-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2016; 6(6): 257-261
doi:10.5923/j.sports.20160606.09

The Effects of Adaptive Strength Training in Female Adults
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSascha Gail1, Steffen Rodefeld2, Sabine Maier1, Stefan Künzell1
1Institute of Sports Science / Sports Centre, Augsburg University, Augsburg, Germany
2Therapy and Training Department, Hessingpark-Clinic GmbH, Augsburg, Germany
Correspondence to: Sascha Gail, Institute of Sports Science / Sports Centre, Augsburg University, Augsburg, Germany.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The purpose of this study is to investigate the effects of the relatively new so-called adaptive strength training by comparing it to a conventional strength training in female adults. Twenty-six healthy female adults were randomly allocated to perform either an adaptive strength training or a conventional strength training over a period of 8 weeks. Both strength training programs consisted of the following exercises: leg press, leg extension, latissimus pull-down and rowing. The program was conducted twice a week with at least 48 hours break between each training session. In order to analyze the effects we determine isokinetic maximum strength as well as body composition immediately before and immediately after the intervention phase. In all four exercises the participants showed significant improvements in isokinetic maximum strength during retests (p < 0.05; 0.445 ≤ η2 ≤ 0.616), which is especially relevant to general practice. Significant differences between the intervention groups were not found (p < 0.05; 0.000 ≤ η2 ≤ 0.108). Furthermore, the participants had no significant differences in any of the investigated body composition parameters during retests (p < 0.05; 0.000 ≤ η2 ≤ 0.009). Differences between the two intervention groups were also insignificant for body composition parameters (p < 0.05; 0.005 ≤ η2 ≤ 0.064). Effects of adaptive strength training and conventional strength training are very similar in female adults after a training period of 8 weeks.
Keywords: Body Composition, High Intensity, Maximum Strength, Muscle Fatigue, Strength Training Method
Cite this paper: Sascha Gail, Steffen Rodefeld, Sabine Maier, Stefan Künzell, The Effects of Adaptive Strength Training in Female Adults, International Journal of Sports Science, Vol. 6 No. 6, 2016, pp. 257-261. doi: 10.5923/j.sports.20160606.09.
Article Outline
1. Introduction
- Strength training is highly recommended by medical professionals and sports scientists worldwide. Health organizations also state its numerous potential benefits on health and fitness condition. Strength training evidently increases lean body mass, reduces body fat, raises resting metabolic rate, and effects bone mineral density. For a summary, see Kraemer, Ratamess and French [1]. It also improves blood lipid profiles, glucose tolerance and insulin sensitivity, and decreases blood pressure [2]. Furthermore, strength training relieves lower back pain [2]. Moreover, strength training plays an important role in the prevention and treatment of chronic diseases such as diabetes and hypertension [3]. It is also commonly known that strength training is an effective strategy to counteract the degenerative aging process [4-7].In order to achieve specific goals through strength training various methods can be taken into consideration. For instance, in order to target muscle hypertrophy the American College of Sports Medicine [8] generally suggests training sets with six to twelve repetitions and heavy weights. A relatively new method is the adaptive strength training (in-house development by milon industries GmbH, Emersacker, Germany). Here, the resistance is adapted in accordance to the power reserves of the person who is exercising. In order to determine the remaining power, a computer program within the exercise device permanently analyzes the speed of the movement and if the exercise is executed in the recommended range of motion and velocity. In addition, the program considers some adaptation rules. The first rule is that if the person exercising cannot hold the concentric resistance, the concentric resistance decreases. The second rule is that if the person cannot hold the eccentric resistance, the eccentric resistance decreases. The third rule implies that if the person exercising cannot hold neither the concentric resistance nor the eccentric resistance, both loads decrease. The last rule is that if the exercising person cannot hold the predefined end position of the exercise, which means a shorter range of motion (ROM), both loads decrease automatically. By applying these rules, the adaptive strength training should lead to stronger muscle fatigue and larger effects compared to a conventional strength training.To the best of our knowledge, this present study is the first that investigates systematically the effects of adaptive strength training. Here, we compare the effects between an adaptive strength training program and a conventional strength training program in female adults.
2. Methods
2.1. Participants
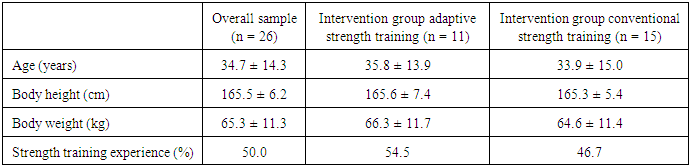
- Twenty-six healthy female adults without exercise contraindications participated voluntarily in this study and gave their written informed consent (Table 1). The participants had an age, body height and body weight of 34.7 ± 14.3 years, 165.5 ± 6.2 cm and 65.3 ± 11.3 kg, respectively. Thirteen participants had at least 3 months strength training experience, whereas thirteen participants were inexperienced. Six further people had to stop participating due to illness or time issues. All the procedures undertaken in this study were approved by the local ethics board of the University of Augsburg and are in compliance with the Declaration of Helsinki.
|
2.2. Experimental Design
- Participants were randomly allocated to either the intervention group executing the adaptive strength training or the intervention group executing the conventional strength training. Both intervention groups included a strength training program for 8 weeks that consisted of the following exercises: leg press, leg extension, latissimus pull-down and rowing. The participants carried out the strength training program twice a week with at least 48 hours break between the training sessions. All exercises were performed in three sets with ten repetitions and separated by a two minutes rest between each set. The speed of movement (SOM) was 2 – 0 – 2 (eccentric – isometric – concentric). As a result, the time under tension (TUT) amounted 40 seconds, which corresponded with the common recommendations for muscle hypertrophy training [9].
2.3. Experimental Procedures
- At first, all participants completed a preparation session, where the exercise devices (miltronic Premium Med; milon industries GmbH, Emersacker, Germany) were introduced and the correct exercise techniques shown to the participants. The miltronic Premium Med devices gave visual feedback to the participants about the correct ROM and the appropriate SOM as well as the time of movement turnaround during the exercise. The appropriate adjustment of the exercise devices was controlled by adjustment data saved on a chip card. After the preparation session, the participants passed three habituation training sessions. In order to analyze the effects, a comprehensive assessment took place immediately before the intervention phase (test) as well as immediately after the intervention phase (retest). The diagnostic included isokinetic maximum strength tests (maximum measurement error less than 5 percent according to the exercise device manufacturer) with the four training exercises and a body composition assessment. For the isokinetic maximum strength tests, three test trials with 10 seconds rest between the test trials were performed. The best test trial was used for the diagnostic result as well as to determine the training weights for both strength training programs. The body composition assessment was based on a bio-impedance measuring device (Biacorpus RX 4000; MEDI CAL HealthCare GmbH, Karlsruhe, Germany) and considered body weight in kg, lean body mass in kg, lean body mass in %, body fat in kg, and body fat in %. Test and retest took place approximately at the same time of the day to avoid any impacts on the strength test results through the circadian rhythm [10, 11] or on the body composition, through diet-related fluctuations (e.g. deviations of water balance). All tests were instructed and supervised by the same experimenter. Each participant was tested separately and requested to exercise with maximum effort. The warm-up comprised of 10 minutes moderate cycling (1 watt per kilogram body weight at 60-80 revolutions per minute) and one submaximal set of the test exercises (ten repetitions). Due to negative effects on strength performance [12] and the lack of evidence for injury prevention [13], stretching was not included. All participants started with leg press followed by leg extension, then latissimus pull-down and rowing. For the conventional strength training program concentric and eccentric training weights were fixed on 85% of the maximum strength, which corresponded with the best test trial of the isokinetic maximum strength test. For the adaptive strength training program the concentric and eccentric training weights were the same at the beginning of the training sets. In comparison to the conventional strength training program, during the exercises some additional adaptation rules were considered, which are described in detail in the introduction chapter.
2.4. Statistical Analysis
- All statistical analyses were carried out using the statistical software IBM® SPSS® Statistics version 23 (IBM® Corp., Armonk, NY, USA). Results are shown as mean ± standard deviation. In order to identify effects a variance analysis with repeated measurements with both factors, time of measurement (test vs. retest) and intervention group (adaptive strength training vs. conventional strength training), was conducted. The examination of the requirements occurred with the Shapiro-Wilk test (standard distribution) and the Levene test (variance homogeneity). An alpha of 5% was accepted as statistically significant.
3. Results
3.1. Maximum Strength
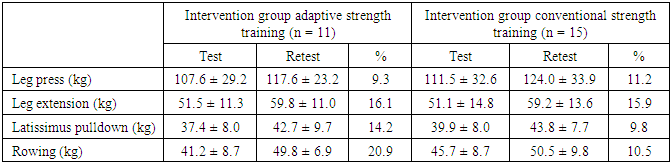
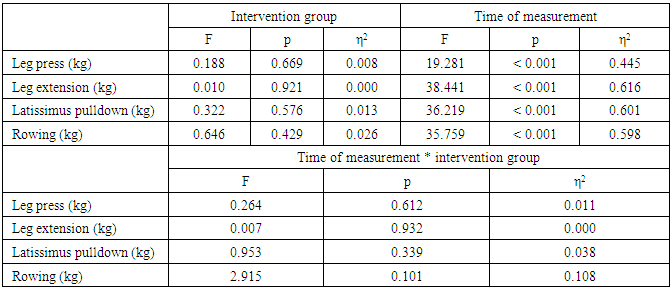
- Table 2 and 3 present the results concerning maximum strength. The participants showed for all four exercises significant (p < 0.05) improvements in isokinetic maximum strength during retests and therefore constitute a relevance to general practice (0.445 ≤ η2 ≤ 0.616). Depending on the exercise, the increases amounted 9.3% - 20.9% for the intervention group adaptive strength training and 9.8% - 15.9% for the intervention group conventional strength training. Statistical significant differences between the intervention groups were not found (p < 0.05; 0.000 ≤ η2 ≤ 0.108).
|
|
3.2. Body Composition
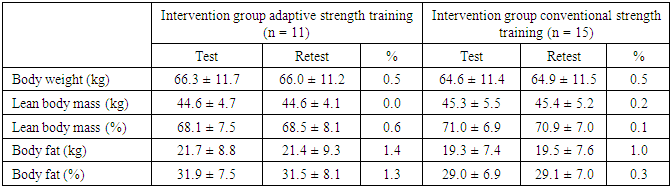
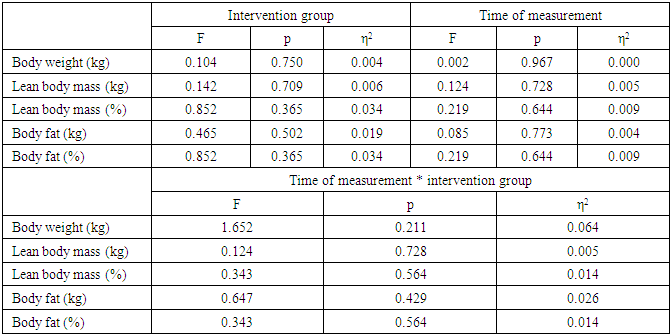
- The effects with respect to body composition are reported in Table 4 and Table 5. Accordingly, the participants showed no statistical significant (p < 0.05) or relevant (0.000 ≤ η2 ≤ 0.009) differences in any of the examined parameters during retests. Differences between the two intervention groups were not found (p < 0.05; 0.005 ≤ η2 ≤ 0.064).
|
|
4. Discussion
- The aim of this study was to analyze the effects of adaptive strength training in recreational sport. For this purpose, we compared the effects between an adaptive strength training program and a conventional strength training program.As Toigo and Boutellier [14] first discussed and Marschall and Büsch [15] insisted upon, the present intervention study refined and controlled further exercise descriptors, e.g. fractional and temporal distribution of the contraction modes per repetition and duration of one repetition. These are relevant to target any training adaptations and are in addition to the common exercise descriptors, e.g. number of sets [14, 15]. Finally, for strength training the afore-mentioned important exercise descriptors from Toigo and Boutellier [14] (i.e. load magnitude, number of repetitions, number of sets, rest in-between sets, number of exercise interventions, duration of the experimental period, fractional and temporal distribution of the contraction modes per repetition and duration of one repetition, rest in-between repetitions, TUT, volitional muscle failure, ROM, recovery time in-between exercise sessions, anatomical definition of the exercise) were taken into consideration. Another special feature of the present study was that the participants were exclusively female adults, whereas most intervention studies dealing with the effects of strength training methods are usually conducted with male athletes [16-18]. This is especially meaningful because a previously neglected target group in strength training intervention studies has now been studied.We show that a systematic strength training over a period of 8 weeks already leads to relevant improvements of maximum strength in female adults. An increase of maximum strength, as a basic parameter of explosive strength, is not only beneficial in competitive sports, but also in recreational sport as a preventive measure, e.g. joint stability in daily life [19]. A potential benefit of adaptive strength training in comparison to conventional strength training could not be found. After a training period of 8 weeks adaptive strength training as well as conventional strength training results in similar effects regarding maximum strength in female adults. Therefore, other factors, such as enjoyment or motivation during exercising, should be taken into account whether an adaptive strength training or a conventional strength training is suitable. However, it can be assumed that compliance and sustainability in adaptive strength training is higher than in conventional strength training and therefore would allow larger effects in long-term perspectives. This can be derived from the fact that in adaptive strength training the load decreases automatically if the load is too heavy to be adequately overcome. However, in the present study participants quitting due to illness and time issues was moderately higher in the intervention group adaptive strength training than in the intervention group conventional strength training. We believe that this was a coincidence. Limitations of the study were in particular the restricted intervention period of 8 weeks as well as the exemplary choice of only four exercises. These aspects can also explain the absence of significant changes of body composition parameters. The extent of training intervention, particularly the duration of the intervention period and the number of exercises, was obviously not sufficient to achieve relevant increase of lean body mass and/or relevant decrease of body fat in general practice.There are some interesting research prospects for adaptive strength training. In further intervention studies, the effects of adaptive strength training with extended training periods as well as with more exercises (e.g. a whole-body training program) could be examined. Furthermore, the effects of adaptive strength training in other target groups such as men, adolescent, rehabilitation patients and competitive athletes could be focused on in future investigations.
5. Conclusions
- In conclusion, the effects of adaptive strength training and conventional strength training are very similar. Thus, other factors such as enjoyment or training motivation during exercising should be considered in the method applied. However, these results are only valid for female adults in case of a training period of 8 weeks and with a limited number of exercises. In order to make more general training recommendations, further intervention studies with longer training periods in form of a whole-body training program as well as other target groups are needed.
ACKNOWLEDGEMENTS
- The authors thank all participants for their cooperation in this study. The authors have no conflict of interest.