-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2013; 3(5): 163-171
doi:10.5923/j.sports.20130305.04
The Effects of Ankle Taping on Ankle Strength in Varsity Basketball Players
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLPaolo Sanzo, Courtney Steven, Carlos Zerpa
School of Kinesiology, Lakehead University, Thunder Bay, P7B 5E1, Canada
Correspondence to: Paolo Sanzo, School of Kinesiology, Lakehead University, Thunder Bay, P7B 5E1, Canada.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Ankle sprains are one of the most common injuries among basketball players that can lead to residual effects negatively affecting performance. To prevent ankle injuries, athletes commonly have their ankle taped to externally stabilize the ligaments without disturbing normal joint biomechanics. There has been contradictory reports and significant debate, however, about the effectiveness of ankle tape and its impact on sport or motor performance. The purpose of this study was to analyze the effect of a closed basket weave ankle taping technique on ankle strength in varsity basketball players before and after a sport specific activity. Fifteen varsity basketball players (8 females and 7 males) participated in this study. Ankle strength was measured before and after activity under two conditions (without and with taping). During the first session neither ankle was taped and strength was tested bilaterally before activity and after 30 minutes of basketball shooting drills. During the second session the dominant ankle was taped, the non-dominant ankle was not taped, and the same testing format used. A repeated measures ANOVA was completed to analyze the data. The application of ankle taping did not have a significant effect on ankle strength. Although not statistically significant, there was an increase in strength following activity for dorsiflexion, inversion and eversion with the application of tape to the dominant ankle and a reduction in plantarflexion strength. The decrease in strength for plantarflexion with tape to the dominant ankle was less than when tape was not applied. The results of this study have demonstrated that tape does not significantly affect ankle strength and may actually reduce fatigue and possibly improve performance. Therefore, if the patient or athlete reports subjective improvement and believes in the utility of the tape then it should be considered as a possible adjunct for treatment without concern for negative effects on ankle strength.
Keywords: Ankle Tape, Ankle Strength, Taping
Cite this paper: Paolo Sanzo, Courtney Steven, Carlos Zerpa, The Effects of Ankle Taping on Ankle Strength in Varsity Basketball Players, International Journal of Sports Science, Vol. 3 No. 5, 2013, pp. 163-171. doi: 10.5923/j.sports.20130305.04.
Article Outline
1. Introduction
- Ankle sprains are one of the most common sport-related injuries[1, 2]. They are most common in sports such as basketball that require frequent changes in direction and rapid acceleration and deceleration[3, 4]. About 85% of all ankle injuries are ligamentous sprains[3, 5]. Of these ligamentous sprains, a high proportion involves the lateral ligamentous and myofascial structures of the ankle[5]. Lateral ligament sprains account for approximately 15% of all athletic injuries[6]. Lateral ankle sprains, also known as inversion ankle sprains, often occur with the foot in a plantarflexed and inverted position or occur when landing inappropriately[2]. This may be due to the fact that the peroneal muscles are not strong enough to prevent the forced inversion causing the lateral ligaments, the anterior talofibular and calcaneofibular ligaments, to be injured[1, 3, 4, 6]. Ankle sprains may result in residual effects such as pain, inflammation, weakness, and a loss of motion[1]. These residual effects may negatively affect performance, leading to a loss of practice and game time, and the presence of chronic ankle instability, weakness, and pain[4, 7]. To prevent these types of injuries athletes often have their ankles taped prophylactically[2, 5]. The clinical reasoning behind taping is to externally stabilize the ligaments of the ankle without disturbing the normal joint mechanics[6]. There has been, however, significant debate and contradictory reports about the effectiveness of ankle taping and bracing. It has been reported that initially ankle tape is effective at restricting joint range of motion (ROM) when first applied but it loses up to 40% of its restrictiveness after only 10 minutes of exercise, and has no significant restrictiveness after approximately 60 minutes of activity[6]. Greene and Hillman[6] compared the support provided by a semi-ridged orthosis and adhesive ankle tape before, during and after a three hour volleyball practice by studying the effect the devices had on inversion and eversion ROM and on the participant’s vertical jumping ability. Greene and Hillman found that before exercise both systems significantly restricted ankle inversion and eversion ROM by approximately 40% (p<.01) but there was no significant difference between the bracing and taping. Throughout exercise testing it was reported that the orthosis significantly restricted ankle ROM more than taping. The orthoses demonstrated only minimal loosening while the tape loosened and lost its ability to stabilize the ankle after 20 minutes of activity[6]. During the vertical jumping test, Greene and Hillman also found that neither method had a significant effect on the athlete’s vertical jump height. It was concluded that initially tape was effective at restricting joint ROM but quickly lost its effectiveness and was ineffective after 60 minutes of activity. As well, tape did not appear to affect vertical jumping ability. There is also debate and conflicting reports about the effects of ankle taping on motor performance. Some studies have reported that motor performance may be adversely affected with the use of ankle taping while others have reported no significant impairment[6, 8, 9].Burks et al.[8] analyzed the effects of prophylactic taping and bracing on athletic performance. Subjects included 30 varsity athletes in peak condition that were tested with ankle taping and with the application of two different types of ankle braces (Swede-O and Kallassy braces). Participants completed four different tasks including the broad jump, vertical jump, 10 yard shuttle run and 40 yard sprint[8]. Each task was performed twice under the following conditions: with no support; with both ankles taped; with both ankles in the Swede-O braces; and with both ankles in the Kallassy braces[8]. All performance scores decreased with taping and bracing but not all decreases were significant[8]. There was a significant decrease in vertical jump height by 4% (p<.05); a significant increase in the shuttle run time by 1.6% (p<.05); and a significant increase in the sprint time by 3.5% with tape applied[8]. When the Swede-O brace was applied to the ankle, decreases in the vertical jump height (4.6%), broad jump (3.6%), and sprint (3.2%) abilities were evident (p<.05). When the Kallassy brace was applied to the ankle, decreases in the vertical jump height (3.4%) were evident (p<.05)[8]. There was a significant difference (p<.05) between the shuttle run time with taping applied to the ankle compared to the time to complete the test with the use of the Kallassy ankle brace. The results of the broad jump with the Swede-O ankle brace were also significantly shorter than with the Kallassy ankle brace[8]. Burks et al. concluded that when the ankles were immobilized with either taping or bracing there was indeed a decrease in performance as compared to the completion of these same tasks without taping or bracing[8]. A study by Verbrugge[9] also examined the effect of a semi-rigid Air-Stirrup brace and adhesive ankle taping on motor performance. Twenty six male athletes were asked to complete an agility run, a 40 yard sprint, and a vertical jump test with ankle bracing and taping. Verbrugge[9] reported that ankle taping and bracing had no significant effect on agility, sprint speed, or vertical jumping ability contradicting previous negative reports. The type of taping technique and whether an underlay of prewrap should be used has also been questioned. A study by Ricard et al.[2] compared the effects of tape with and without prewrap on dynamic ankle inversion before and after activity. Range of motion data was measured using an electric goniometer while participants balanced on a platform in 15° of plantarflexion. Sudden ankle inversion was induced by dropping the platform to 37° of inversion. Total inversion, time to maximum inversion, average inversion velocity, and maximum inversion velocity was measured for 10 trials[2]. Ricard et al. reported no significant difference between the effectiveness of applying tape directly to the skin or over prewrap. There was, however, a significant difference (p<.05) between both taping conditions and no tape for average inversion velocity, maximum inversion, maximum inversion velocity, and the time to maximum inversion[2]. Therefore, both taping conditions provided some restriction and support after exercise.Despite the clinical hypothesis that the use of an external support reduces the ability to perform functional and sport specific movements, outcomes are often inconclusive and variable[10]. In a meta-analysis conducted by Cordova et al.[10] the effect of adhesive tape, a lace up style and semi rigid style brace were examined on sprint, agility and vertical jumping abilities. A negative effect with the use of lace up brace on sprint speed was reported but otherwise the results were inconclusive. Another valid consideration regarding the use of ankle taping as part of the rehabilitation process or prophylactically is that there is a significant cost and many hours of work associated with this approach[5]. It has been reported that ankle taping may result in a cost of $1.75 per ankle resulting in more than $400 per athlete in expenditures over the course of a season[4]. The use of long term taping may further add financial impact and healthcare costs, raising the question of whether this added expenditure is worth the benefit. If tape is ineffective or hinders performance then this cost may not be worth the expense and be better put towards other areas of treatment or prevention. Studies that that have examined the effectiveness of ankle taping from an injury prevention perspective have produced mixed results. Prophylactic taping and bracing has been considered one possible way of preventing ankle injuries at all levels of sport. Mickel et al.[4] examined the incidence of injury during a high school football season comparing ankle taping to bracing. Eighty three athletes were randomly assigned to either prophylactic bracing or taping to both ankles and the incidence of injury monitored. There was no statistically significant difference in the incidence of ankle sprains between the groups. The time taken to apply the tape to the athletes, and the average cost to tape each ankle during the entire season was greater than the cost of the available brace. The projected savings of using prophylactic bracing rather than prophylactic taping of the ankle again substantiated the question of the cost effectiveness and benefit of using this taping.In a systematic review by Dizon and Reyes[11] comparing the effectiveness of a variety of external ankle supports (ankle tape, brace or orthoses), ankle braces reduced ankle sprains by 69% and ankle tape by 71%.Miller et al.[12] investigated the effectiveness of tape, bracing and no intervention on ankle laxity before and after exercise in subjects with varying degrees of previous ankle injury. Taping provided the best results for inversion and eversion movement restriction. Following the removal of the external supports, however, post exercise laxity was the greatest after removing the brace and it was concluded that taping may be a better option to consider clinically[12].Conversely, Rosenbaum et al.[13] examined the effect of ten different braces (rigid, semi rigid and soft) and found no difference on agility, vertical jumping, cutting, hopping, sprinting and side stepping tasks. Also, in a systematic review and meta-analysis by Raymond et al.[14] examining the effect of taping or bracing on proprioception, no significant effect was reported.The medical literature available on the use of ankle taping and its direct effect on ankle strength, however, is limited. As a result, the purpose of this study was to determine if there was a difference in the resisted isometric ankle strength of the ankles of varsity basketball players before and after a sport specific exercise activity with and without ankle taping.It was hypothesized that ankle strength and force production would be decreased when resisted isometric strength was tested before practice with tape applied to the ankle as compared to without tape. It was also hypothesized that force production would be the same when resisted isometric strength was tested after practice with and without tape applied to the ankle.
2. Methods
2.1. Subjects
- Fifteen participants (eight females and seven males) were recruited from a university men’s and women’s varsity basketball team. Participants were included into the study if they: 1) were over the age of 18 at the time of testing and; 2) were members of the university varsity basketball team. Participants were excluded from the study if they: 1) had an acute ankle injury within the past six weeks prior to testing; 2) were unable to participate in practice without their ankle(s) taped or braced and; 3) were allergic to adhesives such as Band Aids, tape or Tuff Skin. Prior to participation in the study, all procedures and risks were explained to the subjects and informed consent was obtained.
2.2. Instruments and Materials
- The materials used in this study included Tuff Skin, heel and lace pads, Prowrap, and zinc oxide tape to perform a closed basket weave taping technique to the ankle. A Baseline Electronic Dynamometer Manual Muscle Tester (Fabrication Enterprises Incorporated, Model 12-0342, FabricationEnterprises.com) was used to measure ankle strength and a Velcro strap was used to stabilize the lower leg.
2.3. Data Collection and Test Procedures
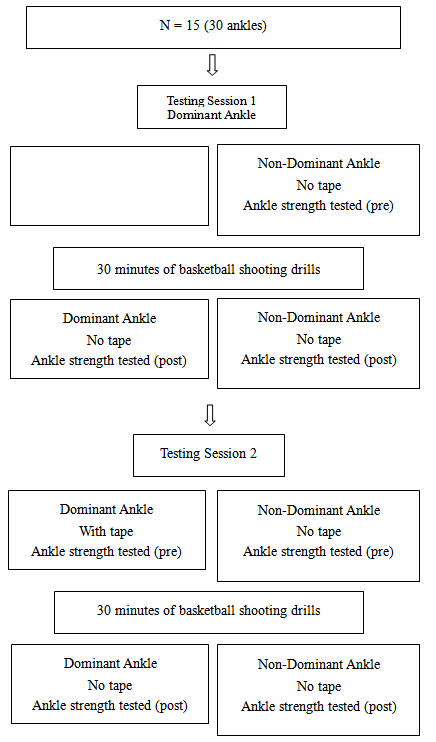 | Figure 1. Study design flow chart |
2.4. Data Analysis
- Descriptive statistics were used to compare mean and standard deviations for ankle strength with and without tape. Repeated measures ANOVA were conducted to examine if there were any significant differences for ankle strength before and after activity with and without ankle tape. A Bonferroni correction was implemented to keep the error rates at an alpha level of .05.
3. Results
- The participants’ mean age, height and weight ranged from 18-23 years (mean age 20.8 years; SD ±1.5), 163.7-198.2 cm (mean height 180.6 cm; SD ±12.2), and 58.3-117.9 kg (mean weight 76.5 kg; SD ±15.8). All participants were right leg dominant. All participants were able to complete the testing and no adverse reactions to the tape or testing protocol were reported.There was no significant difference in ankle strength for plantarflexion (F=.90, p=.36), dorsiflexion (F=2.52, p=.14), inversion (F=4.01, p=.06), and eversion in the dominant ankle over time (F=.56, p=.47) during the first testing session with no tape (see Figure 2). There was no significant difference in ankle strength for plantarflexion (F=3.96, p=.06), dorsiflexion (F=.31, p=.59), inversion (F=.12, p=.74), and eversion in the non-dominant ankle over time (F=.001, p=.98) during the first testing session with no tape (see figure 3).There was no significant difference in ankle strength for plantarflexion (F=1.16, p=.29), dorsiflexion (F=.31, p=.59), inversion (F=.02, p=.90), and eversion in the dominant ankle over time (F=.007, p=.94) during the second testing session with tape (see figure 4).
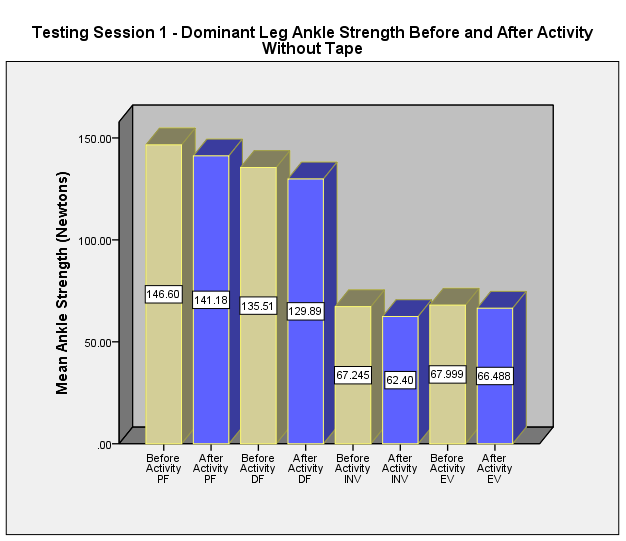 | Figure 2. Dominant leg ankle strength before and after activity without tape (testing session 1) |
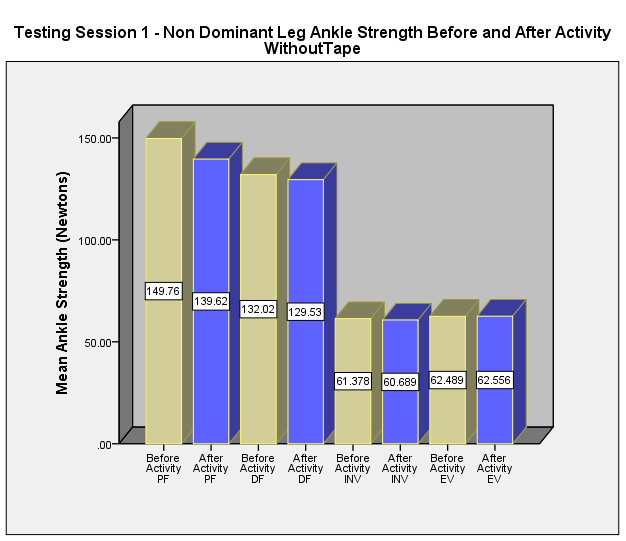 | Figure 3. Non dominant leg ankle strength before and after activity without tape (testing session 1) |
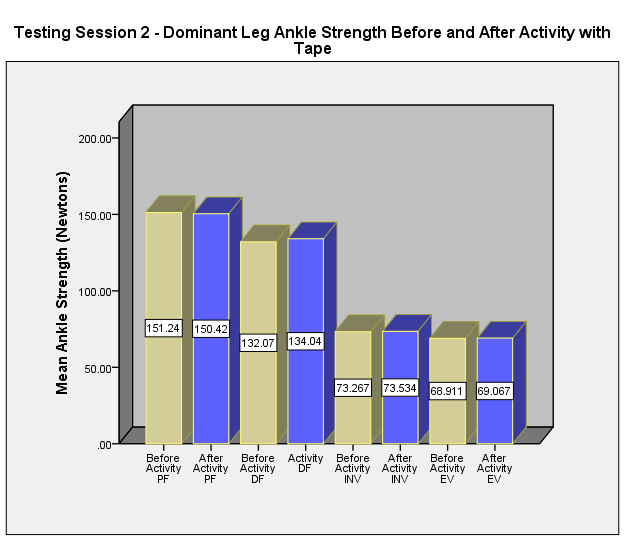 | Figure 4. Dominant leg ankle strength before and after activity with tape (testing session 2) |
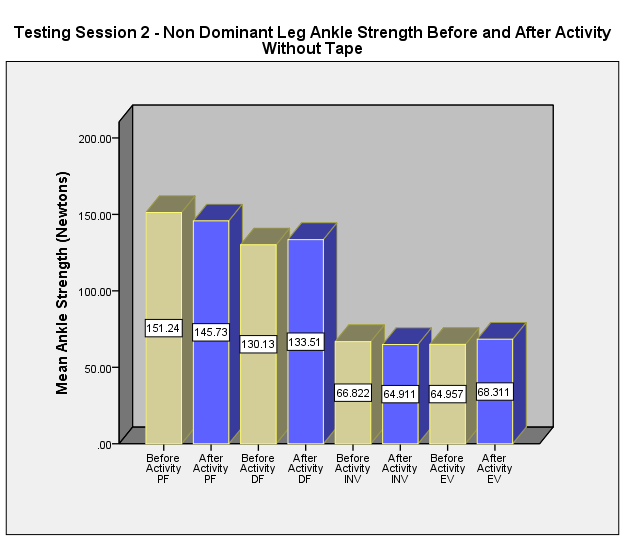 | Figure 5. Non dominant leg ankle strength before and after activity without tape (testing session 2) |
4. Discussion
- Taping is a technique that is used clinically as part of the rehabilitation process when an injury has occurred and prophylactically to prevent injuries in a variety of sport, functional and occupational settings. The exact mechanism by which taping positively or negatively impacts an individual is unclear with inconsistent findings reported. The medical literature available on the use of ankle taping and its direct effect on ankle strength is limited. This study has demonstrated that tape does not significantly affect resisted isometric ankle strength in varsity basketball players. In functional tasks or sports that require strength as a key component or skill, the use of tape may not negatively impact on performance.The results of this study are similar to Greene and Hillman[6] and Verbrugge[9], but contradict the findings of Burks et al.[8]. Greene and Hillman[6] measured the effect of tape on the vertical jumping ability. They reported that tape did not affect the participant’s vertical jumping height.Verbrugge[9] also examined the effect of bracing and ankle taping on motor performance. Verbrugge[9] reported that ankle taping and bracing had no significant effect on agility, sprint speed, or vertical jumping ability. Although these studies tested functional abilities, their conclusions compared to our study are similar in that ankle taping does not appear to have a significant effect on functional abilities or strength.Similar findings were also reported by Ozer et al.[15] who assessed the effects of taping and bracing on functional balance, jumping, multi-joint coordination and proprioception. Twenty physically active male university students were tested under three conditions (with the application of bracing or taping, or when barefoot - control). Participants performed jumping, single leg balancing, coordination and proprioception tests with the Functional Squat System under each condition. No significant difference was found among groups for the balance task. The barefoot group, however, had better results in the vertical jumping task than the other groups. Coordination was better for the bracing and taping groups. Ozer et al.[15] concluded that taping or bracing may have an important role in preventing ankle injuries by affecting the proprioceptive input into the area and the individual’s coordination. The decreased vertical jumping ability may also act in a protective manner if an injury is present and may be beneficial as part of the rehabilitation process in certain situations such as overuse injuries where the goal may be to limit the ability of the patient to jump offloading stress from the area and allowing the injured area to heal. Conversely, if taping and bracing is applied to participants involved in jumping sports the fact that individuals with bracing or taping had decreased vertical jumping ability may be detrimental to their ability if this is a key skill to the sport that they are competing in. This may lead one to suspect that the use of taping and bracing may produce a sport specific effect in some cases and may explain some of the varied findings and contradictory reports on the effects of tape. This may be an area where further research is required to see if similar findings occur across a variety of sports.Another possible mechanism whereby the application of tape may have a protective mechanism is by its effect on ROM. Purcell et al.[16] assessed the effect of two types of tape including self-adherent and white cloth tape compared to no tape on ROM. Range of motion was measured before and immediately after the application of taping, and then after 30 minutes of exercise. Purcel et al.[16] reported that the white cloth and self-adherent tape limited inversion and eversion immediately after the application but after 30 minutes of exercise only the self-adherent tape still decreased ankle ROM. Plantarflexion and dorsiflexion ROM was limited with white tape and self-adherent tape immediately after its application and after exercise. Self-adherent tape was better than white tape, however, as it lost some of its restrictive properties after 30 minutes of exercise[16].Anecdotal reports also suggest that athletes often strongly believe that taping will protect them from injury. As a result, the benefits that we see when tape is applied may be related to a placebo effect. Sawkins et al.[7] compared the effects of placebo to tape in individuals with ankle instability. Thirty subjects with ankle instability were asked to complete a hopping test and modified star excursion balance test with real tape, placebo tape, and no tape. They found no significant difference in the performance of each task and reported the importance of continuing to use tape even if no significant positive benefit was found biomechanically or from a performance perspective. By maximizing the patient’s trust and confidence in the taping technique, this belief may somehow positively contribute to injury prevention[7]. The negative perspective must also be considered as a potential belief system. If the individual views the use of tape as a weakness, a reminder of their injury or inability to perform at their pre-injury level, the negative psychological aspect may have a detrimental effect. Again, further study may be beneficial to expand and analyse this concept.The effectiveness, or lack thereof in some cases, has been questioned due to time and cost factors but also due to the fact that the tape often loosens very quickly losing much of its restrictive properties fairly quickly. Wilkerson et al.[17] found inconsistent results on the effectiveness of ankle taping for ankle protection. When analysing the kinematics of the possible effects of tape, the force vectors created by tension within the various taping strips and the actual type of technique used was inconsistent. They concluded that the force vectors produced by the tape may be crucial to the influence on the degree of motion that is restrained and the possible effects of the taping technique.Reports also question the use of tape due to the possible detrimental effects on performance and function. Burks et al.[8] reported that the use of tape significantly decreased vertical jumping height and the time to complete a 10 yard shuttle run and 40 yard sprint. This seems to contradict other reports that have not found negative effects of tape application but again highlights the inconsistency and contradictory findings. Possible explanations for the contradictory findings could be related to the fact that different methodologies and study designs were used. In some cases, athletic versus non-athletic subjects or healthy versus injured individuals were included in the study. In many cases different types of taping techniques may also have been used and the amount of force used when laying down the tape may not have been consistent and this may have added to the measurement error and contributed to the contradictory findings.In this study, following 30 minutes of sport specific physical activity most participants demonstrated a decrease in ankle strength upon retesting during the first testing session. Generally this finding would be expected due to fatigue factors as a possible explanation. A common trend, however, that was not statistically significant but may be clinically relevant, is that there was an increase in strength upon retesting following activity during the second testing session for dorsiflexion, inversion and eversion with the application of tape. Most strength values were also higher on the dominant leg (with and without tape) when compared to the non-dominant leg. Plantarflexion strength was decreased both with and without taping after the sport specific physical activity but it decreased less with the application of tape during the second testing session. This difference was not significant in this study but is an interesting finding that should also be highlighted. Another contradictory finding that weakens any inferences that can be made is the fact that participants also demonstrated an increase in strength for dorsiflexion and eversion without tape during the second testing session. Again, the reason for these findings cannot be conclusively stated but opens up the discussion for further study. Future studies are warranted and should continue to examine the use of tape but should consider several design changes. By standardizing the amount of force provided with each strip of tape, varying the type of tape used, increasing the sample size, including participants that are involved in other jumping types of sports (e.g. volleyball players) and including symptomatic individuals with ankle injuries may provide further information of the effect of tape to see if the trends described are in fact correct and clinically significant. There are several limitations in this study that must be reported and addressed. The sample size for this study included only 15 participants who were high level athletes and this effects the external validity of the findings. These results cannot be generalized beyond those who were involved in this study. The sample population tested included only varsity basketball players; so, these results cannot be generalized to other sports or the non-athletic population. A larger and more diverse sample would allow for better inferences to be made and for the results to be more generalized. Motivation and the degree of effort imparted by the subject is another extraneous variable in this study that must also be considered. Although participants were asked to maximally contract during strength testing this may not have been the case and affected the results. Other extraneous variables that must be considered that may have affected the results of this study was the effect of time between testing sessions, fatigue introduced from academic, practice, game, and travel time and commitments, and measurement error with the use of the manual muscle tester to measure ankle strength. Although testing sessions were scheduled as close together as possible and a standard methodology was used to try to minimize these effects on the results of this study, we cannot completely disregard their possible effect in this study.Another consideration for future study or methodological changes may be to schedule testing during the athletes’ off season to decrease variability and the effect of other extraneous variables described above that may have affected the results. As well, alternative methods of measuring ankle strength could be explored so that the findings are representative of the true effect of ankle tape on ankle strength. Future studies should also further explore if these findings are sport specific or if they can be generalized to other sports. This study could be repeated using other athletes in jumping sports to see if similar findings are also found. Different taping techniques and types of tape may also impact on ankle strength differently[18]. The inclusion of participants with current ankle sprains/injuries to examine the effect tape on ankle strength may also produce some interesting findings.
5. Conclusions
- Ankle taping did not have a significant effect on ankle strength in varsity basketball players before and after 30 minutes of sport specific physical activity. This contradicts research that commonly suggests that tape may have a negative impact on sport performance and strength. The clinical implication of this is that if the patient or athlete reports subjective improvement and believes in the utility of the tape then it should be considered as a possible adjunct for treatment without concern for negative effects on ankle strength.
ACKNOWLEDGEMENTS
- We would like to thank the research participants from the university men’s and women’s varsity basketball teams for their participation in this study.