-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2013; 3(5): 172-182
doi:10.5923/j.sports.20130305.05
The Relationship between Self-Reported and on Field Lower Extremity Functional Assessment Tools Used for Assessing Functional Status in Hip Dysfunction Athletes
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML1Post graduated from Amity University, Dept. Amity Institute of Physiotherapy, sec. 125 , Noida, 201303, India
2Professor at Amity University, Dept. Amity Institute of Physiotherapy, sec.125, Noida, 201303, India
Correspondence to: Zeinia Samar, Post graduated from Amity University, Dept. Amity Institute of Physiotherapy, sec. 125 , Noida, 201303, India.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Background: Hip injuries are fairly common in athletes. Hip pain in runners and soccer players is a common problem treated by orthopedic and sports physical therapist. Effectiveness of the current functional tools available in hip dysfunction athletes is requires further study.[1]Objective: To find out the relationship between self reported and on field lower extremity functional assessment tools used for assessing functional status in hip dysfunction athletes and to determine which is better. Methods: This study was conducted on 50 athletes with hip dysfunction. The test procedures consisted of a general warm-up, a task specific warm-up, actual testing, and a cool down. Participants performed FMS, triple hop distance (THD), and timed 6m hop test, finally LEFS scores were taken. The scores for THD and 6m THT were expressed as limb symmetry index scores (LSI). Co-relation between all of them was determined. Results: FMS and LEFS were found to be significantly co-related, 6m THT and THD were found to be significantly correlated, while FMS and hop tests, LEFS and hop tests were not correlated with each other. Conclusion: We concluded that there is a relationship between self-reported functional assessment tool LEFS and on field functional assessment tool FMS used for assessing L.E. functional status. FMS and LEFS do not prove to be useful while 6m THT and THD prove to be useful tools for assessing functional status in hip dysfunction athletes.
Keywords: LEFS, Functional Movement Screen (FMS), Hop Tests, 6m Timed Hop Test, Triple Hop Distance (THD), Hip Dysfunction
Cite this paper: Zeinia Samar, Anu Bansal, The Relationship between Self-Reported and on Field Lower Extremity Functional Assessment Tools Used for Assessing Functional Status in Hip Dysfunction Athletes, International Journal of Sports Science, Vol. 3 No. 5, 2013, pp. 172-182. doi: 10.5923/j.sports.20130305.05.
Article Outline
1. Introduction
1.1. Prevalence of Hip Injuries
- Hip injuries are fairly common, accounting for roughly 5% to 6% of musculoskeletal complaints in adults and 10% to 24% of complaints in children.[2] These injuries are particularly common in certain athletes, such as dancers, runners, and soccer players, because their sports activities involve a high degree of increased force and extremes of movement across the hip.[2] Hip pain in runners is a common problem treated by orthopaedic and sports physical therapists[4]
1.2. Common Hip Injuries in Athletes
- Dysfunction can be defined as pain, asymmetry, or injury that impairs normal movement and performance of a functional activity[1]. The common hip injuries in athletes are muscle strains, hip contusions, avulsion and apophyseal injuries, hip dislocations and subluxations, labral tears and hip fractures. Many of these injuries occur early in the athletic season.[6] Muscle strains are most common. The adductor muscles are frequently involved in strains, especially in hockey, football, and soccer players.[2] Strains of the rectus femoris muscle are common, result from an explosive hip flexion maneuver, such as sprinting or kicking, or from eccentric overload as the hip is extended, athletes have painful and possibly weak knee extension or hip flexion. Strain or rupture of the iliopsoas muscle can also occur during resisted hip flexion or passive hyperextension (eccentric overload). Soccer players often suffer from this type of injury when they are hit as they extend their leg to kick.[6]
1.3. Functional Performance Testing
- Functional performance tests require the integration of multiple body regions and systems to execute movement patterns and therefore may have an advantage over more traditional clinical measures.[1] Components of ROM, flexibility, muscular strength, endurance, coordination, proprioception,[9] balance, and motor control of multiple regions can be assessed simultaneously by observing the movement patterns in which the athlete normally functions.[1,9] Functional performance tests have been commonly used to identify impairments related to ankle or knee injuries and determine the readiness of an athlete to return to sports after injury.[1]The Lower Extremity Functional Scale (LEFS) is a region-specific, self-report functional status measure.[14] Individuals’ scores on this 20-item questionnaire range from 0 to 80, with higher scores indicating better functional status.[14] Each LEFS item is scored on a Likert scale from 0 to 4 with higher scores representing higher functional levels, the maximum score being 80.[40] Functional movement screen:Gray Cook designed the FMS to determine if an individual possesses or lacks the ability to perform fundamental movement patterns[11] and in an effort to bridge the gap between the pre-participation medical screening and performance testing.[10,11] and to determine potential injury risk.[1] Inter-rater reliability (ICC3,1) for the composite FMS score was .971.[9] The FMS has been used in sports teams to screen pre-season for injury risk and to develop specific intervention programs to prevent injuries. [9]Triple-hop distance(THD) was designed originally as a test for those recovering from injury or surgery to gauge readiness for activity and frequently has been reported to require a combination of muscular strength, power, and balance.[13] THD is a strong predictor of lower limb muscular strength and power in a healthy soccer population and support its clinical usefulness as a preseason screening test.[7] The test-retest reliability of this standardized protocol is excellent with intraclass correlation coefficient (ICC) as 0.97[13]. The timed 6m hop is a power test, which assesses the time taken to cover a distance of 6m by hopping.[14] The ICC range from .88 to .97 when analyzing mean scores between the sessions[14]. For patients with unilateral hip symptoms, hop tests may be used in comparison of the uninvolved side.[1]Correlation was determined between LEFS with FMS, 6m timed hop test and THD. In order to utilize a functional tool to see the progress of a rehabilitation protocol or patient progress, it is important to know the relationship between these functional performance tests. Further study is needed to find out the relevancy of existing functional performance tests to be used in a young, athletic population with hip dysfunction.[1]
2. Methods
- Fifty collegiate athletes of soccer and runner teams (both male and female) from the different universities were recruited and volunteered for the study. The subjects were required to read and sign consent forms approved by Amity Institute of Physiotherapy. Each subject completed a short questionnaire/assessment regarding their injuries history, usual physical activity levels, and demographic information. Athletes that did not clear the pre-participation physical exam were excluded from the study. The assessment form is provided in the appendix.Inclusion criteria : • Subjects with the history of greater than 4 months[1] and less than 8 months of hip pain.• 18-26 years old who had not sustained an injury within the previous 30 days that prohibited full participation in preseason practice and/or conditioning programs[11], • Patients with BMI 20-29 Kg/m sq.[14], • Those players who were on the active roster at the start of the competitive season[12], and• Membership on the injured reserve and time loss of 3 weeks was utilized as the injury definition.[12]Exclusion criteria: • An injury sustained within the 30 days preceding testing that excluded the athlete from participating in practice and/or competition[11],• Recent surgical intervention that limited the athlete's participation in sport due to physician-imposed restriction [11] and • Athletes who have any other recent unresolved dysfunction of shoulder, spinal, elbow, wrist, knee, SI joint, or ankle
2.1. Instrumentation
- The required equipment includes a 2x6 Board, 4 foot dowel rod, 2 smaller dowel, an elastic band, measuring tape. The picture of the equipment is provided in Figure 1.
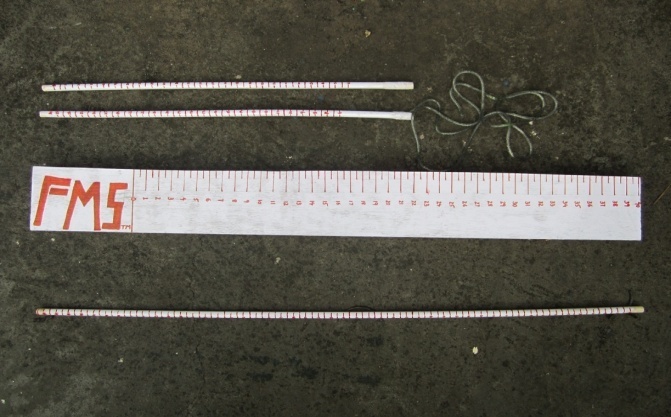 | Figure 1. FMS equipment |
2.2. Procedures
2.2.1. Overview
- The subjects involved in the study (n= 50) comprised of hip dysfunction athletes. The test procedures consisted of a general warm-up, a task specific warm-up, actual testing, a cool down.[29] The general warm-up required participants to ride a stationary bike at a steady, comfortable speed for 3min followed by gentle quadriceps, hamstrings, and calf stretches.[29] Stretching involved 3 repetitions of each stretch using a 10-second hold.[29] The task specific warm-up allowed subjects the opportunity to practice each functional performance test.[29] First, the test administrator demonstrated each functional performance test.[29] Participants then practiced each test 3 times in the following order: FMS, triple hop distance (THD), and timed 6m hop test. Practice was done in this order so as to get the athlete acquainted with what they have to do in the final testing and hence, minimizing errors while final testing. Participants rested approximately 30 sec between each practice trial and rested 1 minute prior to actual testing.[29] Actual testing had participants perform each functional performance test in a randomly determined order.[29] The scores for THD and timed 6m hop test were expressed as lower symmetry index scores (LSI). The limb symmetry index (LSI) has been the most frequently reported criterion for assessing whether muscle strength and hop performance are normal or abnormal, i.e. that the capacity of the injured leg is, or is not, as good as that of the non-injured leg. An LSI of <90%, i.e. more than 10% difference between limbs has been regarded as unsatisfactory for both strength and hop performance. [30,31] Hop limb symmetry index (LSI) for THD was expressed as the percentage of the longest involved limb hop distance divided by the longest uninvolved limb hop distance.[27] In 6-m timed hop, LSI was expressed as the percentage of the fastest uninvolved limb time divided by the fastest involved limb time.[27] Testing consisted of 3 consecutive trials for each functional performance test.[29] Participants received no verbal encouragement during actual testing.[29] A cool down period followed actual testing.[29] Subjects were verbally instructed to perform the gentle stretching as previously done during the general warm-up period.[29] Then, LEFS scores were taken, that is a subjective tool.
2.2.2. Functional Movement Screen (FMS)
- The FMS™ consists of seven movement tests, described by Cook et al[10,17,18] that include: Deep Squat, Hurdle Step, In-Line Lunge, Shoulder Mobility, Active Straight Leg Raise, Trunk Stability Push-Up, and Rotary Stability.[11]Scoring the Functional Movement Screen™The scoring for the FMS™ consists of four possibilities. The scores range from 0 to 3, three being the best possible score. An individual is given a score of zero if at any time during the testing he/she has pain anywhere in the body. If pain occurs, a score of zero is given and the painful area is noted. A score of one is given if the person is unable to complete the movement pattern or is unable to assume the position to perform the movement. A score of two is given if the person is able to complete the movement but must compensate in some way to perform the fundamental movement. A score of three is given if the person performs the movement correctly without any compensation. Specific comments should be noted defining why a score of three was not obtained.[10]Grades from 3 - 0– 3 perform functional movement pattern– 2 perform functional movement pattern with compensation– 1 inability t