-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2017; 7(2): 81-86
doi:10.5923/j.sports.20170702.09

Physical Activity and Health Related Physical Fitness Attributes of Staff Members in a Kenyan Public University
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLFrancis M. Mwangi1, Elijah G. Rintaugu2
1Department of Recreation Management and Exercise Science, Kenyatta University, Kenya
2Department of Recreation Management and Exercise Science, Dean, School of Applied Human Sciences, Kenyatta University, Kenya
Correspondence to: Francis M. Mwangi, Department of Recreation Management and Exercise Science, Kenyatta University, Kenya.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

High health care service cost for employees have been documented in many institutions. The purpose of the study was to assess university staff in selected health related fitness variables and their physical activity levels. A total of 237 staff members volunteered to take part in the study. International Physical Activity Questionnaire (IPAQ) short questionnaire was used to acquire physical activity information from all participants. A fitness protocol was used to record data on their health related variables; Resting heart rate (RHR), body fat percentage (%BF), blood pressure (BP) (as assessed using bioelectric impedance and an automated BP machine), and body mass index (BMI). The values rated against norms and the World Health Organization recommendations. Results showed that only 40.08% were physically active (moderate to vigorous) either inside or outside the university. 26.16% of the staff members were active in recreation activities inside the university and 28.27% were active in recreation activities outside the university. Only 41.4% recorded average or better RHR, 10.13% normal %BF, 59.07% normal to average systolic BP, 42.62% normal to average diastolic BP, and 36.3% normal BMI status. There was significant correlations between most of the variables and (p <. 05). The study concluded that majority of staff members in the institution are not physically active enough and that they are below the recommended health and fitness status. The study recommended aggressive campaign to educate the staff members on dangers of sedentary lifestyles, and the institutions to embrace prevention-based health policies to prioritize provision of fitness facilities and health promotion programs. Further studies should be done to focus on other health related variables, and cost effective benefits of staff health and fitness programs.
Keywords: Physical Activity, Resting Heart Rate, Blood pressure, Body Fat percentage, Body Mass Index
Cite this paper: Francis M. Mwangi, Elijah G. Rintaugu, Physical Activity and Health Related Physical Fitness Attributes of Staff Members in a Kenyan Public University, International Journal of Sports Science, Vol. 7 No. 2, 2017, pp. 81-86. doi: 10.5923/j.sports.20170702.09.
1. Introduction
- Health and fitness parameters are known to improve with increases in physical activity (PA) levels. Body composition, aerobic capacity, muscular strength and endurance, coordination and flexibility are some of health and fitness indicators which correlate with physically active lifestyles [26, 23, 29]. Physical exercise has been shown to reduce the severity and outcome of three of the most common chronic degenerative diseases of westernized nations: hypertension, coronary heart disease and non-insulin-dependent diabetes mellitus (type II diabetes) [20]. Physical activity also has a well-known role in preventing and reducing obesity, and has beneficial influence on insulin metabolism [22]. Furthermore, increased levels of PA have a positive impact in virtually all chronic diseases, including but not limited to stroke, peripheral artery disease, chronic obstructive pulmonary disease, osteoporosis and some forms of cancer [29]. World Health Organization (WHO) defines health as ‘a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity’ [30]. To promote and maintain health, all healthy adults aged 18 to 65 years need moderate-intensity aerobic (endurance) physical activity for a minimum of 30 min on five days each week or vigorous-intensity aerobic physical activity for a minimum of 20 min on three days each week [2, 6]. Although changes such as urbanization, reduced manual labour, and more motorization of transportation (which have contributed to low physical activity levels and correspondingly higher obesity rates) are mostly associated with industrialized and affluent nations [16], sedentary behaviour and the concomitant ill health is becoming increasingly common in developing countries like Kenya [16, 31]. Due to mechanization and industrialization, occupational physical activity levels have reduced in many communities. There is often a need for additional daily physical activities designed to improve health and fitness. USDHHS (2000) observe that, adoption and maintenance of regular physical activity is an important component of any health regime which provides multiple opportunities to improve and maintain health [29]. The authors continues to assert that because few occupations today provide sufficient vigorous or moderate physical activity to produce health benefits, sufficient physical activity should be encouraged and planned as part of a daily routine or leisure time activities [29].In most universities in the developing countries, sports and exercise facilities are assembled for students only. Most of the staff members do not use these facilities though the universities pay huge medical bills for their staff. According to Sturm (2002), health care service cost for employees who are obese are 36% greater than for individuals who are not obese, and 77% more on medications [27]. These expenses include medical insurance premiums, hospitalization, physician visits, outpatient testing and treatment, laboratory radiology and pharmaceuticals. In addition, there are indirect costs which include decreased productivity and lost time due to increased absenteeism, as well as opportunity cost [27, 11]. Naguin, Zannis and Lowe (2008) observe that, health promotion especially in the form of increased physical activity among employees could improve the overall health of the participants, cut down on absenteeism and reduce health care costs [11]. Proper and Mechelen (2008) as well as Robert and Bertera (1990) also presented empirical evidence of decreased health care costs, less workplace absenteeism and increase in level of fitness and decreases in chronic disease as a result of work site health promotion programmes [19, 21].The scenario depicted by the cited literature indicated that physical activity as part of health promotion programs is essential to enhance productivity both at individual and at institutional levels. The purpose of the current study was to establish health related fitness status of public university staff members and their current physical activity levels, as well as the relationships among the same. The rationale was that, after the staff members know their fitness status and the implications of their PA levels, they would pursue and/or maintain physically active lifestyles. Also, the university would put up the necessary measures to enhance fitness infrastructure and programmes to boost the welfare of the employees and reduce health-related costs.
2. Methods
- Cross sectional survey design was adopted for the study. A total of 237 staff members (102 Male; 43% and 135 Female; 57%) from various sections/ units volunteered to take part in the study. A self-reported IPAQ short questionnaire based on 7-day recall [28] was used to capture physical activity and demographic information of the participants. A fitness protocol was used to record data on their health related variables. Resting Heart Rate, Blood pressure, Body Fat percentage, and Body Mass Index were selected as basic indicators of fitness and health which can be followed up easily by the participants even after the study. The procedures for the measuring these variables were non-invasive. Permission to carry out the survey was granted by the office of the Vice Chancellor and request for members to volunteer to be tested was circulated. The members were informed of the objectives and the procedures of the tests before they accented to be participants. The tests were conducted by qualified personnel in the sports and games department using.The resting heart rate, systolic and diastolic blood pressure were assessed using an automated BP machine (Omron Healthcare HEM-629N), and the variables measurements taken when the participant was rested in seated position. Body height / stature measurements were made by having the participant stand on the footplate of the stadiometer (Height Measure SE001, Leicester) without shoes. The individual was positioned with heels close together, legs straight, arms at sides, shoulders relaxed. The participant’s head was held in the Frankfort plane and the participant was asked to inhale deeply and to stand fully erect without altering the position of the heels. The headpiece lowered snugly to the crown of the head with sufficient pressure to compress the hair. The reading was made to the nearest 0.1 of centimeter with the measurer’s eyes parallel to the headpiece for accuracy, as described in the ISAK manual [9]. For body weight measurements, participants were weighed without shoes on and wearing only lightweight garments. They were asked to stand on the platform of electronic/digital weighing scale (Seca aura 807, Leicester) and the weight of the individual was recorded to the nearest 0.1 kg. The body mass index were calculated from the above height and weight measures, while body fat percentage was assessed using a Body Fat Monitor bioelectric impedance (Omron BF306). Values were rated against the recommendations of the WHO (2010), WHO (1995) and Netfit (2016a) [31, 32, 12]. The data was coded and processed using SPSS software.
3. Results
- The participants’ average age was 36.78 ± 9.51 years (Mean ± SD). Descriptive summary of data collected on staff recreation tendencies within and outside the institution indicates that majority of the members (59.92%) are not actively involved in any physically active recreational activities. Only 26.16% of the staff members were active in recreation activities inside the university and 28.27% were active in recreation activities outside the university. Out of 40.08% who were active (moderate to vigorous physical activity) either inside or outside the university, 58.94% were male and 41.05% female. The results of the fitness and health assessments tests are shown in tables and figures below. Up to 41.4% recorded average or better resting heart rate (RHR) status (Table 1). 59.07% normal to average systolic BP (Figure 1), 42.62% normal to average diastolic BP, 10.13% normal body fat (Figure 2) and 36.3% normal body mass index (BMI) (Figure 3). The percentage of participant recording values lower or higher than those considered as indicators of good health were 58.6 (heart rate) (Table 1), 40.0 (systolic BP) (Figure 1), 56.0 (diastolic BP), 85.23 (body fat) (Figure 2), and 63.75 (BMI) (Figure 3). The figures indicate that majority of the participants are not physically fit in terms of the fitness attributes that were considered.
|
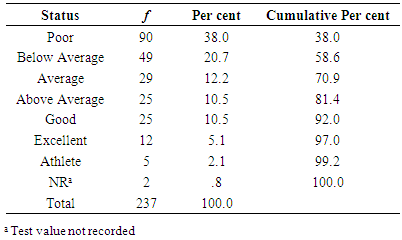
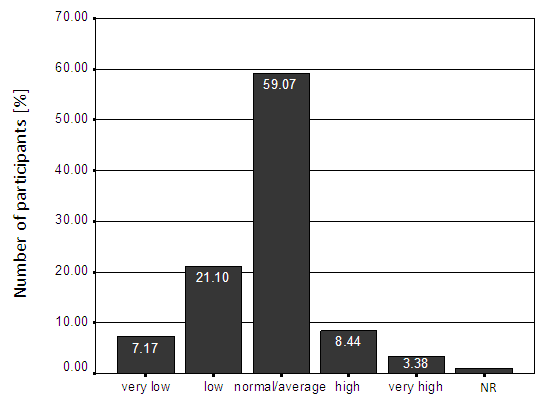 | Figure 1. Status of participants’ systolic blood pressure (n = 237) |
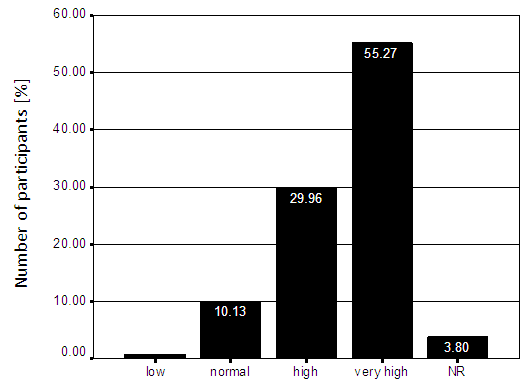 | Figure 2. Status of the participant's body fat percentage (n = 237) |
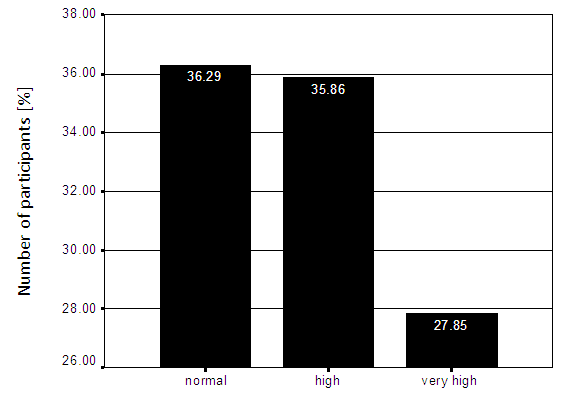 | Figure 3. Status of the participant's body mass index (n = 237) |
|
4. Discussion
- Health-related components of physical fitness include body composition, cardiorespiratory function, flexibility, and muscular strength/endurance [29]. Engaging in physical activity is associated with positive influence to these components, and thus better health outcomes. According to America College of Sports Medicine (ACSM) position stand [2], all healthy adults aged 18 to 65 years need moderate-intensity aerobic (endurance) physical activity for a minimum of 30 minutes on five days each week or vigorous-intensity aerobic physical activity for a minimum of 20 minutes on three days each week, to promote and maintain health [2, 6]. One can also combine moderate and vigorous intensity activities to meet this recommendation. Moderate-intensity aerobic activity, which is generally equivalent to a brisk walk and noticeably accelerates the heart rate, can be accumulated toward the 30-minutes minimum by performing bouts each lasting 10 or more minutes. Vigorous-intensity activity is exemplified by jogging, and causes rapid breathing and a substantial increase in heart rate. In addition, every adult should perform activities that maintain or increase muscular strength and endurance a minimum of two days each week [2, 6].The current study focussed on assessing body composition related variables among university staff members, and their physical activity patterns. This appraisal was aimed at establishing the base values before re-launching on-campus fitness programmes for staff members. It was hoped that members would be motivated to engage in PA when they were enlightened about the health-related fitness variables and their individual status.Heart rate variable values are influenced by an individual’s age and level of cardio-respiratory fitness. Percentage of maximum heart rate (%MHR) at rest (and during exercise) have been used to predict cardio-respiratory fitness, with the maximum heart rate (MHR) measured directly, or estimated from age-based formulae [5, 18]. The values in the current study were interpreted using age determined norms [13] and presented in Table 1. Someone’s resting heart rate is said to often be a good determination as to how fit one is. Fitness exercises are known to induce resting bradycardia. As one become fitter through aerobic exercise, the heart becomes more efficient at pumping blood around the body, especially if combined with a reduction of the plaque (fatty deposits) within arteries. As a result the resting heart rate gets lower. Therefore, the lower the HR, the healthier the person, and the more the capacity to perform given tasks more successfully [5, 7, 18].Blood pressure (BP) is measured and reported in terms of systolic / diastolic BP in mmHg. It is considered when reading around 120 / 80. One is considered to have borderline hypertension when the reading is 140 / 90, moderate to high risk if 141 / 90 to 160 / 95, and a high risk if the reading is higher than 160 / 95. One should consult a doctor prior to starting any exercise program if the BP readings fall under moderate or high risk. Low blood pressure (hypotension) on the other hand is pressure that is so low (around 100/60) that it cause a lack of oxygen to vital organs such as the brain due to the low flow of blood through the arteries and veins. When someone is either high or low blood pressure readings, the person should take extra care with workouts, especially when increasing heart rate or working with heavy weights. Those with low blood pressure should aim to spend extra time warming up the body to assist with blood flow, and be keen to always consult with their doctor anytime they feel unsure or un-well [14]. Moderate and high intensity cardio vascular exercises have been shown to lower resting blood pressure. Ghadieh Saab (2015) found through a systematic clinical review that moderate intensity aerobic exercise has been proven to prevent hypertension and to help in the management of grade 1 hypertension [4].Body fat percentage has been used as a measure of health related fitness, with high percentage of the same associated with health risks conditions such as Overweight, Obesity, High BP, High lipidemia, arterosclelosis, cholesterols etc. Everyone requires a minimum amount of body fat - about 5% for men and 8% for women [8]. This fat is called essential fat and is necessary for good health. Body fat values are influenced by an individual’s diet, body type, age and level of cardio-respiratory fitness. Heyward (2006) suggested that fat tend to accumulate as one grows older because of decreased activity level and increased adipocytes in the body [7]. St-Onge and Gallagher (2010) observed that increased age may be accompanied by increased per cent body fat [25], which invariably would lead to an increase in total body weight in middle aged persons before the onset of decrease in lean mass. This may explain the significant correlations noted in the current study between age category and percentage body fat and BMI. However, the average age of the participants (36.78 ± 9.51 years) cannot account for the high percentages found with high and very high percentage body fat. High body fat is often associated with over-weight status. However, a high body fat level is a far greater risk to one’s health than being over-weight. This is because muscle tissue is far heavier and denser than body fat, so as one become fitter with exercise, body weight may increase with or without body fat percentage coming down, depending on type of exercise and the fat intake through diet. In the current study, body fat was assessed through Bioelectrical Impedance which is a far less invasive than the older method of using callipers at various body points. Norms from Netfit (2016d) and WHO (1995) were used to rate and interpret the values [15, 32].The study findings are significant in that they revealed that smaller percentage of staff members is physically active and corresponds to the lower percentages of the members of staff who recorded average to normal health related fitness indices. The findings are in agreement with a related study by Omondi, et al., (2007) which revealed a significant relationship between health status and physical activity among university staff members [17]. In the study conducted to determine the relationship between physical activity patterns, dietary intake and health status of lecturers at the University of Nairobi, 120 lecturers were involved where data collection questionnaires with a physical activity checklist based on 7-day recall, 24-hour food recall, anthropometric, blood pressure measurements, and diabetes-related questions were applied. A significant relationship between health status and physical activity (χ2 =27.54, N=118) was revealed [17].Related studies in other countries reveal similar tread to the current one. A study to assess the level of physical activity and anthropometric measurements among bank officials in Nigeria found more than half of respondents (60%) of the 50 bank workers who participated either overweight or obese [1]. Most university employees were found to spent 75% of their workday seated (with the exception of facilities management workers), and had low levels of leisure time PA [3]. The author concluded that university employees are prime candidates for workplace interventions to reduce physical inactivity. Sampson-Akpan et al., (2013) conducted a study to determine academic staff perceptions of the necessity of physical activity (PA) for quality living and involvement in physical activity in universities in Cross Rivers state, Nigeria [24]. The 400 university lecturers involved had high perception that PA enhances quality living though their involvement in P.A. was very low [24]. Morakinyo & Omolawon (2008) investigated selected psycho-social factors that serve as inhibitors to recreational sports participation among residents of university of Ibadan, Oyo state, Nigeria [10]. From the 400 respondents, the variables of occupational/ academic demands, motivation and age used in the study had significant psycho-social influence on recreational sports participation among the residents [10]. The current study adopted similar approaches to those used in the above cited studies (save for diet and psycho-social issues) and the results are in concurrence, calling for enhancement of health and fitness programmes as well as more health promotion and education in various institutions. The results indicates that effort need to have sufficiently equipped gym available for members as well as qualified and competent personnel to vibrant elaborate health and fitness programs in order to reverse the grim status of the staff members. There is need also for prevention-based health policies which would help to prioritise establishment and provision of fitness and recreation facilities and programs, in order to save the institution the loss accruing from less productive unfit staff, absenteeism and cost of medical consultation, treatment, medication, as well as redeem opportunity costs.
5. Conclusions
- The study concluded that majority of staff members in the institution are not physically active enough and that they are below the recommended health and fitness status. There exist high correlations between participation in active recreation physical activities and status of the health-related fitness variables. The study recommends that aggressive campaign be carried out with the aim to educating the staff members on dangers of sedentary lifestyles. This would help in getting the university staff active for their health benefits as well as for good role modelling in the society. The institutions’ health units need to work hand in hand with professionals who are knowledgeable in exercise prescription to handle cases of hypokinetic diseases. Further studies should be done to focus on other health related variables, and cost effective benefits analyses of staff health and fitness centres and programs with the view of guiding the institutions on policy and practice in this regard. Staff health and medical programmes should also focus on prevention and health promotion in addition to the traditional approaches that focus on treatment and rehabilitation.
ACKNOWLEDGEMENTS
- The authors wish to acknowledge with appreciation the contribution of the following persons who assisted in some data collection processes; Joan A. Adalo, James O. Omondi, Moses O. Ondeng, Hellen Ngethe and Kizito Mukhwana. Our gratitude also goes to all the study participants.