-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2013; 3(6): 193-197
doi:10.5923/j.sports.20130306.02
Convergent Validity of Skinfold Thickness and the Hand-held Bioelectrical Impedance Analyzer using Current FITNESSGRAM Standards
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRyan Burns, James Hannon, Brett Allen, Timothy Brusseau
Department of Exercise and Sport Science, University of Utah, Salt Lake City, Utah, U.S.A
Correspondence to: Ryan Burns, Department of Exercise and Sport Science, University of Utah, Salt Lake City, Utah, U.S.A.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Given the limitations of BMI, low-cost alternatives are needed to accurately and efficiently estimate adiposity in physical education classes. The purpose of this study was to examine the convergent validity between the Omron HBF-301 BIA device (BIA) and skinfold thickness assessment (SKF) in middle-school students using current FITNESSGRAM standards. Body composition was assessed on 134 students from the 6th-8th grades. SKF consisted of averaging three skinfolds measurements at two sites (tricep, calf) using gender-specific Slaughter equations to estimate percent body fat (%BF). BIA required entering physical characteristics into the analyzer then having students hold the device until a %BF reading was displayed.Correlations between SKF and BIA were (r=.72, P<.001) with a 3.81% prediction error between methods. Bland-Altman plots yielded wide Limits of Agreement with a significant trend of r= -.34 (P<.05) for Grade 8. Classifying students into FITNESSGRAM’s Fitness Zones, a modified kappa coefficient of .48 (95% CI: .35, .66; P<.001) and proportion of agreement of 0.83 was found between methods. The results suggest although BIA and SKF classified youth into Fitness Zones similarly, there were large differences in %BF estimation between methods with BIA tending to underestimate %BF compared to SKF in older children with higher levels of adiposity.
Keywords: Adolescent, Body Composition, FITNESSGRAM, Measurement, Validity
Cite this paper: Ryan Burns, James Hannon, Brett Allen, Timothy Brusseau, Convergent Validity of Skinfold Thickness and the Hand-held Bioelectrical Impedance Analyzer using Current FITNESSGRAM Standards, International Journal of Sports Science, Vol. 3 No. 6, 2013, pp. 193-197. doi: 10.5923/j.sports.20130306.02.
Article Outline
1. Introduction
- Over the past couple of decades, obesity rates have been a major public health concern in the US with obesity prevalence among children and adolescents almost tripling since 1980[1]. The prevalence of cardiovascular disease and type II diabetes risk factors associated with excess adiposity has shown to track reasonably well from childhood and adolescence into adulthood where it affects morbidity and mortality[2]. Because of the importance to the future health of adolescent youth, proper screening measures are needed that can be used in physical education settings to identify those who may be at risk for chronic disease later in life if unfavorable body composition were to track from current levels.The FITNESSGRAM fitness and physical activity assessment and reporting program incorporate body composition as one of its domains of health related physical fitness[3]. FITNESSGRAM recommends the use of a direct measure of adiposity such as percent body fat estimated from two-site skinfold thickness assessment (SKF) or an alternative measure, percent body fat estimated from bioelectrical impedance analysis (BIA) to classify children into one of three Fitness Zones that are related to health risk.SKF is a more direct measure of adiposity compared to BMI[4] and requires the use of calipers to measure skinfold thickness at various sites on the child’s body. Two-site SKF assessment (triceps and calf) has demonstrated acceptable test-retest reliability (ICC>.98)[5] and has estimated %BF within ±2% compared to a four-compartment criterion in a sample of African American and Caucasian adolescents[6]. A viable alternative to the use of SKF in physical education classes is BIA. Body fat is estimated from BIA by sending a low-level electrical current through the body using a portable “foot-to-foot” or “hand-to-hand” device that can be easily administered in physical education settings. The segmental hand-held Omron BIA (Model HBF-306) device is popular in physical education settings because of its ease of use, portability, and affordability (cost<$75.00). The test-retest reliability of this device is strong (ICC>.98)[7, 8, 9] but Lukaski and Siders[10] showed that when Omron BIA was compared to DEXA, there was a 2.3% (men) to 6.3% (women) underestimation of %BF, especially in individuals with higher levels of adiposity. However, other studies have shown acceptable agreement between the Omron BIA and DEXA giving evidence for its criterion-related validity [5, 11]. Estimations in %BF between two-site SKF and Omron BIA have shown evidence of disagreement in the adolescent population. Using a sample of 8th grade youth and the old FITNESSGRAM standards for analysis,[5] reported that Omron BIA underestimated SKF in high adipose girls yet found acceptable agreement into FITNESSGRAM’s Fitness Zones with percentage agreement of 92.6% for boys and 87.2% for girls. Hannon et al.[12] also found Omron BIA under-estimated of body fat compared to SKF in adolescent boys and girls, and using static cutoffs for obese/non-obese classification, found that the two methods agreed 84% of the time.Since two-site SKF and BIA are the recommended methods to assess body composition for the FITNESSGRAM program, their relationship and agreement must be examined to establish convergent validity. Although SKF and Omron BIA may relate to criterion measures of body composition, their estimation of body composition may not necessarily relate to each other in physical education settings. Evidence for convergent validity and strong relative accuracy will suggest that these two field tests would yield similar reporting outcomes when administered to physical education students. Conversely, poor evidence for convergent validity and weak relative accuracy would indicate that these two field tests may have differences in body composition reporting outcomes, meaning that a student may receive a different reporting outcome (health classification) based on which field test was administered. The purpose of this study was to examine the convergent validity and relative accuracy between SKF and Omron BIA using the new FITNESSGRAM body composition standards. It was hypothesized that these two field methods would have high disagreement in body fat estimates; therefore concurrent use in physical education curricula should be revisited.
2. Methods
2.1. Participants
- Participants included 134 school-aged youth (65 boys, 69 girls) recruited from the 6th, 7th, and 8th grades (mean age=12.9 years, SD=.87 years) from three schools located in a metropolitan area in the Southwestern United States. The sample distribution by grade included 34 6th graders (17 boys, 17 girls), 52 7th graders (22 boys, 30 girls), and 48 8th graders (26 boys, 22 girls). Written consent was obtained from parents and assent was obtained from the participants prior to data collection. The University ethics committee, the Institutional Review Board, and principals from the participating schools approved the protocols used in this study.
2.2. Procedures
- Data collection took place on one testing day during each student’s physical education class. All measurements were conducted at least 2 hours post-prandial during the final two class periods of the school day to ensure consistency for time of day testing. A trained graduate student within the Department of Exercise and Sport Science administered all testing to ensure consistency during data collection. At the beginning of their physical education class, students were asked to remove their shoes, as height (to the nearest 1 cm) and weight (to the nearest 0.1 kg) were determined using a portable stadiometer (Seca 213; Chino, CA, USA) and medical scale (Tanita HD-314; Arlington Heights, IL, USA). Students then entered a private screening area where skinfold measurements were taken on the students’ triceps and medial calf using a Lange (Ann Arbor, MI, USA) skinfold caliper. Each site was measured 3 times in a rotating order on the students’ right side with the average used as the recorded measure. Percent body fat was estimated using the gender-specific equations from[13]. Finally, the students’ height, weight, age, and gender were entered into a handheld OMRON body fat analyser (Model HBF-306; Lake Forest, IL, USA) by the researcher. The students held the analyser with arms extended, parallel to the floor until the device displayed the student’s body fat percentage estimated from manufacturer-developed equations.
2.3. Statistical Analyses
- Data were screened for outliers and normality was checked prior to the main analyses. Convergent validity was analyzed using Pearson correlations, Bland-Altman plots, and prediction error using SKF as reference, along with modified kappa statistics and proportion of agreement. Bland-Altman[14] pair-wise comparisons were used to assess agreement between SKF and BIA within each gender group and grade level. Differences between the methods (BIA-SKF) were plotted on the y-axis and the method means (BIA+SKF/2) were plotted on the x-axis. The mean differences (MD), 95% Limits of Agreement (MD±1.96*SD), and correlation coefficients (r) between method differences and means were reported.Classification agreement into body composition Fitness Zones between BIA and SKF was assessed using FITNESSGRAM’s current age and gender specific criterion-referenced standards. Each student was classified into either the Healthy Fitness Zone (HFZ), Needs Improvement Zone-some risk (NIZ-some risk), or Needs improvement Zone-health risk (NIZ-health risk) based on SKF and BIA assessment. A 3x3 contingency was created displaying the agreement between methods into the Fitness Zones. Agreement was statistically analyzed using modified kappa statistics and proportion of agreement. Kappa was considered weak if <.20, fair if .20-.40, moderate if .40-.60, substantial if .60-.80, and almost perfect if .80-1.00[15]. All analyses were carried out using STATA v12.0 (College Station, TX, USA) statistical software.
3. Results
3.1. Pearson Correlations and Prediction Error
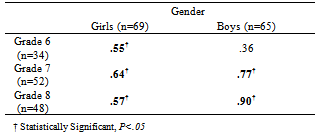
- Table 1 shows the Pearson correlations between SKF and Omron BIA per grade-gender group. The correlation for the entire sample was (r=.72, P<.001). Prediction error, calculated by standard error of measurement, was found to be 3.81% for the entire sample.
|
3.2. Bland -Altman Analyses
- The results suggest that for boys and girls, %BF agreement between methods was similar. Bland-Altman analyses revealed that for the boys the MD between SKF and BIA was (MD=-.92%) with 95% Limits of Agreement of (-11.00%, 9.17%). For the girls, the MD was (MD=-1.26%) with 95% Limits of Agreement of (-11.31%, 8.77%). There were no significant trends found between methods when analyzing the %BF agreement by gender group. Bland-Altman difference plots for each grade level are displayed in Figures 1-3. In general, MDs increased with older grade levels, however Limits of Agreement tended to be more narrow at older grade levels. There was a significant trend between method differences and means for Grade 8 (r=-.34, P<group.
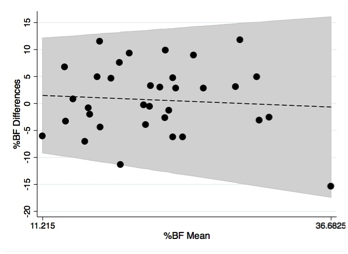 | Figure 1. Body fat agreement between SKF and BIA for Grade 6. MD=0.66%; 95% Limits of Agreement (-11.93%, 13.26%) |
3.3. Fitness Zone Classification Agreement
- Table 2 presents a 3x3 contingency table showing the agreement between SKF and BIA in their classification into FITNESSGRAM’s Fitness Zones. New FITNESSGRAM standards use a three Fitness Zone classification system that are age and gender specific. Agreement into Fitness Zones between SKF and BIA was moderate with kappa=0.48 (95% CI: .35, .66; P<.001) and proportion of agreement=0.83.
|

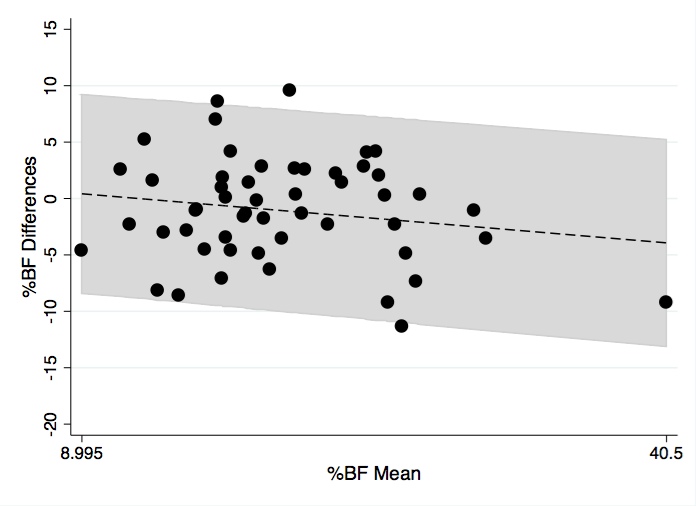 | Figure 2. Body fat agreement between SKF and BIA for Grade 7. MD=-1.07%; 95% Limits of Agreement (-10.03%, 7.89%) |
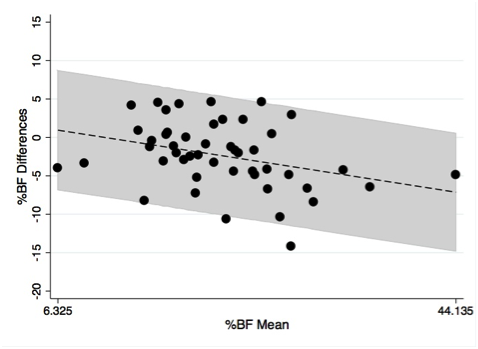 | Figure 3. Body fat agreement between SKF and BIA for Grade 8. MD=-2.36%; 95% Limits of Agreement (-10.86%, 6.08%) |
4. Discussion
- The purpose of this study was to examine the convergent validity of SKF and Omron BIA in a sample of middle-school students. The correlations and prediction error between methods was similar to that of[5], where a correlation between SKF and Omron BIA of r=.74 and prediction error of 4.1% was fund using a similar sample size of 132 8th grade youth. The sample in this study was younger involving 6th, 7th, and 8th grade students. Nonetheless, the correlations and error were nearly identical to[5] with a correlation of r=.72 and prediction error of 3.81%. Despite these aforementioned similarities, the classification agreement into Fitness Zones differed compared to[5]. The current body composition Fitness Zone cut-off scores were developed from two-site skinfold assessment using the triceps and sub-scapular sites[17], even though the triceps and calf site are recommended for assessment by FITNESSGRAM[3]. Students are classified based on their age and gender into 3 Fitness Zones: HFZ, NIZ-some risk, and the NIZ-higher risk. In this study, 83% of the time the SKF and BIA agreed into classifying the students into the HFZ or the NIZ. Ihmels et al.[5] found higher percentage of agreement between the Omron BIA and SKF (92.6% for boys and 87.2% for girls). However[5] used an older sample of adolescent youth and used the older dichotomous FITNESSGRAM classification scheme for analysis. The classification agreement yielded in the current study was nearly identical to[12]. Hannon et al.[12] found a percentage of agreement of 84% in classifying youth into obese or non-obese categories using static cut-off values.Bland-Altman analyses were also used to examine individual differences in %BF estimation between SKF and BIA across the range of body composition values. There were similar 95% Limits of Agreement between SKF and BIA within each gender group. Suggesting that the two methods agreed similarly in ability to estimate %BF regardless of the child’s gender. Prior research has examined agreement between SKF and BIA controlling for gender in adolescent school-aged children, however no research has examined agreement controlling for grade level. There were wide 95% Limits of Agreement across all grade levels with the overall trend being that the younger grades having larger variability than the older grades. Both methods of body composition assessment can be efficiently used in physical education classes to assess adiposity, however it is discerning that there were such large differences in %BF estimation with some students displaying differences as much as 13%. Although the SKF method is the recommended body composition assessment for FITNESSGRAM, the Omron hand-held BIA provides a less time consuming and intrusive method for acquiring adiposity measurements. However, a possible limitation of this method is that it is highly sensitive to the hydration status of the individual; with low levels of hydration associating with higher %BF readings[18]. Hydration status was not controlled for in this study and the practicality of controlling for hydration in a physical education setting is not feasible when administering to large class sizes. Despite the lack of control for hydration, the BIA method tended to underestimate SKF especially in children with higher levels of adiposity (see Figure 3). In agreement with studies conducted by[10] and[12], there was evidence for the Omron hand-held BIA underestimation of %BF compared to SKF in adolescent school aged children. This study supports previous findings, especially in older children where there was a statistically significant correlation between %BF method differences and means for Grade 8. However for younger children in Grade 6 and Grade 7, no statistically significant trends were found. Perhaps the bias toward underestimation of %BF using BIA is a phenomenon more prevalent in older children. Future research needs to further explore bias trends in younger and older children to provide further evidence for this phenomenon. Because there was a lack of a criterion measure of body composition used in this study, there is no way of knowing what method was a more valid measure of body composition. Previous research has examined the validity of both SKF and Omron BIA but the conclusions have been inconsistent[8, 9, 10, 19]. Eisenmann et al.[20] found that two-site SKF correlated well with DEXA (r=.82) but the correlation between Omron BIA and DEXA was low (r=.30). Jensky-Squires et al.[21] found a correlation of (r=.83) between Omron BIA and DEXA but wide 95% Limits of Agreement (-11%, 4.5%) with a mean underestimation of -3.3%. The evidence suggests that BIA has a tendency to underestimate %BF compared to criterion measures and compared to SKF in children and adults. Although the criterion-related validity of SKF using Slaughter equations is questionable, its higher correlations with DEXA and more accurate agreement with criterion measures suggest that it is probably the more valid measure body composition between the field methods.There are limitations to this study that may have affected the results. The sample used was heavily Caucasian (85% Non-Hispanic Caucasian) and approximately 70% of the sample was classified into FITNESSGRAM’s HFZ using SKF and BIA. Future research needs to examine agreement using a more ethnically diverse sample and a sample with a larger range of body composition to make the classification into the Fitness Zones more symmetrical. Additionally, the sample was limited to middle-school students so the results cannot be generalized to younger or older age groups.
5. Conclusions
- The results of this study introduce some issues that must be considered when physical educators or clinicians are choosing a method to assess body composition. Although SKF and BIA are more direct measures of adiposity than BMI, their agreement in estimating a child’s %BF is questionable. If a physical educator or clinician is choosing between methods, they must consider that the BIA will tend to have lower %BF estimations compared to SKF, especially among children who have higher levels of adiposity. It is unknown what method is a more valid measure of body composition, although SKF has been validated against 4-compartment models and DEXA while the Omron hand-held BIA has demonstrated validity in a few studies, but showed significant underestimation of %BF when compared to DEXA in others. Despite the discrepancies in %BF agreement, the body composition classification agreement into FITNESSGRAM’s Fitness Zones was moderate. In the current study, approximately 83% of the time the SKF and BIA agreed in classifying students into the HFZ, NIZ-some risk, or NIZ-health risk Fitness Zones. Therefore, if physical educators or clinicians wish to use body composition assessment for the sole purpose of classification, both SKF and BIA are similar in ability and arguably could be used interchangeably. However, if physical educators and clinicians wish to be more precise and inform their students or patients of their exact %BF, the potential for a high degree of disagreement between the two methods must be taken into consideration before administration to a specific population. It is concluded that the convergent validity between SKF and Omron BIA is questionable.
ACKNOWLEDGEMENTS
- The authors would like to give a special thanks to the administrators, teachers, and students of Early Light Academy, J.E. Cosgriff Memorial Catholic School, and The Madeleine Choir School for participating in this study.