-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2017; 7(3): 111-117
doi:10.5923/j.sports.20170703.03

Maximal Static and Dynamic Neck Strength in Hockey Players and Wrestlers
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMorgan Broennle, Derek Kivi, Carlos Zerpa
School of Kinesiology, Lakehead University Thunder Bay, Canada
Correspondence to: Derek Kivi, School of Kinesiology, Lakehead University Thunder Bay, Canada.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

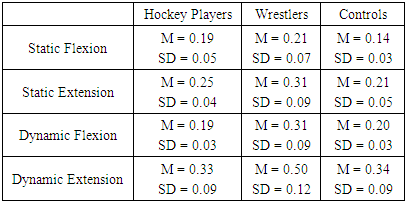
The purpose of this study was to compare maximal static and dynamic neck strength between hockey players and wrestlers. Athletes were recruited from the university men’s hockey and wrestling teams, with active male university students serving as a control group. Each group consisted of eight participants between the ages of eighteen and twenty-four. Anthropometric measurements, including height, mass, neck length, and neck girth were taken prior to testing. Static and dynamic cervical strength testing was completed using a modified Nautilus neck strengthening machine. Maximal static neck flexion and extension strength were measured using a load cell attached to the arm of the Nautilus machine, which was set in a neutral neck position. To measure dynamic neck strength, a 6-Repetition Max (RM) submaximal test was completed for cervical flexion and extension, from which 1-RM values were predicted. Mean normalized strength values were significantly higher among all participants for neck extension (M = .32, SD = .12) than for neck flexion (M = .20, SD = .07). Mean neck strength was significantly greater for dynamic muscle contractions (M = .31, SD = .13) than for static muscle contractions (M = .22, SD = .08). When comparing among groups, mean normalized static neck strength of the wrestlers was significantly greater than that of the hockey players in both the flexion and extension directions, with no differences seen between the hockey players and the controls. Differences in static and dynamic neck strength between hockey players and wrestlers are likely associated with the demands of each sport and their sport-specific strength training.
Keywords: Cervical musculature, Neck training, Cervical strength testing, Neck injury, Sport performance
Cite this paper: Morgan Broennle, Derek Kivi, Carlos Zerpa, Maximal Static and Dynamic Neck Strength in Hockey Players and Wrestlers, International Journal of Sports Science, Vol. 7 No. 3, 2017, pp. 111-117. doi: 10.5923/j.sports.20170703.03.
Article Outline
1. Introduction
- It has been recommended that athletes involved in contact sport incorporate strengthening exercises for the cervical musculature into their training programs in order to reduce the risk and severity of neck injuries and improve sport performance [7, 8, 22, 25, 27, 30]. According to Cross and Serenelli [8], a cervical strength training program for any athlete involved in contact sport should begin with static (isometric) exercise and progress to include dynamic workouts. Such training enhances the athlete’s ability to effectively stabilize the neck while developing proprioception and contractile force of the neck muscles [5]. This development is essential to minimizing neck injury as it can improve the speed and strength of muscular contractions, enabling the athlete to achieve appropriate neck tension at impact [12]. Additionally, cervical spine stability is important for maintaining proper posture for optimal performance [8]. Finally, cervical muscle hypertrophy from dynamic training may aid in the dissipation of energy from impact forces to the head [10]. Ice hockey and wrestling are two contact sports in which specific trends in neck injuries have been observed [2, 23, 26, 30]. The risk and severity of the neck injuries common to each sport, however, differ substantially due to considerable difference in the physical stress placed on the cervical muscles during sport action and in training. Research has shown that while there is an increased risk of catastrophic spine injury associated with ice hockey, overuse injuries to the cervical muscles and ligaments are much more prominent in wrestling [21]. To minimize these injuries, cervical strength training is recommended throughout the literature as a prevention strategy against athletic neck injuries, many amateur, varsity and even professional level hockey teams, however, do not include neck strengthening exercises in their training programs. In addition, training programs that do include neck strengthening exercises typically focus solely on isometric muscle contractions. Even sport-specific training resources for ice hockey, such as that by Manners [20], lack information regarding neck strengthening exercises. In contrast, wrestling programs characteristically emphasize cervical strength exercises during training, incorporating both static and dynamic neck muscle contractions, in order to meet the physical demands placed on the cervical musculature during competition [14, 31]. The emphasis towards cervical strength training and the inclusion of dynamic neck exercises may contribute to the low incidence of catastrophic neck injuries associated with wrestling. Although static testing is useful for evaluating neck strength during the initial stages of a sports training program, a dynamic testing method should be used for assessing neck strength during later stages of conditioning as the protocol used for assessing muscular performance should be specific to the training modality [16]. Very few studies involving neck strength, however, employ dynamic testing. This approach was noted by Benson et al. [1] in their literature review regarding sport concussion prevention. A 1 repetition maximum (1-RM) test is an efficient and affordable way to assess dynamic muscle strength; nevertheless, it may be inappropriate for assessing neck strength due to the increased vulnerability of the cervical spine and risk of injury involved. According to Dohoney, Chromiak, Lemire, Abadie, and Kovacs [9], however, prediction of 1-RM strength can be used to assess an individual’s maximal lifting capacity without subjecting the participant to the increased risk associated with some 1-RM lifts. A submaximal test completed to fatigue and predict an athlete’s 1-RM neck strength is, therefore, a more appropriate test. A 4 to 6-RM is a suitable submaximal test as it involves a repetition range that is consistent with strength development programs. While a predictive 1-RM neck test may be a simple and effective method for assessing athletes’ dynamic neck strength and monitoring dynamic cervical training, no research has measured the absolute 1-RM or predicted 1-RM strength for any neck movement. Although researchers have developed numerous static tests for assessing neck strength, no study has compared the static and dynamic neck strength profiles of athletes involved in various contact sports. Comparing the neck strength profiles of wrestlers and hockey players may provide valuable insight into the cervical muscle demands associated with each sport and assist coaches and trainers in prescribing appropriate neck training programs for their athletes to minimize the risk of neck injury.The purpose of this study was to compare maximal static with the predicted 1-RM neck strength among wrestlers, hockey players and controls. It was hypothesized that trained athletes would demonstrate greater static and dynamic neck strength than healthy controls, and that wrestlers would show greater static and dynamic neck strength than hockey players due to the emphasis placed on the cervical muscles during competition and training.
2. Methods
2.1. Participants
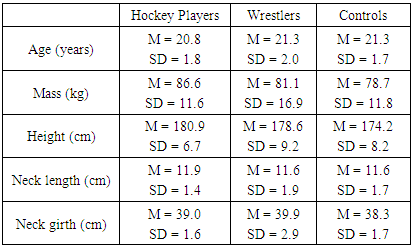
- Twenty-four participants were recruited for this study, including eight hockey players, eight wrestlers, and eight males who served as a control group (Table 1). The hockey players were recruited from a university hockey team and a junior “A” hockey team; both teams were of similar age and caliber of hockey. The wrestlers were members of a university wrestling team. A group of healthy university students served as a control group. The wrestlers and hockey players had been actively involved in a sports specific training program for at least three years. Individuals in the control group had participated in moderate, nonspecific activities for general health and fitness or recreational sport for at least three years.
|
2.2. Instrumentation
- Participants completed static and dynamic cervical strength tests for flexion and extension using a Nautilus 4-way neck strengthening machine. The Nautilus machine was chosen to evaluate neck strength because it is a standard piece of equipment used for strengthening the neck musculature. The Nautilus machine was positioned 30 centimeters from the concrete wall of the lab and bolted to the floor. A strain gauge load cell was secured to the wall behind the Nautilus machine at the same height as the head pads. The load cell was attached to the moveable arm of the Nautilus machine with a lightweight metal chain to measure the force produced during the static strength tests. The chain was removed from the Nautilus machine to measure dynamic neck strength, for which participants completed a 6-RM submaximal test to fatigue for neck flexion and extension. An electrogoniometer (Biometrics Ltd., Ladysmith, VA, USA) was also attached to the moveable arm of the Nautilus machine, and was used to ensure that each participant moved through a full range of motion for each repetition during the isotonic neck testing. Both the load cell and electrogoniometer were interfaced to an A/D Instruments Power Lab Unit and a personal computer which ran Lab Chart Software displayed the angular data and force measures in real-time.
2.3. Testing Procedures
- Each participant completed three test sessions, which were scheduled approximately one week apart at the same time of day. The first session was used to complete the pre-screening assessment and familiarize participants with the testing equipment and procedures. During the second test session, participants completed either the static or the dynamic testing protocol with the remaining testing technique being completed at the third test session. The order in which static and dynamic testing was completed was randomly assigned to each participant to limit any learning effect. Additionally, the order of cervical flexion and extension exercises were randomly assigned to participants at each session. Participants completed a standardized warm-up at the start of each session, which included 5-minutes of moderate intensity biking and a series of dynamic neck stretches. The dynamic stretches included flexion, extension, lateral flexion, rotation, and retraction movements performed through a full range of motion at a slow continuous pace without resistance. Similar static neck stretches were completed post testing as a cool-down.
2.3.1. Familiarization Session
- Once the pre-screening assessment was completed, participants were familiarized with the Borg 15-Category Scale for rating perceived exertion (RPE). Participants were asked to provide an RPE score after each working set of the familiarization and test sessions based on the amount of exertion they experienced in their neck muscles to ensure that all trials were performed at a safe and appropriate intensity. RPE values given by participants during the dynamic familiarization exercises were also used to estimate an appropriate starting weight for the 6-RM neck tests. Participants were instructed on how to rate perceived exertion according to guidelines established by Gearhart et al [13]. As recommended, a clear definition of the perception of physical exertion was provided to participants as they were presented with the Borg 15-Category Scale. The Borg Scale was placed in full view for participants throughout each test session so that they could easily relate their perceived muscle exertion with the numbers on the scale. Participants were first positioned correctly in the Nautilus machine. The seat was adjusted to the proper height so that when the participant was seated the torso was upright and the neck was in a neutral position, the head was placed against the pad of the moveable arm. The feet were positioned flat on the floor for stabilization, and the hands grasped the support handles. Participants then completed three submaximal isometric efforts of increasing intensity for cervical flexion and extension. Intensity levels included 50%, 75%, and 90% of maximal effort with 2 to 3-minutes of rest provided between each effort. Participants rated their perceived exertion immediately following each effort. During each practice trial participants were corrected on form, if necessary. Technique was monitored as a precautionary measure against injury and to ensure that all participants used consistent form during the maximal static testing.
2.3.2. Static Test Session
- The protocol used for maximal static testing was adapted from Burnett, Coleman, and Netto [3] and Leggett et al. [17]. Participants performed three maximal static efforts in either cervical flexion or extension, while maintaining a neutral neck position. Beginning with the head against the resistance pads of the Nautilus machine, participants steadily increased the amount of force produced, reaching maximum force at 3-seconds and the maintaining maximum tension for an additional 2-seconds. A metronome was used to regulate the rate and duration of each static contraction. Three minutes of rest was provided between each trial, during which participants rated their perceived exertion. Participants were verbally encouraged to give maximum efforts for all trials. The same procedure was repeated for the opposite direction of neck movement following 3 to 5-minutes of recovery. The peak static force value (measured in Newtons (N)) from the three test trials, for both flexion and extension, was used to represent the maximal static neck strength measurements of each participant.
2.3.3. Dynamic Test Session
- The 6-RM testing protocol used for dynamic strength testing was adapted from that of Kraemer, Ratamess, Fry, and French [16] and Burnett, Coleman, and Netto [3]. Each participant was properly positioned in the Nautilus machine with his head and neck in a neutral position. Beginning with flexion or extension, participants performed a light dynamic warm-up within the Nautilus machine consisting of 10 repetitions with 50% of their estimated 6-RM weight. This resistance was light enough to allow easy completion of set repetitions. Participants then completed a set of six repetitions at 70% of their estimated 6-RM weight, followed by a set of three to six repetitions at 90% of their estimated 6-RM weight, with a 1-minute rest interval between each set. Participants were then given a 3-minute rest interval before attempting six repetitions with 100% to 105% of their estimated 6-RM weight. Data from this set was accepted for predicting 1-RM values if a minimum of four to a maximum of eight repetitions were completed. Following 5-minutes of recovery, the same protocol was used to test the 6-RM for the opposite direction of neck movement. A metronome was set at the same cadence as the dynamic familiarization so that participants completed one repetition per 3-seconds, and the electrogoniometer ensured that each repetition was completed through a full range of motion. Verbal encouragement was given throughout the 6-RM protocol. Data from the 6-RM test was then entered into the equation from Wathen [29] in order to estimate each participant’s 1-RM for cervical flexion and extension, measured in kilograms (kg). W = the weight lifted, R = the number of repetitions completed, e = a mathematical constant equal to 2.71828.
 | (1) |
2.4. Statistical Analysis
- The peak static and dynamic neck strength measurement in both the flexion and extension directions was normalized for each individual by dividing the value by his body weight (N) or body mass (kg) in order to make comparisons between static and dynamic measures. A 3x2x2 mixed factorial ANOVA with repeated measures on the third factor was used to compare the normalized maximal static and dynamic neck strength among the groups. The three independent variables included participant group (wrestlers, hockey players, and controls), strength type (static and dynamic) and movement direction (flexion and extension). Significant main effects were further analysed with Bonferroni adjusted pairwise comparisons. Predictive Analytics Software (PASW) Statistics 18 for Windows was used for all statistical testing. The alpha level for statistical significance was set at p<0.05.
3. Results
- Mean normalized static and dynamic neck strength values for each group are seen in Table 2.
|
4. Discussion
- A comparison of maximal static and dynamic neck strength among wrestlers, hockey players and controls revealed unique group differences. Neck strength was found to be significantly greater for the wrestlers as compared to the hockey players and the group of healthy controls. This is similar to Rezasoltani, Ahmadi, Nehzate-Koshroh, Forohideh, and Ylinen [23] in their comparison of neck strength between elite wrestlers and a control group, who also found the static cervical flexion and extension strengths to be significantly greater in the wrestlers. The researchers attributed the differences in cervical muscle performance to the long-term specific training and competition program followed by the wrestlers. Results of the present study also suggest that the training demands of wrestlers stimulate the cervical muscles effectively enough to elicit increased static neck strength. As the nature of wrestling typically stresses the cervical muscles much more than ice hockey, it is appropriate that differences in static neck strength were greater between the wrestlers and controls than between the hockey players and the controls. While the wrestlers were significantly stronger than the controls in both movement directions, the static neck force of the hockey players was significantly greater than that of the controls for flexion movements only. Therefore, cervical muscle stress that is experienced during hockey training and competition may promote greater gains in cervical flexion strength than extension strength. The substantial cervical demands of wrestling may also account for the superior dynamic neck strength demonstrated by the wrestlers in this study. The dynamic neck strength of the wrestlers was significantly greater than that of the hockey players and the controls, for all movement directions. The normalized dynamic neck strength of the hockey players, however, did not differ significantly from the control group. This outcome suggests that the intensity of cervical muscle actions that hockey players are exposed to is not sufficient enough to increase dynamic neck strength above that of a healthy control group. Although Naish, Burnett, Burrows, Andrews and Appleby [22] found that the static neck strength of professional rugby players improved following a five-week neck strengthening program, the increase in strength was non-significant. The researchers attributed these results to the players being well-conditioned athletes. Similarly, hockey players may require greater neurological stimulation of the cervical musculature than what is experienced during games and training to improve dynamic neck strength. In ice hockey, isometric cervical muscle contractions are consistently used to maintain appropriate head and neck positioning during play. Additionally, most hockey conditioning programs consist mainly of conventional resistance exercises, without any neck specific training. According to Conley, Stone, Nimmons, and Dudley [6] conventional resistance exercises elicit forceful static contractions of the cervical musculature for stabilization. Although Conley et al. [6] reported that the stimulus is insufficient to generate neck muscle hypertrophy or improve dynamic cervical strength it may be enough to increase static strength. Therefore, the emphasis placed on isometric contractions of the neck musculature during hockey games, practices, and training may explain why the static neck strength of the hockey players did not differ significantly from that of the wrestlers for flexion or extension movements. The lack of neck specific training associated with the hockey players, however, would account for the higher static strength and the significantly greater dynamic force measurements still exhibited by the wrestlers. In contrast, a variety of techniques and maneuvers are used in wrestling which place excessive loads on the wrestler’s cervical spine [23]. For instance, a bridge position in which the back and neck are maintained in an arched position may be used as either an offensive or defensive strategy. Other contortions of the spine and neck, as well as repetitive pulling and pushing movements, are also used for controlling take downs and pinning the opponent. Such maneuvers require superior spinal and cervical strength. Additionally, stability of the cervical spine must be maintained by active co-contraction of neck extensor and flexor muscles to avoid injury [24]. Therefore, to develop both dynamic and static cervical muscle strength, wrestlers routinely include neck specific exercises in their training programs, consisting of front and back neck bridging, manual resistance and nautilus exercises [14]. Previous literature supports the concept that enhanced dynamic neck force is related to exercise intensity and muscle recruitment patterns that are developed through specific strength training [3, 4]. In comparing two dynamic cervical training modalities, including a pin-loaded machine and Thera-Band tubing, it was proposed that the increased intensity of the pin-loaded machine would be more effective for developing static neck strength [4]. The pin-loaded machine was also associated with significantly greater EMG activations in comparison to the Thera-Bands, which would explain the greater training effect produced by the machine [3]. Although dynamic neck strength was not tested in either study, results suggest that more intense dynamic exercises will generate greater muscle activation and thereby develop greater cervical muscle strength. Additionally, Murphy and Wilson [21] found that motor unit activation patterns were significantly different between static and dynamic movement. Therefore, the greater dynamic neck strength demonstrated by the wrestlers in the present study is likely related to more intense dynamic neck actions involved in training and competition as compared to the hockey players. By incorporating dynamic cervical exercises into their training, the wrestlers may have developed neural activation patterns specific to dynamic muscle contractions, which may promote increased isotonic neck force.Greater contractile forces of the cervical spine can enhance an athlete’s ability to effectively stabilize the neck during game play, enable a player to contract the neck muscles faster and with increased force at moments of impact, and improve the ability of the neck muscles to absorb external forces. Previous research has shown that greater static neck strength and anticipatory muscle activation are both associated with a reduction in linear and angular velocity of the head after impulse loading [11, 28]. Additionally, Schmidt et al. [24], found that the odds of sustaining higher magnitude head impacts were reduced with greater cervical stiffness and less angular displacement after perturbation. As explained, players with greater cervical stiffness may be better able to engage their neck muscles after a head perturbation and therefore resist head displacement [24]. It was further suggested that neuromuscular training may be required to evoke changes in cervical dynamic stabilization. Future research is needed to determine the relationship between dynamic neck strength and head kinematics and cervical stiffness at moments of impact. Also, the effect of dynamic cervical training on dynamic neck strength should be examined further as dynamic cervical muscle strength may be important to reducing neck injury and improving spinal stability in any contact sport. The physical demands of the respective sports and the differences in cervical strength profiles of the wrestlers and hockey players may be associated with specific trends in neck injuries observed within each sport. Research shows that there is an increased risk of catastrophic spine injury associated with ice hockey, typically resulting from a headfirst impact into the boards or another player. These situations can cause axial loading to the cervical spine in which the resultant injury is commonly a fracture-dislocation or burst injury at the fifth and/or sixth cervical vertebra [25]. Depending on the force and direction of the impact, the severity of this injury can range from a mild concussion to complete paralysis. Contracting the cervical extensor muscles in order to achieve a head up position prior to impact, however, can avoid axial loading and is therefore, critical to reducing the severity of the resulting injury [8]. In their study involving football players Schmidt et al. [24] found that players who contracted their cervical musculature sooner after perturbation into forced extension had reduced odds of sustaining severe head impacts. In other instances, such as those involving board collisions or body checking, appropriate neck muscle tension can reduce head acceleration and enhance the ability of the neck muscles to absorb forces [24]. As Tierney et al. [28] explained such actions could minimize the risk and severity of concussion and whiplash injuries, also common to ice hockey. In contrast to hockey, catastrophic neck injuries in wrestling are rare [15, 30]. Instead, overuse injuries to the cervical muscles and ligaments are much more prominent, typically resulting from repetitive force overload or excessive training [23]. It is plausible that the low incidence of catastrophic neck injuries in wrestling is partly due to the specific neck strengthening exercises that are emphasized in training.
5. Conclusions
- The results of this study reveal the differences in static and dynamic neck strength between hockey players and wrestlers. More attention on neck specific training in ice hockey may be beneficial to improving the neck strength of hockey players. This approach may increase the speed and strength of cervical muscular contractions and provide greater cervical stability at moments of impact, which may reduce the risk and severity of cervical injuries associated with the sport. Future research will be conducted with a larger sample size to further explore these differences.