-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2017; 7(3): 122-127
doi:10.5923/j.sports.20170703.05

The Effects of Kettlebell Mass and Swing Cadence on Heart Rate, Blood Lactate, and Rating of Perceived Exertion during an Interval Training Protocol
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLCorey Wesley, Derek Kivi
School of Kinesiology, Lakehead University Thunder Bay, Canada
Correspondence to: Corey Wesley, School of Kinesiology, Lakehead University Thunder Bay, Canada.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The purpose of this study was to determine the effects of kettlebell mass and swing cadence on heart rate, blood lactate, and rating of perceived exertion (RPE) during an interval kettlebell swing protocol in experienced female kettlebell users. Eighteen female participants completed three 5-minute rounds of a 15-second on, 15-second off interval kettlebell swing protocol using an 8, 12 and 16 kg kettlebell during three separate testing sessions. Each testing session used a cadence of 8, 10 or 12 swings per 15 second interval (SPI15). Mean values for heart rate, blood lactate, and RPE were measured for each 5-minute round of each testing session. The results of the repeated measures analysis of variance revealed no significant interaction effects were found between kettlebell mass and swing cadence for heart rate or RPE, but a significant interaction effect was found for blood lactate (F (4, 68) = 6.621, p < 0.001). Significant main effects were found for both kettlebell mass and swing cadence for heart rate (F (2, 34) = 97.302, p < 0.05), blood lactate (F (2, 34) = 33.273, p < 0.05), and RPE (F (2, 34) = 118.300, p < 0.05). The results revealed that the kettlebell swing, regardless of kettlebell mass or swing cadence, provided a level of intensity that was sufficient to increase aerobic capacity. The results suggest that various combinations of kettlebell masses and swing cadences can be utilized and implemented into a strength and conditioning program.
Keywords: Kettlebell, Mass, Cadence, Interval training, Aerobic capacity
Cite this paper: Corey Wesley, Derek Kivi, The Effects of Kettlebell Mass and Swing Cadence on Heart Rate, Blood Lactate, and Rating of Perceived Exertion during an Interval Training Protocol, International Journal of Sports Science, Vol. 7 No. 3, 2017, pp. 122-127. doi: 10.5923/j.sports.20170703.05.
Article Outline
1. Introduction
- Since the turn of the millennium, the kettlebell has seen a widespread re-emergence amongst athletes, strength coaches and fitness enthusiasts. A centuries old tool, a kettlebell is a sphere shaped cast iron weight that resembles a cannonball with a handle. Kettlebell training emphasizes increasing rate of force production through ballistic full body movements with submaximal loads [18]. Although previous research has demonstrated significant increases in endurance, strength, and power through training [14, 15], findings on the kettlebell’s utility for cardio-respiratory adaptations are unclear or controversial, as heart rates achieved during kettlebell exercise are consistently higher than the corresponding oxygen uptake demands [5, 11]. The two arm kettlebell swing is a compound cyclical ipsilateral hip hinge movement performed explosively. The user assumes a hip hinge posture with the kettlebell anterior to the toes and grasps the kettlebell handle with both hands and projects the kettlebell back between the legs (Figure 1A). Once the hips are loaded, the user explosively extends the hips while projecting the kettlebell forward until the body forms a straight line from ear to ankle and the kettlebell and arms form a horizontal line at eye level (Figure 1B). The kettlebell is then projected back between the legs and the movement is repeated. The swing consists of cycles of rapid force production and relaxation. EMG analysis has shown that the posterior chain muscles cycle between 100% activation to almost complete relaxation [16]. The relaxation portion of the swing may act as a mechanism for clearing metabolic by-products faster; reducing the inhibiting effects of anaerobic activities such as the swing [9, 11]. Due to an acute release of hormones involved in muscular adaptations during kettlebell swing exercise, the swing may be a great addition to traditional resistance training programs [1].
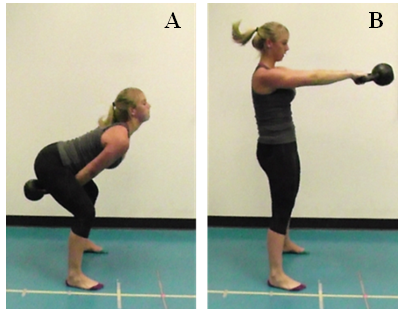 | Figure 1. The two arm kettlebell swing (A) hip hinge position and (B) top swing position |
2. Methods
2.1. Participants
- Eighteen female participants (Age = 30 ± 9.6 years, Height = 165.5 ± 7.4 cm, Mass = 68.2 ± 9.0 kg) were recruited from a local fitness facility that offers kettlebell classes conducted by a certified Russian Kettlebell Challenge (RKC) instructor. All participants were previously instructed in performing proper kettlebell swing technique with at least 6 months experience in kettlebell training under a certified kettlebell instructor. In order to maintain homogeneity and for convenience in sampling, only female participants were selected as a higher prevalence of potential participants in the kettlebell classes were female. Participants were screened by a Physical Activity Readiness Questionnaire (Par-Q) and a Movement Clearance Test [2] prior to their participation in the study. Ethical approval was received from the Lakehead University Research Ethics Board prior to data collection.
2.2. Testing Procedures
- Body mass (kg) was measured using a digital scale and height (cm) was taken using a wall mounted Tanita HealthOMeter height rod. Resting heart rate (bpm) and resting blood lactate (mmol/l) were measured at the beginning of each session after having the participant lie supine on the floor for 5 minutes [12] prior to the start of the testing protocol. To accurately determine percentage of heart rate maximum during testing protocols, age predicted maximal heart rate was estimated for each participant using the formula from Gellish et al. [9] [207 – (0.7 x age)]. A standardized 10-minute warm up was completed prior to testing, and involved a general warm up and a kettlebell specific joint mobility/dynamic stretching complex. The general warm up consisted of 5 minutes on a cycle ergometer at a resistance of 2% of body weight at 60 revolutions per minute paced by a metronome. The 5-minute kettlebell specific joint mobility/dynamic stretching warm up emphasized the major muscles groups and joints used while executing the kettlebell swing, including the muscles and joints of the neck, shoulders, elbows, wrists, back, abdominals, hips, hamstrings, quadriceps, knees and ankles. Following the general and specific warm up, in order to prepare for the cadence level used during the upcoming testing session, participants completed one 15 second swing interval at the specified cadence, using a 12 kg kettlebell. The participants were then given a 5-minute period before the testing protocol commenced.Each testing session consisted of 3 rounds of an interval kettlebell swing protocol, lasting 5 minutes each, with each round utilizing a different mass kettlebell. The mass of the kettlebell for each round was randomly 8, 12 and 16 kilograms. Each round involved 10 intervals of 15 seconds work, followed by 15 seconds of rest, utilizing the two arm kettlebell swing. The participants were then given a 10 minute active recovery between rounds and were encouraged to stay loose by walking around. The purpose of the 10 minute recovery was to ensure that the participant’s heart rate returned to resting levels before commencing the next round. The participant was required to swing the kettlebell with two hands back between the legs and concentrically accelerate it forward and up to chest level and back down between the legs. The number of kettlebell swing repetitions for each 15 second interval was paced to a metronome and randomly varied between each of the three testing sessions from 8 swings per 15 second interval (SPI15), 10 SPI15, or 12 SPI15. For each swing cadence, the metronome was set at 64 bpm (8 SPI15), 80 bpm (10 SPI15) and 96 bpm (12 SPI15), producing two beats per swing, one at the top swing and one at the bottom swing. The 15 second interval cadence (8, 10, and 12 SPI15) for each of the three testing sessions was determined by a pilot study prior to the initial data collection, which ensured that the participants could complete each stage of the protocol for each kettlebell mass. Throughout the testing protocol, heart rate was recorded at 15 and 45 seconds of each minute using a Polar RS400 Heart Rate Monitor and chest strap, with the peak heart rate measured being used for analysis. Immediately upon completion of each 5-minute round of the interval swing protocol, a rating of perceived exertion (RPE) was assessed using the 6-20 Ratings of Perceived Exertion Borg Scale. Lactate measurements were also taken at the end of each 5-minute round of the protocol from the participant’s fingertip using a Lactate Pro Portable Analyzer. The Lactate Pro Lactate Analyzer has been reported as accurate and reliable, and exhibits a high degree of agreement with other lactate analyzers [17].After completing the testing protocol, participants performed a cool down consisting of 3 minutes on the cycle ergometer and static stretching which focused on the major muscle groups emphasized during the kettlebell swing.
2.3. Statistical Analysis
- Descriptive statistics were used to compare means and standard deviations for heart rate, blood lactate, and RPE across the three kettlebell masses and cadences. A 3 mass (8, 12, 16 kg) x 3 cadence (8, 10, 12 SPI15) repeated measures analysis of variance was used to identify significant differences in heart rate, blood lactate, and RPE. Significant main effects were further analysed with Bonferroni adjusted pairwise comparisons. Statistical significance was set at the p < 0.05 level.
3. Results
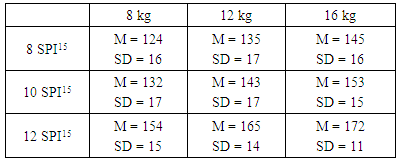
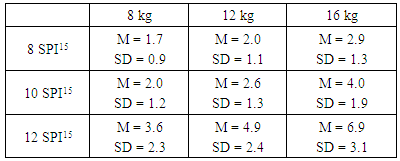
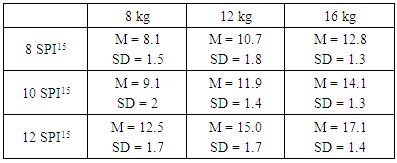
- Mean heart rate (bpm), lactate (mmol/l), and RPE are presented in Tables 1, 2, and 3, respectively. There was no interaction effect seen between kettlebell mass and swing cadence for heart rate (F (4, 68) = 1.122, p = 0.354). Similarly, there was no interaction between kettlebell mass and swing cadence on RPE (F (4, 68) = 0.316, p < 0.866). An interaction effect was found between kettlebell mass and swing cadence for blood lactate (F (4, 68) = 6.621, p < 0.001) (Figure 2). A significant main effect for kettlebell mass was found for heart rate (F (2, 34) = 145.287, p < 0.05), blood lactate (F (2, 34) = 63.008, p < 0.05), and RPE (F (2, 34) = 247.03, p < 0.05). Post hoc analysis showed that for each 4 kg increase in kettlebell mass, significant increases were seen in heart rate (p < 0.001), lactate (p < 0.001), and RPE (p < 0.001).A significant main effect was also found for each dependent variable as swing cadence increased (heart rate: F (2, 34) = 97.302, p < 0.05; blood lactate: F (2, 34) = 33.273, p < 0.05; and RPE: F (2, 34) = 118.300, p < 0.05. As with kettlebell mass, post hoc analysis found that each increase in swing cadence level significantly increased heart rate (p < 0.001), blood lactate (p < 0.001) and RPE (p < 0.001).
|
|
|
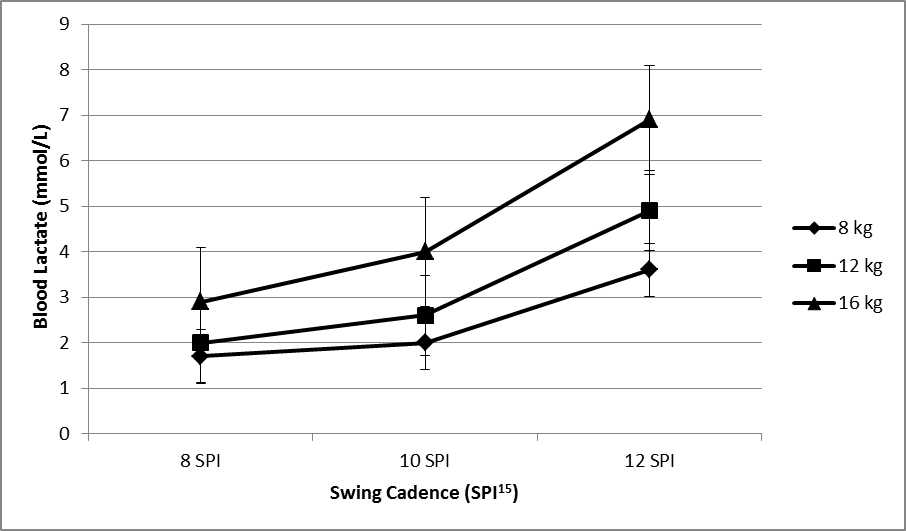 | Figure 2. Mean blood lactate values for each swing cadence and kettlebell mass |
4. Discussion
- This study examined the physiological responses and perceived intensity of the kettlebell swing during different mass and cadence levels to better understand this method of training. As kettlebells are traditionally manufactured in 4 kilogram increments, the results suggest that these increments are appropriate from a physiological perspective as heart rate, blood lactate, and RPE were found to increase significantly with each kettlebell mass used. For kettlebell users who are seeking to gradually increase cardiovascular intensity during subsequent training sessions, it may be recommended to implement 2 kg increases, progressively overloading the intensity level without drastically increasing in the physiological response. Regardless of mass or cadence used during this study, the two arm kettlebell swing was found achieve the minimum threshold for increasing aerobic capacity, which is consistent with other studies on the kettlebell swing [5, 8, 10]. Previous research, however, has indicated that the heart rates reached during kettlebell swing exercise are consistently higher than their oxygen uptake demands, questioning its utility as a tool for increasing cardiorespiratory fitness. Hulsey et al. [10], when comparing an interval kettlebell swing routine with treadmill running at equivalent RPE values (15.3 to 15.5), found no significant differences in heart rate; however, oxygen consumption and caloric expenditure were higher in treadmill running. Nonetheless, kettlebell swing bouts were performed above 85% of their maximum heart rate, thus eliciting a physiological response necessary for improving cardiorespiratory fitness. Thomas et al. [18] found that heart rate and RPE levels were higher during kettlebell exercise than moderate intensity treadmill exercise when oxygen consumption was equivalent. Therefore, previous research on kettlebell swing exercise suggests an adequate physiological response necessary for increasing cardiorespiratory fitness, however, perceived exertion and heart rate is higher during kettlebell exercise when compared to other modalities such as treadmill exercise when physiological responses are equal. The fact that the previous studies recruited novice kettlebell users as participants suggests that experience may be a factor in determining the perceived exertion during the kettlebell swing, as our participants were able to work at higher cadence levels and heart rate values before RPE reached the levels in the previous studies. This suggests that kettlebell swing exercises may be a great alternative for cardiorespiratory fitness when proper form is achieved through instruction and experience, with the added benefits of muscular strength, endurance, and power.Differences in kettlebell masses and swing cadences used among kettlebell research studies makes it difficult to directly compare the physiological responses observed. Duncan et al. [3] controlled kettlebell swing intensity and compared physiological responses at different kettlebell mass and swing cadence levels during a continuous kettlebell swing protocol. Participants swung a kettlebell for 2-4 minutes at a slow (20 swings per minute) and a fast (40 swings per minute) cadence, with a 4 and an 8 kg kettlebell. No significant differences were found in heart rate or blood lactate across mass and cadence variations; however, perceived exertion increased as mass increased. Because RPE was higher with the 8 kg kettlebell and no differences in the physiological response between masses, the authors suggested that training programs might be more effective when using a 4 kg load on the basis that it will feel more comfortable but elicit the same physiological response as an 8 kg load. One limitation with their study may been the load chosen to compare and the cadence levels, which were much lighter and slower than our procedures. Due to the pendulum-like motion of the kettlebell swing, slow cadence levels may be perceived as unnatural, as the dynamic swinging motion becomes a static resistive motion when the ballistic hip hinge is eliminated, resulting in a shoulder dominated exercise. This may have been the case during the 20 swings per minute in the Duncan et al. [3] study. This cadence would have been equivalent to 5 SPI15 in our study, and may have forced the user to resist the mass of the kettlebell during the relaxation phase of the tension/relaxation cycle of the swing. At 8 SPI15 (32 swings per minute), our participants reported that this swing cadence was unnaturally slow. To maintain this cadence, participants were either forced to (i) resist the kettlebell momentum during the backswing, (ii) hold the kettlebell up during the top swing, which was only possible with the 8 kg kettlebell, or (iii) make the kettlebell float higher during the top swing with the heavier kettlebells. As a result of this unnatural pace, the physiological variables may have been inflated. Nevertheless, this cadence produced a significantly lower metabolic response than the 10 and 12 SPI15 cadence levels, and based on these observations, a cadence lower than 32 swings per minute would not be recommended during kettlebell swing exercise.As swing cadence increased to 12 SPI15 (48 swings per minute), users were forced to actively pull the kettlebell down during the backswing in order to keep pace, emphasizing an ‘overspeed eccentric’ action during the backswing; this was not seen at the 8 or 10 SPI15 level. Because of the increased speed during the backswing, the stretch reflex of the posterior chain may have been initiated, as the force produced during the subsequent forward swing was visibly greater in the participants at the 12 SPI15 cadence. This increased pace resulted in significant increases in heart rate (14.7%), blood lactate (83%) and RPE (27%) from the 10 SPI15 to the 12 SPI15 cadence level, and noticeably higher than from 8 SPI15 to 10 SPI15 (5.9%, 32%, & 10% respectively). These increases are possibly due to the elimination of the relaxation phase (backswing) during the tension/relaxation cycle of the kettlebell swing, as the users were forced to pull the kettlebell down during the backswing to keep pace.Fung and Shore [8] suggested that aerobic threshold is not surpassed during kettlebell exercise when its mass is equal to or below 13% of body mass, placing the 8 kg kettlebell used in our study below this threshold. However, if aerobic threshold is estimated as occurring at a blood lactate level of 2 mmol/l [6, 13], then the 10 and 12 SPI15 cadences used with the 8 kg kettlebell produced lactate levels that were equal to or surpassed aerobic threshold. For all trials involving kettlebell masses above 8 kg and regardless of cadence, blood lactate levels were equal to or greater than 2 mmol/l. It was only at the 10 SPI15 cadence with the 10 kg mass and at the 10 and 12 SPI15 cadences with the 16 kg mass that anaerobic threshold of 4 mmol/l [6, 13] was reached. Blood lactate has been examined previously in kettlebell research involving various protocols. Budnar et al. [1] had 10 male participants swing a 16 kg for 12 rounds of 30 seconds work, 30 seconds rest at a cadence of 19 swings per interval, which approximates to our 10 SPI15 cadence level. Blood lactate reached 7 ± 3 mmol/l. Similarly, Duncan et al. [3] saw blood lactate range from 5.8 to 7.5 mmol/l during 2 to 4 minutes continuous swinging with 4 and 8 kg kettlebells. Comparable results have been reported previously with shorter duration, higher intensity intervals as well. Fortner et al. [7] saw blood lactate reach 6.4 ± 1.1 mmol/l during 8 rounds of 20 seconds work with 10 seconds rest. In their study, females used 4.5 kg kettlebells and males used 8 kg kettlebells, and were directed to swing as fast as possible. Our study utilized cadence levels above 40 swings per minute in a controlled, interval fashion, suggesting that faster cadence levels for shorter intervals can result in a physiological response which is comparable to long interval or continuous protocols.The results from this study suggest that different combinations of mass and cadence may be used during a two-handed interval kettlebell swing exercise protocol in order to produce the same physiological response. For example, kettlebell users who may lack the strength to swing the 16 kg kettlebell or who may be recovering from an injury may benefit by swinging a lighter mass kettlebell at faster cadences. Likewise, increasing the ability to swing heavier loads without increasing the physiological response can be done by increasing the mass and lowering the cadence speed. Furthermore, simply changing the mass and cadence combination on any given training session for variety can be accomplished while maintaining the desired training intensity. For example, the 16 kg kettlebell at 8 SPI15 elicited a heart rate response of 145 ± 16 bpm, whereas increasing the cadence to 10 SPI15 and decreasing the mass to 12 kg resulted in a similar response of 143 ± 17 bpm. When applied to sport-specific training, faster cadences with higher repetitions per interval can be implemented on dynamic-effort speed training days, whereas increases in mass combined with a slower cadence can be implemented during strength days, without comprising the metabolic response of the training session.
5. Conclusions
- This study examined the physiological responses and perceived intensity of the two arm kettlebell swing in experienced users. The results indicate that an interval training protocol provides a level of intensity that is sufficient to increase aerobic capacity. This information can be beneficial for individuals who participate in kettlebell training, as various combinations of swing cadences and masses can be effective in adding variety to training while achieving the desired physiological response.