-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2014; 4(4): 130-135
doi:10.5923/j.sports.20140404.02
Tai Chi for Subjectively Perceived Health of the Elderly
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLHung Manh Nguyen1, Duong Dai Nguyen2
1Faculty of Sport and Physical Education, Vinh University, 182 Le Duan, Vinh city, Nghe An, Vietnam
2Bac Ninh Sport University, Trang Ha, Tu Son, Bac Ninh, Vietnam
Correspondence to: Hung Manh Nguyen, Faculty of Sport and Physical Education, Vinh University, 182 Le Duan, Vinh city, Nghe An, Vietnam.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Objective: Evaluating the effects of Tai Chi exercise on subjectively perceived health of community-dwelling elderly. Design: A randomized controlled trial. Setting: Community-dwelling elderly in Vinh city, Vietnam. Participants: Ninety- six community-dwelling participants aged 60 to 79 years (68.9 ± 5.1 years) were recruited. Intervention: Subjects were divided randomly into two groups: Tai Chi and Control groups. Participants in the Tai Chi group (aged 69.02 ± 5.16 years) attended a 60-minute Tai Chi practice session twice a week for 6 months. The session consisted of a 15-minute warm-up and a 15-minute cool-down period. The Control group (aged 68.72 ± 4.94 years) maintained routine daily activities. Outcome measures: The Short-Form 36 (SF-36) is primary outcome measure. Results: After 24 weeks of the Tai Chi training program, the intervention group showed significant better results than coutrol group. Age, Sex, Education are not predictors for scores of short form 36 between Tai Chi and Control but only Group is a prominent predictor. Conclusion: In this randomized controlled trial study, Tai Chi is beneficial to improve subjectively perceived health of the elderly. Assessment of the effects of Tai Chi may be focused more on chronic disease with a long-term training program in the future.
Keywords: Elderly, Mental health, Physical health, Tai Chi, Vietnam
Cite this paper: Hung Manh Nguyen, Duong Dai Nguyen, Tai Chi for Subjectively Perceived Health of the Elderly, International Journal of Sports Science, Vol. 4 No. 4, 2014, pp. 130-135. doi: 10.5923/j.sports.20140404.02.
Article Outline
1. Introduction
- With increasing age, health and the health-related to quality of life tend to decline. This process is especially pronounced beyond an age of around 60 year. It manifests itself in the form of a higher incidence and prevalence of certain diseases and also through more severe symptoms of some of the diseases which occur in other age group as well (Pfaff, 2009). It has been well-documented that many physical changes and psychological changes are associated with aging (Shephard, 1997). Exercise can improve cardiovascular function; reduce risk factor of cardiovascular disease, lead to strength improvement, balance and flexibility. Moreover, the psychological functions like cognitive such as memory, depression, perception of control of the elderly are also improved (Mazzeo, et al., 1998). Tai Chi appears to improve physiological function and fear of falling in the elderly (Zhang, Ishikawa-Takata, Yamazaki, Morita, & Ohta, 2006), self-efficacy (Li, et al., 2001). Tai Chi exercise also has an effect on pain, balance, muscle strength, and perceived difficulty in physical functioning (Song, Lee, Lam, & Bae, 2007). A self-paced and self-controlled activity such as Tai Chi has the potential to be an effective, low-cost means in improving functional status in older persons (Li, et al., 2001). Furthermore, Tai Chi participants tended to have a lower rate of falls. It is also concluded that Tai Chi is a balanced exercise that integrated key components of modern exercise training. Tai Chi is beneficial to psychological and physiological functions. Additionally, Tai Chi can be prescribed as an alternative exercise program for selected patients with cardiovascular, orthopedic or neurological disease, and can reduce the risk of falls in elderly individuals (Lan, Lai, & Chen, 2002). It showed in another study that a six month program of Tai Chi Chuan afforded a significant improvement of performance of memory complaints in the elderly with mild cognitive impairment (Kasai, et al., 2010). Moreover, a number of excellent review articles exist showing evidence that Tai Chi generates various health benefits for individuals of varying age groups and patient populations (Lan, et al., 2002; Li, Hong, & Chan, 2001; Wang, Collet, & Lau, 2004; Wayne, et al., 2004; Wu, 2002). Significant psychological benefits were also observed, such as better perceived social support and mood state and superior relaxation among Tai Chi practitioners (Lee, Lee, & Woo, 2007; Taylor-Piliae, Haskell, Waters, & Froelicher, 2006). To review the physiological and psychological effects of a 12-week Tai Chi program in patients with heart failure, Yeh (Yeh, et al., 2008) reported that Tai Chi may enhance quality of life, exercise capacity, and sleep stability in patients with chronic heart failure. By using the Short Form-36 and exploring eight indicators related quality of life (Ware & Sherbourne, 1992), the specific problems, per health-related quality of life indicator, can be identified. To date, the aging population tends to increase in Vietnam. It would be necessary to find ways and measures to maintain or improve the normal physical functioning and mental health of the elderly. There are many people living in community-dwelling in Vinh City engaging in Tai Chi. However, there have not been comprehensive systematic studies deal with effects of Tai Chi on subjectively perceived health of the elderly.
2. Material and Methods
2.1. Design
- A randomized, controlled trial: One hundred two subjects were recruited. Six subjects did not the meet exclusion criteria MMSE (>24). Subjects were divided randomly into two groups, Tai Chi group and Control group. The subjects were expected to consent and volunteer. Participants in Tai Chi group (n=48, mean (M) age = 69.2 years, standard deviation (SD)=5.3) were assigned 6-months Tai Chi training. Participants in the control group (n=48, M age = 68.7, SD = 4.9) were instructed to maintain their routine daily activities. Based on the previous findings (Li, Duncan, McAuley, & Harmer, 2002; Li & Manor, 2010) with the standardized mean difference of the group means, alpha level = 0.05, desired statistical power = 0.8, effect size is set at medium (ES=0.5). Experienced Tai Chi instructors were selected by investigators to teach class. Tai Chi exercise is 24-form style incorporating elements of balance, postural alignment and concentration.Participants in the Tai Chi group attended a 60-minute Tai Chi practice session twice a week for 6 months. The session consisted of a 15-minute warm-up and a 15-minute cool-down period. Participants in Control group were instructed to maintain their routine daily activities. Short Form-36: The Short Form-36 was used to assess the changes of physical and mental health (Ware, Kosinski, Keller, 1994). The questionnaire of SF-36 (Vietnamese version) was used with permission from Watkins et al (2002). A questionnaire was used to assess and self-report health status. The questionnaire was administered in Vietnamese by trained Vietnamese interviewers. Translation of the United States version of the SF-36 was performed by two independent translators using forward and backward translation methods (Watkins, Plant, Sang, O'Rourke, & Gushulak, 2002).
2.2. Statistical Analysis
- All statistical analyses were conducted using the statistical package for the social science (Statistical Package for Social Sciences, 2005). The statistical significance has been estimated at probability (p-value) equal or less than 0.05. Data are expressed as means ± standard deviation. The completely randomized design (Analysis of variance; ANOVA) was used to determine defferences of varibles and identified for included; One-way ANOVA is to compare all variables of subjects, expecially subjects’ages, and parametes between subjects.
3. Results
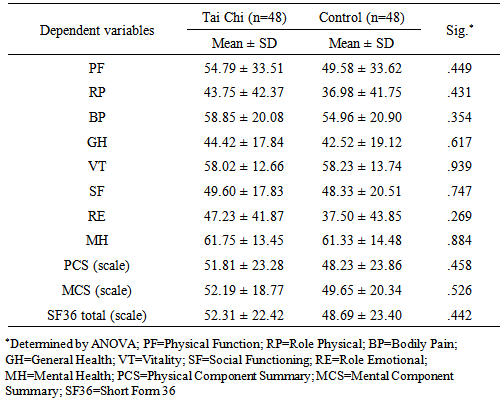
- Comparison between Tai Chi and Control groups at three phases of interventionThere is no significant difference between the two groups of intervention for subjectively perceived health with p-values of all dependent variables are greater than 0.05 (p>0.05) (table 1). Statistical results of one-way Anova showed Physical function [F(1, 94) = .578; p > .05]; Role physical [F(1, 94) = .624; p > .05]; Body pain [F(1, 94) = .867; p > .05]; General health [F(1, 94) = .252; p > .05]; Vitality [F(1, 94) = .006; p > .05]; Social functioning [F(1, 94) = .105; p > .05]; Role Emotional [F(1, 94) = 1.238; p > .05]; Mental health [F(1, 94) = .021; p > .05]; Physical component summary F(1, 94) = .555; p > .05; Mental component summary F(1, 94) = .404; p > .05; Short form 36 [F(1, 94) = .595; p > .05, respectively.
|
|
|
|
|
|
4. Discussion
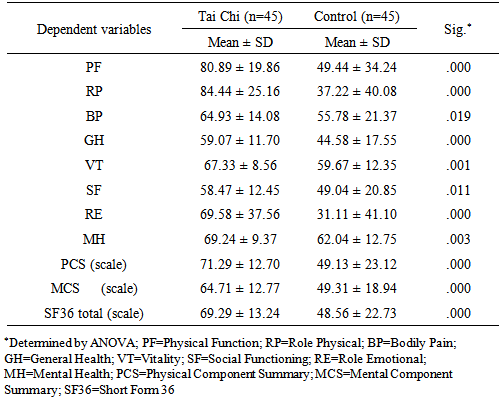
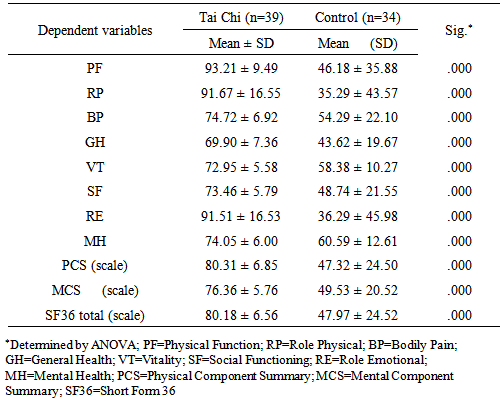
- Tai Chi has been widely practiced in Asia and Europe. It is believed to bring benefits in physiological and psychological aspects. The study process consisted of three main phases: baseline, midpoint and endpoint. Samples of study were recruited from community-dweller in Vinh city. To compare the benefits of Tai Chi exercise, we recruited older people aged from 60-79, which included 96 participants divided into two groups: Tai Chi and Control groups.In this study, we examined the effects of 24-form Tai Chi exercise for six months on perceived health of older people living in a dwelling community. There are highly significant changes between the Tai Chi group and Control group at midpoint and endpoint. Results of the study proved that Tai Chi has strong effects on mental health of older adults. Participants in the Tai Chi group have the advantages in achieving better levels of mental aspect as shown in the SF-3 than their counterparts.Compared with participants in the Control group, Tai Chi participants showed significant improvements on all physical and mental scores of SF-36. Higher mental summary scores of Tai Chi group may due to the program that offers participants an opportunity to communicate and interact socially. These findings are consistent with the other findings that psychological benefits were observed with Tai Chi exercise, such as better perceived social support and mood state and superior relaxation among Tai Chi practitioners (Lee, Arthur, & Avis, 2007; Taylor-Piliae, 2004) and significant improvements for quality of life dimensions such as general health perception, social functioning, vitality, and mental health or psychological well-being (Abbott, Hui, Hays, Li, & Pan, 2007). From a behavioral - immunological perspective, Tai Chi has been found to be associated with significantly decreased sympathetic nervous system activity (Motivala, Sollers, Thayer, & Irwin, 2006). Based on previous studies, we may know that Tai Chi enhance physiological well-being and improve cardiopulmonary functions which are both related to quality of life (Ko, Tsang, & Chan, 2006; Kutner, Barnhart, Wolf, McNeely, & Xu, 1997; Wang, et al., 2004; Zeeuwe, et al., 2006). Tai Chi can improve the quality of life among the elderly (Ho, et al., 2007) and its characteristics are highly relevant for promoting health among older people particularly effecting to nursing home residents (L. Y. Lee, Lee, & Woo, 2009). Tai Chi also appears to lead to improved physical status (Wolf, Barnhart, Ellison, & Coogler, 1997). Over the 6-month Tai chi program, there was a 18.75% drop-out rate in the Tai Chi group. It is evident that relatively high rate of participants were likely to engage in Tai Chi training. The attrition of participation was due mainly to travelling or leaving the city rather than dissatisfaction with the training program. Tai Chi is a low - technology exercise that can be easily carried out in variety of communities.The study has a small sample size, a low-frequency training schedule of only twice per week. Furthermore, we have used two research groups, while the Tai Chi group received treatment but the control group did not. The social effects and biased opinions resulting from individuals in both groups might be raised. It should be, therefore, comparative design that account for equal condition of intervention. Moreover, all participants come from urban areas which may not be representative for the whole Vietnamese population.
5. Conclusions
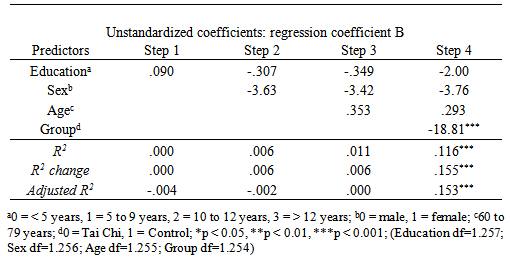
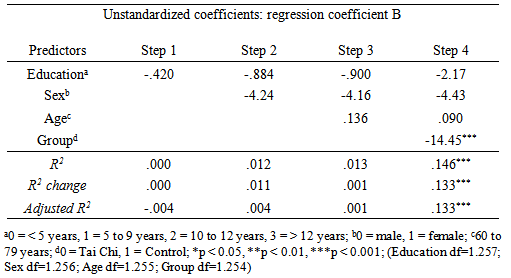
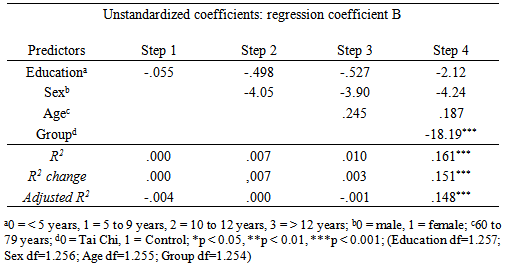
- In this randomized controlled trial study, results showed that a 24 week Tai Chi program can be an alternative form of exercise for older adults. The 24-form Tai Chi brings physical and psychological benefits to older adults. The scores of self-report health in the two domains of Short form 36 of Tai Chi group were better than the Control group. It showed that physical and mental health was much improved after the Tai Chi training. It also enhances and promotes the older adults to participate in Tai Chi in public. Tai Chi exercise is meaningful to promote the healthy elderly not only people living in dwelling communities but also in nursing homes or people with chronic diseases to participate in. In the hierarchical regression models, only Group is a prominent predictor for three depentent varibles (General health component summary, mental component summary, and physical component summary). This strongly proved that Tai Chi have good effect for mental and phycal health of the elderly.
ACKNOWLEDGMENTS
- This work was supported by grant no. 3612/QD-BGDDT from the Vietnam International Education Development; and Tai chi club in Vinh city, Vietnam.
Disclosure
- There are no conflicts of interest in this work. The study sponsors played no role in the study design, collection and analysis of data, writing of the manuscript, or decision to submit the manuscript for publication.