines (cyclists and triathletes). They evaluated eight different anthropometric parameters and demonstrated male athletes had more pronounced parameters than female athletes in both groups [23]. We could not associate the differences in anthropometric to the impact of their weekly training hours or duration in training. Since, athletes from both gender had almost similar training sessions. Hence the dissimilarities can mainly be due to genetic differences and was not predictive of their resultant performances.
4.2. Para-clinical Comparison of between Gender from Same Sporting Disciplines
4.2.1. Electrocardiographic Differences
- In all the sporting disciplines left ventricular hypertrophy mainly concerned male athletes. No significant differences were noted in the type of heart rhythm exhibited from both female and male athletes in each sporting discipline. Most athletes were in regular sinus rhythm. Slowest heart rates (bradycardia) were more expressed by male athletes in each sporting disciplines. Atrio-ventricular conduction was normal for both genders in all the sporting disciplines except for Football where a first degree atrio-ventricular block was noted in both a female and a male athlete. Abnormal repolarisation patterns were recorded for 62 (95.4%) female and 81 (94.2%) male athletes. These correlate to results obtained by Wilhelm M et al [24] in which the prevalence of ECG abnormalities were higher in male than in female athletes respectively (12.4 vs. 9.6%). Also similar to Pelliccia A et al study which resulted from the evaluation of 1005 athletes of the Italian National Olympic Committee and showed a male predominance in ECG abnormalities [5]. Male athletes expressed more related sport induce electrocardiographic alterations. There were no striking differences except for left ventricular hypertrophy.
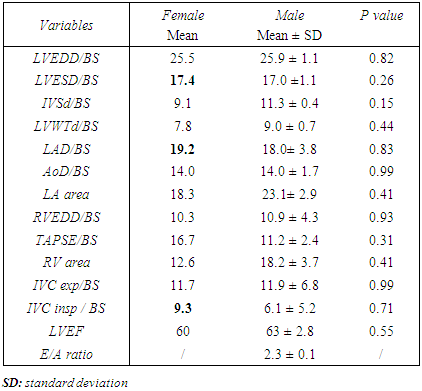
4.2.2. Echocardiographic Differences
- Echocardiographic parameters compared between genders in same sporting disciplines showed higher dimensions for male athletes. These parameters were adjusted to body surface area, to exclude its impact on the magnitude of cardiac dimensions. Exception noted for LAD/BS and LVEF, which were generally greater in female athletes from various sporting disciplines. This is similar to the results obtained by Dilek C et al 2013 in Turkey, were left ventricular end diastolic diameter sizes, left ventricular mass index were higher for male athletes and LADin (left atrial dimension index, unit in cm/m2) were higher in female as in our study [25]. These also correlated to some extend to results of a previous study by Wernstedt C et al which reported that left ventricular mass index were higher in male than female athletes practising endurance training [26]. This male predominance in left ventricular dimension can be a result of a difference in aerobic work capacity and genetic influence. The hormonal influence can also be associated to this variation, with regard to the study by Pavlik G and al [27].
5. Conclusions
- This study on clinical and para-clinical features of 151 highly trained Cameroonian athletes of both genders and from different sporting disciplines showed clear cardiac adaptation features. The striking particularity exhibited by Black athletes as compared to Caucasian athletes was not demonstrated to be specific for a particular gender in our Black population. Nevertheless, there were cardiac adaptation differences between female and male athletes. Black male have more pronounce adaptation changes than Black female athletes.
Future Directions
- Although understanding of the athlete’s heart syndrome is considerably progressing with increasing focus on the Black population, several unanswered questions remain. We believe that from a descriptive and physiologic perspectives, several issues deserve future study. Firstly, the clear impact of genetic and environmental factors which remains poorly understood in Black athletes. Secondly, further studies to compare electrocardiographic patterns with echocardiographic parameters of cardiac morphology. It will be of great interest to conduct a study with such objective in our population. Thirdly, a similar study can be carried in a larger population of athletes and not limited to a university institution but, opened to all sporting institutions.