-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2014; 4(3): 115-120
doi:10.5923/j.sports.20140403.06
Effects of Swimming Technique Backstroke on Lumbar Lordosis and BMI in Females
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMahnaz Manshouri 1, Nader Rahnama 2
1Physical Education Center, Isfahan University of Technology, Isfahan, 84156-83111, Iran
2Department of Physical Education, University of Isfahan, Isfahan, Iran
Correspondence to: Mahnaz Manshouri , Physical Education Center, Isfahan University of Technology, Isfahan, 84156-83111, Iran.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
The present paper aims to investigate the effects of incremental backstroke exercise on lumbar lordosis in non-athlete young females. Materials and Methods: For the purposes of this study, 98 healthy volunteer female, university students with hyperlordosis were selected and divided into an experimental group of 44 subjects (with an average height of 163.52 cm, an average age of 19.25, and an average weight of 62.35 kg) and a control group of 33 subjects (with an average height of 159.78 cm, an average age of 19.3, and an average weight of 61.33 kg). The remaining volunteers were excluded for failure to meet requirements. The subjects in the experimental group participated in three weekly sessions of backstroke exercise over the eight weeks of the study period while the control group received no specifically designed exercise. Lordosis was measured in the subjects using a flexible ruler and their BMIs were determined based on their heights and weights before and after the intervention. The data thus obtained were subjected to COANOVA analysis at a significance level of p≤0.05. Results: The results of the present study indicate that backstroke exercise significantly reduced (p<0.05) the increased lordosis in the subjects while no significant effect was observed with respect to their BMI. Conclusions: The improved lumbar lordosis observed in this study may be ascribed to the strengthened spinal extensor muscles and the stretch of hip flexor and iliopsoas muscles. Another finding is that the 8-week backstroke exercise, especially given the incremental swimming provisioned, had no effect on the subjects’ general body composition.
Keywords: Backstroke, Swimming, Lumbar, Lordosis, BMI
Cite this paper: Mahnaz Manshouri , Nader Rahnama , Effects of Swimming Technique Backstroke on Lumbar Lordosis and BMI in Females, International Journal of Sports Science, Vol. 4 No. 3, 2014, pp. 115-120. doi: 10.5923/j.sports.20140403.06.
Article Outline
1. Introduction
- The spinal column may be regarded as the most important skeletal element in the human physique [1]. Any imbalance in the length or power in lumbar muscles leading to atrophy in some and to shortened length in others will lead to abnormalities in spinal curvatures including hyperlordosis in the spinal column [2]. Posture is defined with reference to the curvatures of the spinal column [3]. The spinal and pelvic muscles are the elements that are involved in keeping constant balance in the standing position; thus, physical weakness, improper exercise, and inappropriate movements such as pushing or pulling objects in the wrong manner will lead to imbalances in body conditions with the consequent imbalanced posture [4, 5].Hyperlordosis, is closely related to pelvic and sacral vertebrae; it is also affected by lumbar extensors, lumbar fascia, lumbar musculature, hip flexors; and the hamstring muscle group [6]. Psoas includes of two psoas major and psoas minor. The iliac is independent of the psoas muscles. The two muscles are considered as one and collectively called ‘iliopsoas’ or pelvic psoas. The gluteus maximus is the most effective muscle in the pelvis. The hamstring muscle is the one in the posterior part of the lower limb which is in the opposite direction to the iliopsoas and the flexor of the lower limb causing pelvic rotation [7]. Despite their important interrelations, the functions of the musculature in the lordotic and pelvic regions have not been adequately investigated [1].A number of studies have so far been conducted on the effects of different exercises on pelvic tilt posture, especially the lumbar lordosis. Daneshmandi (2005) proposed an exercise program for correcting the lumbosacral angle in male students and found that his program led to reduced lumbar lordosis [1]. Farahani (2012) found that corrective exercises significantly increased the power and strength of abdominal musculature and the flexibility of spine extensors, reducing lumbar lordosis [3]. Levine (1997) investigated the effects of an abdominal musculature strengthening exercise on 20 subjects in two control and experimental groups. His 8-week program resulted in increased abdominal strength but no significant differences were observed between lumbar lordosis and pelvic tilt in the two control and experimental groups [8]. Beato (2013) subjected adults with acute backache to an 8-week aquatic therapy (2-3 days a week) and found that his program led to reduced back pain, improved life quality, enhanced physical fitness, and improved body composition [9]. Hofling (2012) used both radiography and the radius method to measure lumbar lordosis in the three standing, breaststroke, and backstroke positions. He found that lumbar lordosis was greater in the standing position than in the swimming positions and that it was greater in the backstroke than in the breaststroke [10]. Ghadimi Ilkhanlar (2010) observed a significant reduction in kyphosis in his subjects after 6 weeks of alternating backstroke exercise [2]. Little is known about the effect of swimming o lumber lordosis. The purpose of this study was to investigate how backstroke swimming may change lumber lordosis of females. In this research non-athlete volunteer female were chosen so that the effect of exercise can be measured more easily in this. Scholars believe that weight gain and obesity increase the force exerted on the spinal column and this overload causes alterations in the column [3]. Vismara showed that obesity reduced the overall movement domain of the spinal column, which leads to the reduced movement domain of the pelvic and thoracic vertebrae. He also maintained that obesity associated with chronic back pain was closely related to increased lordosis [11].In 1832, BMI (Body Max Index) was first introduced as a natural human body index and defined as weight (kg) divided by height squared (m2) expressed as kg/m2, along with a description of human body part proportions [12].The relationship between aquatic exercise and body weight control is yet to be known. However, while some studies have indicated the effect of aquatic exercise on BMI, others have shown no such relationship. Rica (2013) investigated the effects of aquatic exercise on certain parameters in senior, obese females and concluded that aquatic exercise had no effects on the studied anthropometric parameters but it certainly increased the aerobic capacity, muscular power, and life quality of his subjects [13]. Cavalcante et al (2009) investigated the effects of aquatic aerobic exercise on pregnant, non-athlete females and found that the exercise had no effect on their body composition, delivery, or number of childbirths [14]. Aquatic exercise in a study by Cadmus et al (2010) revealed that it had positive effects on obese people with a BMI≥30 but had no effects on subjects with normal BMI and weight [15].Swimming is most often recommended as a preventive measure or a remedy for many diseases [10]. It is also established that swimming activates the musculature of both the trunk and the lower body parts [2]. Swimming involves almost all body muscles due to activity under conditions where water resistance must be overcome. This seems to strengthen weak muscles by favorably involving the muscles supporting the spinal column.The present study aims to investigate the effects of backstroke swimming on lumbar lordosis and BMI in healthy, non-athlete female subjects who participated in this experiment on a voluntary basis.
2. Research Methodology
- The experiment is a field study in which 156 volunteered female university students took part in a preliminary screening test of lumbar lordosis. The subjects were asked to stand against the wall with the head, shoulders, hips, and heels touching the wall surface. The examiner would then measure the space between the lordosis and the wall by palpation. In cases where the examiner’s hand would pass through the space without friction, the subject would be judged as one with increased lumbar lordosis and identified as potential participant in subsequent tests. In this way, 98 subjects were selected for further tests. After the subjects filled out physical health questionnaires and signed a disclaimer form approved by the IUT University Office of Human Research Ethics Committee, indicating their consent to take part in the study, they were divided up into an experimental and a control group of 64 and 34 subjects. The criteria employed for inclusion in the experimental group consisted of basic swimming and floating skills as well as readiness to attend three sessions of exercise on a weekly basis. The program for the experimental group involved a special backstroke exercise in each session throughout the study period while the control group performed a general exercise with no specifically designed program. The protocol approved by the IUT University Office of Research. Lumbar lordosis was then measured using a flexible ruler together with the subjects’ height and weight. The reliability of the flexible ruler has already been established in previous studies [16, 17]. In the present study, the curvature between L1 to S1 was measured using a flexible ruler and the formula
 was used to calculate the curvature angle. L is distance between L1 and S1, H is the distance between the midline of L and the deepest part of the curve [16, 18]. The same measurements were made for the control group before the exercise program was commenced. The exercise was administered three sessions a week during the 8 weeks of the study period. The subjects in the experimental group would not be allowed to engage in any exercise during the study period other than the backstroke program designed for the purpose but their other daily habits and activities were not taken into consideration. Increasing the swimming distance was accomplished gradually and according to the program in Table [1]. The experimental group implemented their exercise program over a period of eight weeks with three sessions of 50 to 90 minutes each week. The participants were examined to ensure their skills in backstroke swimming and inadequacies were remedied before the actual program started. The program consisted of the following parts:Stage 1: Participants would perform stretching exercises, walking in water, and slow swimming for 5 to 10 minutes.Stage 2: In this stage, the subjects would perform the 200-m backstroke swimming for 10 minutes in a number of sets. Swimmers would take 5-minute breaks between each two sets. In order to avoid likely damages due to continued exercises, increments in exercises were designed to take place at two-week intervals such that the subjects in the experimental group performed two sets of 200-m backstroke swimming in weeks 1 and 2, three sets in weeks 3 and 4, 4 sets in weeks 5 and 6, and 5 sets of backstroke swimming in the last two weeks (Table 1).
was used to calculate the curvature angle. L is distance between L1 and S1, H is the distance between the midline of L and the deepest part of the curve [16, 18]. The same measurements were made for the control group before the exercise program was commenced. The exercise was administered three sessions a week during the 8 weeks of the study period. The subjects in the experimental group would not be allowed to engage in any exercise during the study period other than the backstroke program designed for the purpose but their other daily habits and activities were not taken into consideration. Increasing the swimming distance was accomplished gradually and according to the program in Table [1]. The experimental group implemented their exercise program over a period of eight weeks with three sessions of 50 to 90 minutes each week. The participants were examined to ensure their skills in backstroke swimming and inadequacies were remedied before the actual program started. The program consisted of the following parts:Stage 1: Participants would perform stretching exercises, walking in water, and slow swimming for 5 to 10 minutes.Stage 2: In this stage, the subjects would perform the 200-m backstroke swimming for 10 minutes in a number of sets. Swimmers would take 5-minute breaks between each two sets. In order to avoid likely damages due to continued exercises, increments in exercises were designed to take place at two-week intervals such that the subjects in the experimental group performed two sets of 200-m backstroke swimming in weeks 1 and 2, three sets in weeks 3 and 4, 4 sets in weeks 5 and 6, and 5 sets of backstroke swimming in the last two weeks (Table 1).
|

3. Research Findings
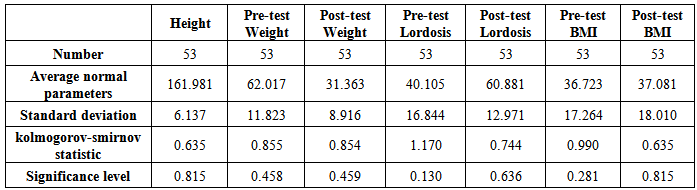
- The results of normality test are presented in Table (2). Clearly, the significance level of the kolmogorov-smirnov test is 5%. This indicates that the parametric tests can be used.
|
|
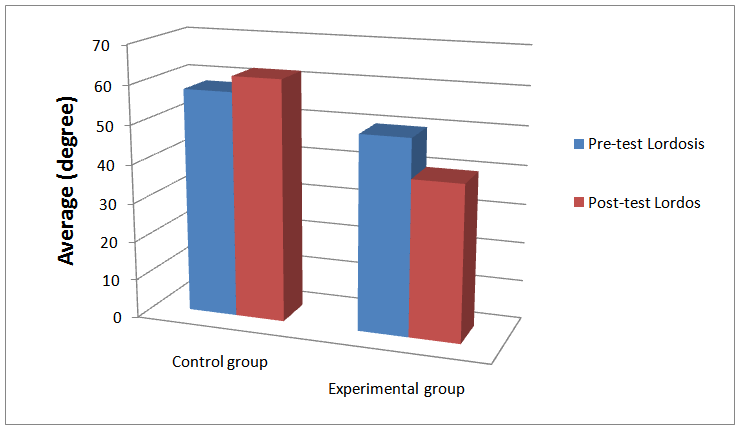 | Figure 1. Pre-test and post-test lordosis means and standard deviations in the two experimental groups |
|

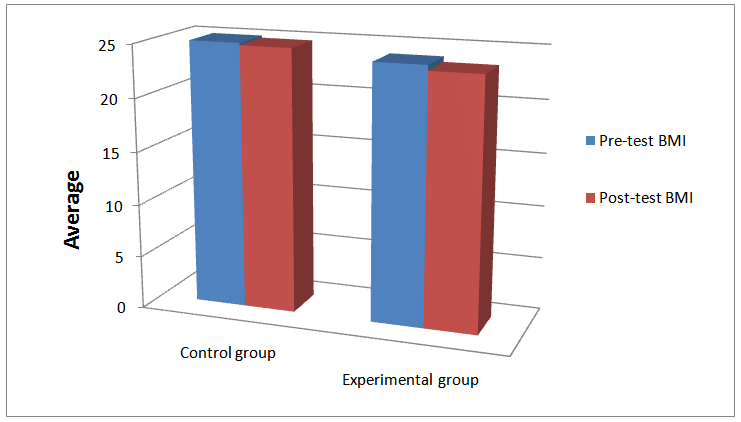 | Figure 2. Pre-test and post-test BMI mean values and the standard deviations in the two experimental groups |
4. Discussion
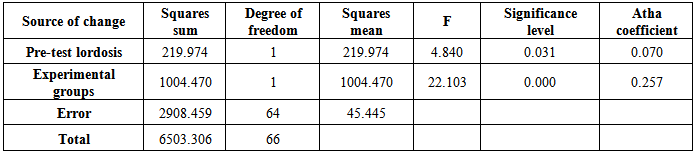
- The objective of this study was to investigate the effects of an 8-week incremental backstroke exercise on lumbar lordosis. The results obtained revealed the significant effect of the exercise on reducing lumbar lordosis in the subjects. This finding is in agreement with those reported by Daneshmandi who claimed that his protocol reduced lumbar lordosis in his subjects [1]. Backstroke swimming is associated with more strokes on the posterior side of the body which strengthens the posterior muscles and is especially accompanied by more effective and greater activity of the hamstrings. Also strengthen the agonist muscles and enhance the flexibility of antagonist muscles [2].The movements of rectus femoris and hamstrings are related. During the extension, these muscles will take opposite roles so that the hamstring will become the agonist and the rectus femoris will become the antagonist. Also, these same muscles will be in coordinated action with knee movements.The iliopsoas is the most important postural muscle and is gradually shortened due to normal daily life activities. Muscle becomes flexible by the kicks during backstroke swimming. The extensors and spine musculature also contribute to increased lordosis as a result of weakening. Again, backstroke swimming can strengthen these muscles to improve and reduce lumbar lordosis. Clinical evidence indicates that lumbar lordosis is associated with such factors as reduced strength of abdominal musculature; lack of flexibility in the trunk and hamstring muscles; weak posture during sleeping, sitting, standing, or walking positions; bad habits of lifting objects; and poor capability of facing anxiety [19].It can, therefore, be claimed that backstroke swimming, especially the backstroke kick, reduced lumbar lordosis in the subjects probably because of the contraction of the extensor muscles, the stretching of the flexor thigh muscles, and the strengthening of the trunk and abdominal musculature [20]. Our findings are in agreement with those of Farahani [3] and Levine [8].Examination of pre-test and post-test BMI scores revealed that backstroke exercise had no significant effect on the subjects’ BMI scores (P≤0.05). This finding is in agreement with the report by Rica who studied the effect of aquatic exercise on senior, obese females. Cavalcante [14] also studied the effect of aquatic aerobic exercise on female subjects and obtained similar results. Cadmus [15] designed an aquatic exercise program and found that the program had no effect on subjects whose BMI scores were normal to slightly high, which confirms the results obtained in the present study.
5. Conclusions
- The subjects in the present study included female, non-athlete university students who were in good health conditions but with minor lumbar lordosis deformity. The results of the study revealed that the incremental backstroke exercise had a positive effect on improving the deformity investigated so that lumbar lordosis was reduced in the experimental subjects.It was also found that the incremental backstroke exercise had no effect on BMI in the experimental group, nor did it bring about any changes in their body composition although it cannot be definitively claimed that the exercise had the same effect on both slim and fat subjects alike.
6. Recommendations
- Future studies may focus on the effects of backstroke swimming on other physical abnormalities and their interrelationships. As the exercise designed for this study seemed to be effective with even fewer sessions, mid-term measurements and tests are also suggested to be accomplished to determine mid-range effects.