-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2015; 5(5): 209-212
doi:10.5923/j.sports.20150505.06
Effect of Levels of Physical Activity on Pulmonary Function of Male Saudi University Students
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAhmed Sayed Khashaba
Assistant Professor- Physiology Medicine, Riyadh Colleges of Dentistry and Pharmacy
Correspondence to: Ahmed Sayed Khashaba, Assistant Professor- Physiology Medicine, Riyadh Colleges of Dentistry and Pharmacy.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Objective: To assess levels of physical activity among Saudi male college students and to explore the possible effect of different levels of physical activity on their respiratory function. SubjectsandMethods: The present study included 400 Saudi male students at the Riyadh Colleges of Dentistry and Pharmacy, Riyadh City, Saudi Arabia. An anonymous, self-administered questionnaire was used to collect data about personal characteristics and self-reported level of physical activity and amount of leisure time spent as inactive, using the official Arabic short version of the International Physical Activity Questionnaire. Pulmonary function testing was performed using the standards outlined by the American Thoracic Society. Results:More than half of university students (54.5%) were physically inactive while 30.5% and 15% had moderate and high intensity physical activities, respectively. Pulmonary function measurements did not differ significantly according to students' age but differed significantly according to students' physical activity levels, with least values among students with low physical activity levels and highest values among students with high physical activity levels. Conclusions:Low physical activity is a common problem among male Saudi university students. Those who are physically active have better pulmonary function parameters.
Keywords: Physical inactivity, Pulmonary function, Spirometry, Saudi Arabia
Cite this paper: Ahmed Sayed Khashaba, Effect of Levels of Physical Activity on Pulmonary Function of Male Saudi University Students, International Journal of Sports Science, Vol. 5 No. 5, 2015, pp. 209-212. doi: 10.5923/j.sports.20150505.06.
Article Outline
1. Introduction
- Physical exercise is vital for a healthy life and has several positive influences on the body, especially the cardiovascular and respiratory systems. It improves endurance and diminishes breathlessness (Fatima et al., 2013). On the other hand, physical inactivity adversely influences body weight and is associated with obesity, which in turn may cause a restrictive syndrome, reducing lung volumes due to the accumulation of perithoracic and abdominal fat (Padez et al., 2004). As far as effect of physical activity on respiratory functions is concerned, recent developments in exercise physiology have shown significantly positive improvements. However, non-significant associations have also been reported (Prakash et al., 2007). Respiratory function depends on many factors, including nervous system, strength of respiratory muscles, and lung dimensions. Spirometry is an important tool for evaluating cardiovascular and respiratory functions (Azad et al., 2011). Forced vital capacity (FVC) and forced expiratory volume in one second (FEV1) are strong indicators of respiratory function (Azad et al., 2011). FEV1 is the most crucial in detecting pulmonary changes easily and effectively in clinical settings and in settings where obesity is prevalent (Thaman et al., 2010). FVC predicts the compliance of lungs and the chest wall (Miller et al., 2005).
2. Study Rationale
- Generally, physical inactivity is common among students. This is due to their busy academic schedule and that students’ parents usually give academic success a higher priority over exercise (El-Gilany and El-Masry, 2011). Due to the lifestyle changes that are currently occurring in Saudi Arabia, as one of the rich petroleum producing Gulf countnries, the Saudi community suffers from high level of physical inactivity. As a result, sedentary living and low levels of physical activity are becoming increasingly prevalent among the Saudi population. In addition, with students’ increased reliance on computer and telecommunication technology, further reductions in PA are projected for the coming years (Al-Hazzaa, 2004).It is important to assess physical activity among college students since the majority of those who exercise regularly at university remain physically active 5 or 10 years later, while most physically inactive university students maintain a sedentary lifestyle afterwards (Sparling and Snow, 2002). Moreover, results of several studies showed that the relationships between measurements of respiratory function and the level of physical activity in daily life are controversial, varying from weak and not statistically significant to strong and statistically significant associations (Steele et al., 2000; Belza et al., 2001; Singh and Morgan, 2001; Pitta et al., 2005). Therefore, the present study aimed to assess levels of physical activity among Saudi male college students and to explore the effect of different levels of students’ physical activity on their respiratory function.
3. Methods
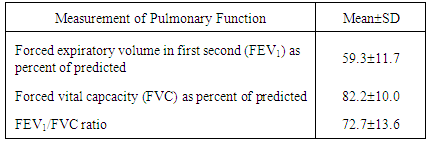
- The present study followed a cross sectional design. A simple random sample was followed to include 400 Saudi male students at the Riyadh Colleges of Dentistry and Pharmacy (RCsDP), Riyadh City, Saudi Arabia. The study was conducted during the period from January to April 2015. Students with chronic diseases (e.g., diabetes, bronchial asthma) were excluded from the study.An anonymous, self-administered questionnaire was used to collect data about personal characteristics and self-reported level of physical activity and amount of leisure time spent as inactive. Physical activity was assessed using the official Arabic short version of the International Physical Activity Questionnaire (IPAQ), which was designed primarily for population surveillance of physical activity among adults (age range 15–69 years). The IPAQ has items regarding time spent in walking, vigorous and moderate intensity physical activities and in sedentary activity during the previous 7 days (Awadalla et al., 2014). The Arabic version has been validated and used by several studies among the Saudi Arabia adult population (Al-Hazzaa, 2004; Al-Hazzaa, 2006; Awadalla et al., 2014).Pulmonary function parameters were measured by an experienced technician using MIR Spirolab III machine, Medical International Research USA, Inc. It is a desktop multifunction spirometer with graphical display and built-in printer. It can be used as a stand-alone or with the WinspiroPro software connected to a PC. Before testing, the required maneuvers were demonstrated by the researcher. Pulmonary function testing was performed using the standards outlined by the American Thoracic Society (1995). Common measurements included forced expiratory volume for the 1st second (FEV1); forced vital capacity (FVC) and the ratio between FEV1 and FVC (FEV1/FVC). Pulmonary function tests were performed three times for each subject. The average for each of the three readings was calculated. The percentages of predicted values for FVC and FEV1 were calculated.Physical activity scores and levels were calculated according to the guidelines for data processing and analysis of the IPAQ (IPAQ Research Committee, 2005).
4. Research Hypotheses
- - Null hypothesis (Ho): Pulmonary function measurements of male Saudi university students do not differ signficiantly according to students’ level of physical activity.- Alternative hypothesis (Ha): Pulmonary function measurements of male Saudi university students differ signficiantly according to students’ level of physical activity.
5. Statistical Analysis
- Collected data were analyzed using the Statistical Package for Social Sciences (SPSS), Version 22. Results of qualitative variables were presented as frequency and percentage, while results of quantitative variables were presented as means and standard deviations. Levene’s test was applied to test normality and homogeneity of variances. Hence, results were compared using one-way analysis of variance. P-values less than an alpha level of 5% were considered as “statistically significant”.
6. Results
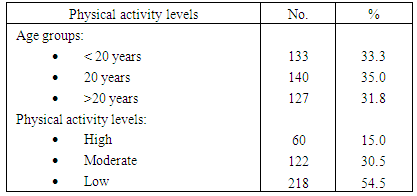
- Table (1) shows that the age of one third of students (33.3%) was less than 20 years, while 35% aged 20 years and 31.8% aged above 20 years. More than half of university students (54.5%) were physically inactive while 30.5% and 15% had moderate and high intensity physical activities, respectively.
|
|
|
7. Discussion
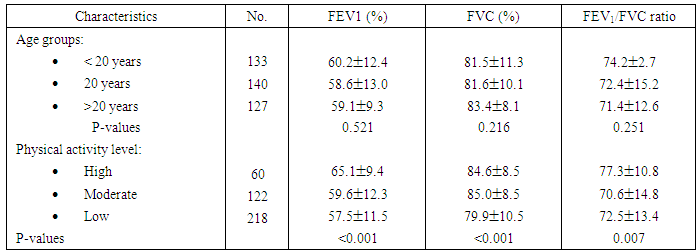
- The measurement of physical activity is an important part of health promoting efforts to manage physical inactivity. Increasing physical activity is considered to be as important as tobacco control, promoting a healthy diet and obesity prevention in minimizing the burden of non-communicable diseases (Bauman et al., 2006).The present study revealed that more than half of Saudi male college students had low physical activity. This finding is in agrement with those of Al-Rafaee and Al-Hazzaa (2001), who reported that over 53% of Saudi males in Riyadh are physically inactive, and another 27.5% are irregularly active, while only 19% are physically active on a regular basis. In a large population-based cross-sectional study, Al-Nozha et al. (2007) reported that only 3.9% of adult Saudis aged 30-70 years perform regular physical activity. The World Health Organisation (2002) reported that physical inactivity in the Saudi population seems to be among the highest in the world. The high prevalence rates for physical inactivity among young Saudi males can be explained by the rapid economic growth surge in the Kingdom of Saudi Arabia, which led to increasingly sedentary lifestyles and other behaviour changes associated with affluence. These changes led to widespread physical inactivity and a low level of physical fitness (Al-Hazzaa et al. 2011; Mahfouz et al., 2011; Khalaf et al., 2013).Regarding the research hypotheses, results of this study showed that pulmonary function measurements differed significantly according to students’ physical activity levels. Mean values for predicted FEV1 (%) and predicted FVC (%) among students were least among students with low physical activity levels, while highest FEV1/FVC ratio was observed among students with high activity levels compared with those with moderate or low activity levels. These findings provide enough evidence to reject the null hypothesis (Ho).These findings were reported and explained by several authors. Thaman et al. (2010) noted that physical exercise controls many crucial elements of aerobic conditioning, including lung ventilation. Forceful inhalation and deflation of the lungs for prolonged periods leads to strengthening of respiratory muscles. Fatima et al. (2013) added that an increase in the maximal shortening of the inspiratory muscles as an effect of physical exercise has been shown to improve pulmonary function parameters.Garcia-Aymerich et al. (2007) reported that men who remained in the active life style during a 19-month follow-up showed 50 ml improvement in their FEV1 and 70 ml in their FVC, in comparison with subjects who remained in sedentary life style had 30 and 20 ml reduction in their FEV1 and FVC, respectively.Azad et al. (2011) reported a positive association between physical activity, physical fitness and lung capacity. Regular physical activity and good physical fitness have been related to better pulmonary function. Jakes et al. (2002) noted that those who participate in vigorous physical activity have a slower rate of decline in their FEV1. Holmen et al. (2002) found smaller lung capacity among nonsmokers with lower levels of physical exercise. Simões et al. (2010) showed that respiratory muscle strength was significantly low in individuals with sedentary lifestyle. Azad et al. (2011) noted that young subjects with sedentary life style are at a higher risk for deterioration of their respiratory indices and may be at risk for developing chronic obstructive pulmonary disease in adulthood. Hence, appropriate interventions, such as prescribed physical activity programs, may prevent lung function deterioration in these young subjects.In conclusion, low physically activity is a common problem among male Saudi university students. Saudi male university students who have low physically activity have significantly lower pulmonary function parameters than those who have high physical activity.