-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2015; 5(4): 162-170
doi:10.5923/j.sports.20150504.08
The Effect of Kinesio Taping on Vertical Jump Height and Muscle Electromyographic Activity of the Gastrocnemius and Soleus in Varsity Athletes
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIan MacDowall, Paolo Sanzo, Carlos Zerpa
School of Kinesiology, Lakehead University, Thunder Bay, Canada
Correspondence to: Paolo Sanzo, School of Kinesiology, Lakehead University, Thunder Bay, Canada.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Objective: To examine the effect of kinesio tape compared to no tape on vertical jump height and triceps surae electromyographic (EMG) muscle activity in healthy varsity athletes. Design: One group pre-test post-test design. Methods: Twenty healthy varsity athletes (15 females and 5 males) between the ages of 18 and 30 (20.45 years ± 1.36) participated in this study. Each participant was a member of a varsity university basketball, volleyball and/or track and field team. After consent was obtained, the participant completed a Physical Activity Readiness Questionnaire (PAR-Q) and the Waterloo Footedness Questionnaire. The participant then completed a brief warm up and three practice trials of each jump technique. The jumping techniques included the countermovement vertical jump and static vertical jump. The skin at each sensor site was prepped and cleaned and a Delsys Trigno Wireless EMG System was attached to the lateral and medial gastrocnemius, and soleus muscles. After insuring that the EMG sensors were firmly attached, the individual performed a maximal vertical jump and the height of the vertical jump measured using a Vertec device. The participant performed three trials of a one-footed take off using only his/her dominant foot and a two-footed take off maximal countermovement vertical jump and static vertical jump. Each of these jumps were performed with a one footed take off using the dominant leg only, and then a two footed take off using both legs. Kinesio tape was then applied to the dominant leg using a combined taping technique (facilitatory and mechanical corrective). The maximal countermovement vertical jump and static vertical jump height was then re-tested. The mean rectified average EMG signal intensities and vertical jump heights were analyzed. A paired samples t-test was used to analyze the data comparing baseline to post-taping values with an alpha level set at p<.05. Results: There was a significant increase in mean vertical jump height (t(19)=-4.091, p=0.01) for the one legged static jump with the application of tape. The mean one legged static jump height without tape was 26.29 cm ± 9.12, while with tape it was 28.72 cm ± 7.37. There was no significant difference in the vertical jump height for the one legged static, one legged countermovement, or two legged countermovement jumps. There was also no significant difference in the EMG activity across the four jump types for the gastrocnemius or soleus muscles with and without tape. Conclusions: The findings of this study have shown that the application of an Achilles tendinopathy kinesio taping technique increased the vertical jump height during a one legged static vertical jump. A trend of minor improvement was evident in all of the vertical jumps that were performed with tape. It was found that kinesio tape had no effect on EMG activity of the gastrocnemius or soleus muscles. The improvement in vertical jump height demonstrates that the application of kinesio tape may provide an individual with an athletic advantage in sports such as volleyball and basketball where jump height may be advantageous in certain sport specific situations.
Keywords: Taping, Kinesio tape, Vertical jump height, Electromyographic activity, Achilles, Gastrocnemius, Soleus
Cite this paper: Ian MacDowall, Paolo Sanzo, Carlos Zerpa, The Effect of Kinesio Taping on Vertical Jump Height and Muscle Electromyographic Activity of the Gastrocnemius and Soleus in Varsity Athletes, International Journal of Sports Science, Vol. 5 No. 4, 2015, pp. 162-170. doi: 10.5923/j.sports.20150504.08.
Article Outline
1. Introduction
- Overuse injuries and soft tissue and tendon disorders often account for 30-50% of all athletic injuries [20, 27]. More specifically, tendinopathies account for 4% of all patients presenting to sports medicine clinics [27]. The Achilles tendon is the largest and strongest tendon in the body [18] and the common union of the gastrocnemius and soleus muscles inserting into the calcaneus [38]. Despite the tendon being the strongest in the human body and having a high capacity to withstand tensile forces, many individuals suffer from pain and discomfort in this area each and every day resulting in a diagnosis of Achilles tendinopathy [11, 38]. Achilles tendinopathy may be caused by excessive loading and tensile forces, degeneration, or in 2% of the cases by systemic diseases [18, 33]. Pain may be present while the patient is at rest but is more common during movement [12]. Often Achilles tendinopathy is associated with running for moderate and longer distances with the annual incidence in runners being reported to be between 7 and 9% [18] and as high as 18% [27]. Achilles tendinopathy is also associated with jumping tasks and other sports such as tennis, badminton, volleyball, and soccer [18]. Tendinopathy is not only present in the athletic and physically active population, however, and does affect the general population as well [33]. There is no conclusive evidence on the optimal intervention that should be used to treat Achilles tendinopathy [20]. There are a variety of proposed conservative treatments and therapeutic modalities to both prevent and treat Achilles tendinopathy, including therapeutic taping [12]. Taping is purported to have a variety of positive therapeutic effects but there are numerous types of tape made of a variety of materials and different techniques and methods of application; this variability further adds to the lack of clarity on its use and which technique or tape is most effective clinically [29].In the 2008 Beijing Olympics, athletes participating in a variety of sports attributed his/her success to the use of kinesio tape; since that time, its use has greatly gained popularity across many settings [37]. Kinesio tape is a type of elastic therapeutic tape that mimics the thickness and weight of the human skin and can stretch up to 60% of its resting length [22]. It can be used in different settings including both injury rehabilitation and prevention [22]. The non-elastic tape, such as athletic tape and Leukotape, is also commonly used in therapeutic, preventative, and sport settings. Non-elastic tape is advantageous as it supports joints by restricting excessive movement [3]. In comparison to non-elastic tape, kinesio tape increases proprioception, realigns fascial tissue, improves blood and lymph circulation, strengthens weakened muscle, and decreases pain [19, 29, 40].The direction in which the tape is applied can have different effects on the tissue. If the tape is anchored at the origin and laid toward the insertion point, it is proposed that the tape assists in relaxing muscle tone; conversely, if the tape is laid in the opposite direction, from insertion to origin, it is proposed to facilitate the muscle and promote muscle contraction [21]. It has been reported that a combination of techniques using an activation and deactivation method simultaneously may be most effective and actually improve performance [25, 34]. The positive effects of kinesio tape on both physiological and performance factors have been considered to be a possible ergogenic aid to athletic performance by some but the available research as an adjunct to sport performance or injury rehabilitation is limited with contrasting findings.Aguilar-Ferrándiz et al. [2] studied the effect of kinesio taping on venous flow of the gastrocnemius muscle in postmenopausal women. They determined that the application of kinesio tape to the gastrocnemius muscle improved venous symptoms, peripheral venous flow, and overall health, and also decreased pain. It has also been reported that when kinesio tape was applied to the quadriceps muscle, electrical activity and motor recruitment of the muscle increased [36]. Slupik et al. [36] also identified that peak torque at the knee joint significantly improved with the application of kinesio tape. The effect of different kinesio taping techniques on a variety of different injuries, such as lateral epicondylitis and plantar fasciitis has also been examined. It was reported that the application of kinesio tape resorbed visible edema, reduced pain levels, and increased functional abilities in these individuals [41]. Conversely, Aytar et al. [4] studied the effect of kinesio taping on patellofemoral pain syndrome, and found that there was no improvement in knee pain levels. It was also found that there was no change in calf pain when kinesio tape was placed superficially on the triceps surae muscle [28]. Merino-Marban et al. [28] also found an increase in ankle dorsiflexion range of motion when kinesio tape was applied. In addition to the contrasting views on pain reduction, there are also varying results regarding the effects of kinesio tape on other biomechanical factors. Abián-Vicén et al. [1] studied the effect of athletic taping on vertical jumping and found that maximum jump height decreased when tape was applied to the ankle. They also determined that peak vertical force and peak power decreased with tape in comparison to no tape. Koyama, Kato, and Yamauchi [23] also found that vertical jump height slightly decreased with the use of athletic tape versus no tape but that ground reaction force actually increased when athletic tape was administered. Similarly, MacKean et al. [26] examined the effects of five different ankle supports on four performance tasks (vertical jump, jump shot, sprint drill, submaximal treadmill run) in 11 female basketball players and reported that vertical jump height and the overall performance was impaired with the use of ankle supports. Hsieh et al. [17] examined the effects of no tape to two types of elastic tape on the maximal vertical jump height in 31 healthy adults. They reported that the EMG activity increased and that increased ground reaction forces were present with one of the types of elastic tape. There was, however, no change in vertical jump height. The authors proposed that the increased ground reaction forces supported the fact that tape may facilitate muscle contraction capacity during the vertical jumping task. Hang et al. [15] found that the application of Y-strip kinesio taping to the triceps surae resulted in increased vertical jump height. It was also reported that muscle activity of the gastrocnemius and soleus muscles increased with the application of kinesio tape. Similarly, Csapo et al. [6] examined the effects of kinaesthetic tape to no tape on isometric strength and EMG activity of the plantarflexor muscles in 24 healthy volunteers. They reported an increase in strength and EMG activity when the foot was in a fully dorsiflexed position; they concluded that the proposed effects of tape may depend on the joint angle during the activity, functional task, or sport.In some cases the effects of tape did not reduce or improve performance. Kummel et al. [24] examined the effect of a flexible tape applied to the vastus lateralis and medialis muscles on jumping performance and on impulse in 23 subjects assigned to either the control or taping group. Individuals performed two trials of three maximal counter-movement jumps. No significant effect was reported on reaction forces or mean jump height.Schiffer et al. [34] tested 18 healthy elite female track and field athletes (long jump, sprint, heptathlon). Participants were asked to perform a double 1-legged jump with and without kinesio tape. Tape was applied to the gastrocnemius, hamstrings, rectus femoris, and iliopsoas muscles with the muscles placed in a maximally stretched position without traction on the tape. No significant difference was found in jump performance as measured by the distance travelled. Taping is often used for rehabilitation and the prevention of ankle and lower leg injuries, but there is also contrasting research in this regards [1, 26]. When kinesio tape was applied to individuals with a lateral ankle sprain, there was no significant difference in vertical jump height for both males and females [30]. Nunes et al. [31] studied the effect of a Y-strip activation kinesio taping technique applied from the origin to the insertion of the triceps surae (from the knee region to the heel) on vertical jump height. In this crossover randomized controlled trial of 20 athletes, no significant effect was reported when comparing the effects of kinesio tape to placebo on vertical jump height, distance travelled in a horizontal jump test, and dynamic balance tested with the Star Balance Excursion Test.The number of studies actually examining the effect of kinesio tape on vertical jump performance is limited. There are also not a great deal of studies that investigate the effects of kinesio tape on highly active populations, as most studies test healthy, inactive individuals. Therefore, the purpose of this study was to examine the effect of kinesio tape compared to no tape on vertical jump height and triceps surae EMG muscle activity in healthy varsity athletes.
2. Methods
2.1. Subjects
- After ethical approval was obtained, 20 healthy subjects between the ages of 18 and 30 years were recruited using both convenience and purposive sampling. Descriptive data for the sample is summarized in Table 1.
|
2.2. Apparatus
- A Delsys Trigno™ Wireless EMG System was used to collect and process the data. Three hybrid EMG Trigno sensors were used to acquire EMG activity for each muscle group. Standing reach height and maximal jump height was measured using a Vertec device.
2.3. Procedure
- Once the purpose and methodology of the study was explained and consent to participate was obtained, anthropometric measures (height, weight) were taken and recorded.Each testing session lasted approximately 45 minutes. Prior to testing, participants were asked to discontinue the use of body oils or lotions the day prior to the scheduled test time. This ensured that an optimal signal was detected by the EMG electrode device [13]. A Physical Activity Readiness Questionnaire (PAR-Q) and Waterloo Footedness Questionnaire [9, 10] were completed to ensure that he/she was physically able to participate in the study and to determine the dominant leg of the individual. Upon completion of the required questionnaires, the participant completed a brief warm up consisting of cycling on a stationary bicycle at a steady, self-selected, and comfortable speed for five minutes. The participant then completed three practice trials of the jump techniques to insure proper form. The first jumping technique tested was the countermovement vertical jump. With his/her feet placed shoulder width apart, the individual crouched down, bent his/her knees, and hyperextended the arms to approximately 45° behind the torso. The individual then rapidly extended his/her knees and shoulders, jumping as high as possible with maximum force. This movement was performed as one fluent motion. Each of these jumps were performed with a one footed take off using the dominant leg only, and a two footed take off using both legs. The second jumping method tested was the static vertical jump. This jump was similar to the countermovement vertical jump, however, instead of performing the movement in one fluid motion, the individual flexed his/her knees and hyperextended their arms, and then held this position for one second prior to jumping as high as they could with maximum force. The amount of knee flexion for the jumps was controlled by having each individual crouch to a pre-determined height for consistency.After the warm up and practice trials were completed, the individual was connected to the Delsys Trigno Wireless EMG System via wireless EMG sensors. Prior to the application of the wireless sensors, the skin of each sensor site was prepped and cleaned to reduce electrical impedance. The sensors were then applied to three different sites: the lateral gastrocnemius, medial gastrocnemius, and soleus muscles. For landmarking of the lateral gastrocnemius sensor site, the individual lay in prone with the dominant knee extended and foot projecting over the end of the table. The sensor was positioned on the lateral head of gastrocnemius, one third of the distance between the head of the fibula and calcaneus, below the head of the fibula with the sensor pointing in the direction of the muscle fibers as per the Surface ElectroMyoGraphy for the Non-Invasive Assessment of Muscles (SENIAM) guidelines (figure 1) [35]. For the medial gastrocnemius muscle, the sensor was applied to the most prominent bulge of the medial head of the gastrocnemius muscle on the dominant leg parallel to the muscle fibers (figure 2) [35]. For the soleus muscle, the participant sat on the examination table with his/her knee flexed to 90° with the heel of the foot on the table. The electrode was positioned two thirds of the distance between the medial condyle of the femur to the medial malleolus of the tibia, below the medial condyle. The sensor was positioned parallel to the muscle fibers of the soleus muscle (figure 3) [35].
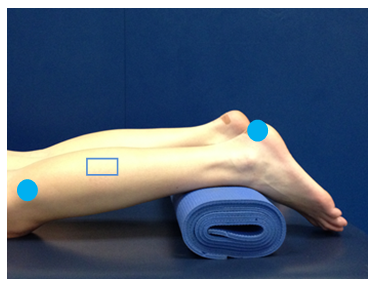 | Figure 1. Lateral gastrocnemius EMG electrode placement location as per the SENIAM guidelines [35]. The  represents the location in which the wireless EMG electrode was positioned on the lateral gastrocnemius muscle represents the location in which the wireless EMG electrode was positioned on the lateral gastrocnemius muscle |
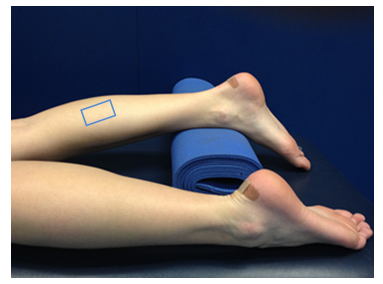 | Figure 2. Medial gastrocnemius EMG electrode placement location as per the SENIAM guidelines [35]. The  represents the location in which the wireless EMG electrode was positioned on the medial gastrocnemius muscle represents the location in which the wireless EMG electrode was positioned on the medial gastrocnemius muscle |
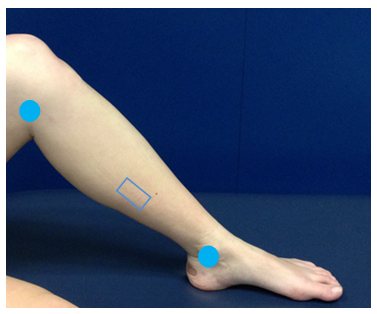 | Figure 3. Soleus EMG electrode placement location as per the SENIAM guidelines [35]. The  represents the location in which the wireless EMG electrode was positioned on the soleus muscle represents the location in which the wireless EMG electrode was positioned on the soleus muscle |
 | Figure 4. Kinesio tape I-strip anchored from the calcaneal fat pad distally to the proximal end of the musculotendinous junction |
 | Figure 5. Kinesio tape I-strips anchored from the medial and lateral femoral condyles proximally to the calcaneal fat pad distally |
2.4. Signal Processing and Analysis
- Descriptive statistics were used to compare means and standard deviations of the mean EMG values and vertical jump heights. Two independent variables (tape intervention and type of jump) and two dependent variables (mean EMG activity measured in μV and maximum vertical jump height measured in centimeters) were examined. The data were analyzed using paired samples t-tests to examine the effect of the taping intervention on the dependent variables for each type of vertical jump. The rejection criteria was set with an alpha level <.05.
3. Results
- The mean one legged static jump height without tape was 26.29 cm ± 9.12, while with tape it was 28.72 cm ± 7.37. The difference between the pre- and post-taping intervention was 2.43 cm. This demonstrated a significant increase in mean vertical jump height (t(19)=-4.091, p=0.01) for the one legged static jump.There were no significant differences in vertical jump height for the two legged static vertical jump, one legged countermovement jump, and two legged countermovement jump. Although the only significant increase in vertical jump height occurred during the one legged static jump, there was an overall increase in each of the four vertical jump types with the application of tape as seen in figure 6.
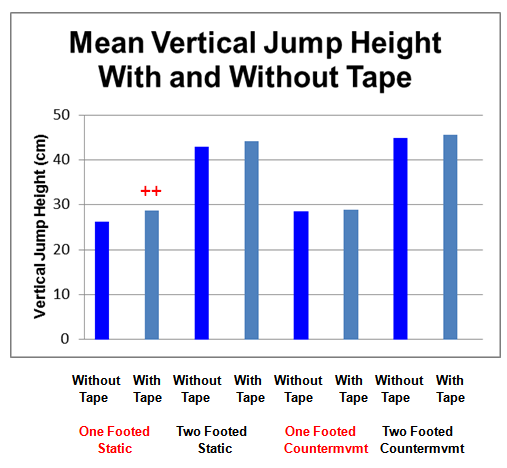 | Figure 6. Mean vertical jump heights (cm) with and without tape for each jump type (  - vertical jump without tape; - vertical jump without tape;  -vertical jump with tape; -vertical jump with tape;  - denotes statistical significance) - denotes statistical significance) |
|
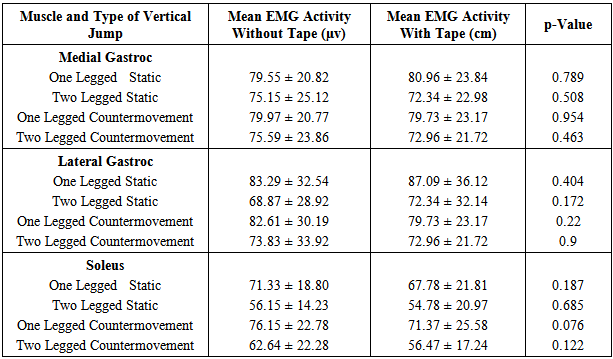
4. Discussion
- This study examined the effects of kinesio tape compared to no tape on vertical jump height and triceps surae EMG muscle activity in healthy varsity athletes. The results showed that vertical jump height significantly increased during the one legged static vertical jump with the application of kinesio tape compared to no tape. There was no significant difference in the vertical jump height with tape for the two legged static, one legged countermovement, or two legged countermovement jumps. There was also no significant effect on EMG muscle activity of the medial gastrocnemius, lateral gastrocnemius, or soleus muscles for any of the four jump types.Opinions about the reported effects of kinesio taping on physical performance measures such as vertical jumping ability and EMG muscle activity are inconsistent in the limited literature available. Previous research examining the effect of kinesio tape on muscle activity found that the tape had no effect on muscle activity in young athletes [14] or decreased muscle activity [16]. However, it has also been identified that kinesio tape increased EMG activity [6, 15, 17, 36]. As the reported results vary across a wide spectrum, trying to compare each of these different studies is extremely difficult due to methodological inconsistencies, different types of tape used, and different methods of application. Many studies have used poor methodological designs or lack pertinent information to clarify exactly what type of tape or technique was used. Each of these variables may greatly impact on the reported findings.With regards to the longer term follow up, the participants in the present study performed the jumping trials immediately after the kinesio tape was applied. It has been reported that the motor units of the muscle may be maximally increased 24 hours after the application of kinesio tape [36]. As a result, this may have impacted on the EMG muscle activity and limited the effect that the kinesio tape had on the muscle activity of the gastrocnemius and soleus muscles.Throughout the study, the distance that participants squatted down in preparation for their jump was controlled and standardized. This may have affected the technique used by participants altering their normal jumping mechanics and affecting the stretch-shortening cycle of the individual’s muscles [6]. In turn, this may have also affected both the vertical jump height and EMG activity. In addition, the application of tape to the ankle may have limited the amount of dorsiflexion range at the ankle and in turn, greater flexion may have occurred at a more proximal joint (i.e., knee, hip, lumbar spine). This may have resulted in greater EMG muscle activity in a more proximal muscle (i.e., quadriceps, gluteus medius, erector spinae). The greater range of motion and increased muscle activity proximally may have assisted with generating more momentum and force resulting in a greater vertical jump height. This may also explain why there was not a significant increase in EMG activity in the calf musculature and may an important consideration for future studies to incorporate analysis of the distal and proximal musculature.Although it has been reported that kinesio tape can have positive physiological effects such as increased venous flow [2] and quadriceps muscle strength [36], there is a lack of evidence that kinesio tape has any benefits on other muscles. Drouin et al. [8] reported that kinesio tape had no significant effect on muscle strength of the masseter and wrist flexor muscles. They also found that there was no significant difference in nerve conductivity in the forearm. It is evident that there is contrasting findings when it comes to the benefits of kinesio tape regarding pain and strength changes; the effects may depend on the specific muscle that the tape is applied to. Jumping is an important aspect of many sports such as basketball, volleyball, and track and field. Athletes in these sports rely on the vertical jump in order to achieve optimal performance, which is why the vertical jump is often used to test an individual’s physical fitness and lower extremity performance capacity [17, 39]. The vertical jump is carried out through rapid extension of the hip, knee, and ankle joints [5] and it is a complex motor skill that involves several muscles including the quadriceps and triceps surae with each muscle influencing performance [31].The contradictory findings on the effect of tape on vertical jump height and EMG activity may be due to the orientation of the kinesio tape and the direction that the tape is laid. The difference in the direction that the kinesio tape is applied may be the reason that the EMG results from the current study vary from previous research. As previously mentioned, the only statistical difference in vertical jump height occurred in the one legged static vertical jump. However, a distinct trend was observed as there was a minor increase in jump height for each of the jump types. In the sporting world, any small increase in jump height counts as even a millimeter may be advantageous. A small improvement in vertical jump height after the application of kinesio tape is beneficial to an athlete, especially in a sport such as volleyball or basketball where that height improvement can be the difference between making the block or not. Therefore, even these minor enhancements in vertical jump height can provide an athletic advantage to the competitor.Some of the limitations of the current study are related to the design of the study. A one group pre-test post-test design was used and future studies should incorporate the addition of a control group, placebo group, or a comparator group using different types of tape to minimize treats to the internal validity of the data. A larger sample size with longer follow up as well may further add to the strength of the findings supporting the use of therapeutic taping.Based on the research available to date, there are various gaps in the literature. While the current research only included healthy individuals, the outcome is useful to establish normative data on the use of Kinesiotape to improve vertical jump performance. From the clinical perspective, future research using a symptomatic population with Achilles tendinopathy may be beneficial and demonstrate added value to the body of literature available to clinicians. It would also be valuable to measure the effect of therapeutic taping on EMG activity of the larger muscles in the upper leg, as well as the lower leg, to determine if this taping technique has any influence on the quadriceps, hamstring, and gluteal muscles. Most studies also do not examine longer term outcomes and cost effectiveness. Longer follow up or periods of application time may provide further understanding into the use of therapeutic taping and further clarify some of the mixed results in the available literature. The effect of tape on other sport specific or performance measures may be another area that further research is required.
5. Conclusions
- Kinesio tape is a popular therapeutic intervention that is often used to prevent and treat many conditions such as Achilles tendinopathy. It has been reported to have various effects on different physical, physiological, and sport specific aspects such as vertical jump height and EMG activity. The findings of this study have shown that the application of kinesio tape increased vertical jump height during a one legged static vertical jump. A trend of minor improvement was evident with all of the vertical jumps that were performed. Kinesio tape had no effect on EMG activity of the gastrocnemius or soleus muscles.The improvement in vertical jump height demonstrated that the application of kinesio tape may provide an individual with an athletic advantage in sports such as volleyball and basketball where jump height may be advantageous in certain sport specific situations. Further study is required, however, to examine the effects on a larger or symptomatic sample.