-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2013; 3(4): 127-131
doi:10.5923/j.sports.20130304.05
Glenohumeral and Scapular Adaptations in Overhead Throwing Athletes
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRibeiro A.1, 2, Silva C.1, Antunes H.1, Rodrigues M.1
1Physiotherapy Department, Instituto Superior Saúde Alto Ave, Póvoa de Lanhoso, Portugal
2Interdisciplinary Centre of Health Sciences(CICS), Póvoa de Lanhoso, Portugal
Correspondence to: Ribeiro A., Physiotherapy Department, Instituto Superior Saúde Alto Ave, Póvoa de Lanhoso, Portugal.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
In overhead athletes, the shoulder complex joint is strongly required especially during movements of external rotation with abduction. This makes these athletes suffer adaptations both in bone and inert structures.The purpose of our study was to evaluate shoulder axial rotation, scapular upward rotation and protraction of three different groups, team-handball players, swimmers and a control group. Thirty-three male participants, divided into three groups (handball, swimming and, control), aged between 16 and 36 years. Handball players present a lower total arc of motion (TRM), thedifferences found are statistically significant (P = 0.003).Regarding protraction, differences were observed concerning the dominant member both in handball and swimming athletes in resting position (0°, P = 0.007);between the handball and control group (P = 0.005) at 45° of abduction; at 90° of abduction, differences were found between the handball and swimming group (P =0.004) and the handball and control group (P = 0.017). Swimmers are those with higher values of scapular superior rotation in both members.The Handball player’s presented lower internal rotation values; however, theydid not present external rotation gains. These athletes present higher scapular protraction. In this group we found changes that are common in overhead athletes with many years of practice or injured subjects.
Keywords: Scapula, Shoulder, Team-Handball, Swimmers
Cite this paper: Ribeiro A., Silva C., Antunes H., Rodrigues M., Glenohumeral and Scapular Adaptations in Overhead Throwing Athletes, International Journal of Sports Science, Vol. 3 No. 4, 2013, pp. 127-131. doi: 10.5923/j.sports.20130304.05.
Article Outline
1. Introduction
- The shoulder complex demonstrates great mobility while compared with other joints, but at same time allows a stable base for the upper limb. The synchronized rhythm between the humerus and scapula has been described as scapulo-humeral rhythm[1]. This is a complex interaction which may be affected by speed or external load[2]. According to Kibler et al[3] scapula is fundamental to shoulder complex movement, functioning as stable base for the rotator cuff muscles during the throwing motion. The presence of injury in soft tissues or bone or even muscular weakness can lead to scapular dyskinesis[3, 4]. For Ludewig et al[5] scapular dyskinesis is due to static and dynamic changes in movement. The overhead throwing athlete seems to demonstrate functional and structural adaptations on their shoulders in order to promote the best sports gesture and achieve the best performance.Myers et al[6] say that these alterations induce changes in scapulohumeral rhythm (SHR) and also to scapular kinematics. According to Burkhart et al[7] posterior capsule tightness can increase stiffness at glenohumeral joint limiting internal rotation. Some of the functional adaptions of the overhead throwing athlete, seen in literature are internal rotation deficit and an external rotation increase[8, 9, and 10]. The direct cause of these adaptations is not yet known. Some believe that the external rotation gain is due to anterior capsular stretching[8], others believe that the glenohumeral internal rotation deficit (GIRD) is due to posterior capsular tightness[7]. An adequate scapular positioning allows a good relationship between tension and length reducing the rotator cuff energy needs during upper limb motion[11]. Considering shoulder adaptations of overhead throwing athletes we hypothesized that different sports could induce different shoulder adaptions. Thus the purpose of our study was to evaluate shoulder axial rotation, scapular upward rotation and protraction of three different groups, team-handball players, swimmers and a control group.
2. Methods
- The independent variables were sport (swimming, team-handball and control group), number of hours of sports practice. Both the dominant and nondominant arms of participants were measured and compared bilaterally. Dominance was defined by the hand the athlete used the most, during sports practice, writing and eating (daily living activities).The dominant arm was defined as the Measurements were taken using a digital inclinometer (Baseline) and a goniometer. The dependent variables were glenohumeral internal rotation (IR), glenohumeral external rotation (ER), total glenohumeral rotation, scapular upward rotation[0º (at rest), 60º, 90º and 120º of glenohumeral abduction] scapular protraction [0º (at rest), 45º (hands on hips), and 90º glenohumeral abduction]. Total glenohumeral rotation range-of-motion was calculated as internal rotation plus external rotation with the dominant and nondominant arms grouped together. The glenohumeral internal rotation deficit was calculated dominant limb less nondominant limb[12].
2.1. Participants
- Thirty-three male subjects volunteered to participate in this study: 11 team-handball players, (24.5±1.55 years; 84.7±3.11 kg; 185.3±0.02 cm), 11 swimmers (17.82±0.52 years; 67.8±2.1 kg; 177.7±0.02 cm) and control group, 11 non-athletes (25±1.16 years; 79.8±2.8 kg; 182.0±0.02 cm). All subjects had to meet inclusion criteria such as being male subjects and no shoulder injuries. All subjects had at least 7 years of practice. Prior to each evaluation all subjects fulfilled an evaluation query together with an informed consent declaration. The study was approved by the Scientific Council of the Superior Health Institute.
2.2. Procedures
- Glenohumeral IR and ER Assessment: Passive internalrotation and external rotation measurements were takenwith the participant in the supine position and the glenohumeral joint in 90ºof abduction. Next, the scapulawas stabilized by the tester’s hand, and the arm was rotateduntil scapular motion was detected. The inclinometer wasplaced on the dorsal surface of the forearm, and the holdbutton was pressed to record the measurement. Thisprocess was repeated 3 times, and the average of the 3measurements was used. All measurements were taken bilaterally by the primary investigator, and the participantsdid not perform warm-ups before the measurements. Theprimary investigator was blinded to the arm dominance of each athlete, and the right arm was tested first.Scapular Upward Rotation Assessment: Scapular upward rotation measurements were taken with the participant standing with normal relaxed posture. A guide pole was used to help position the participant’s arm at 60º, 90º, and 120º of abduction. When the appropriate amount of abduction was determined, a pin was inserted into the guide pole, and that location was recorded for consistency in the postseason measurement. The participant was asked to abduct her arm until it was positioned against the pin.This position was maintained until the measurement was recorded. Next, the lateral arm of the inclinometer was placed over the posterior lateral acromion, and the medi alarm was placed over the root of the scapular spine. The hold button was pressed to record the measurement. This was repeated twice, and the average of the 2 measurements was used. All measurements were taken bilaterally by the primary investigator, and the participants did not perform warm-ups before the measurements. The primary investigator was blinded to the arm dominance of each athlete, and the order of testing was alternated.Scapular Protraction Assessment: Scapular protraction measurements were taken with the participant standing with normal relaxed posture. The measurements were performed at 3 positions (0º [rest], 45º [hands on hips], and 90º of glenohumeral abduction with maximum IR). First, the inferior angle of the scapula was palpated, and the lateral arm of the calliper was placed atthe tip of the inferior angle. The medial arm of the calliper was positioned at the corresponding spinous process, andthe measurement was recorded. This was repeated 3 times,and the average of the measurements was used. All measurements were taken bilaterally by the primary investigator, and the participants did not perform warmups before the measurements. The primary investigator was blinded to the arm dominance of each athlete, and the order of testing was alternated. A One way- ANOVA was performed to calculate differences between groups. The α as set a priory at 0.05. Post hoc Tukey tests were performed to compare differences between groups.
3. Results
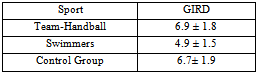
- Results for ICC and SEM for external rotation were 0.991 and 0.001 and for internal rotation 0.994 and 0.001 respectively. Internal rotation seems to be higher in control and swimmer groups while compared with team-handball athletes (Figure 1).All groups demonstrated higher values of external rotation in the dominant arm while compared with the non-dominant (figure 2).We found statistically significant differences in dominant (P=0.006) and non-dominant shoulders (P=0.0011). The Post hoc Tuckey test revealed statistically significant differences between team-handball and swimmers (P=0.026) and team-handball and control group (P=0.007) when internal rotation was considered.Concerning non-dominant shoulder we found differences between team-handball and control group (P=0.008).No differences were found between groups considering GIRD.
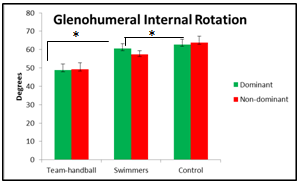 | Figure 1. Dominant and non-dominant Glenohumeral Internal Rotation (Mean, SEM), * values statistically significant |
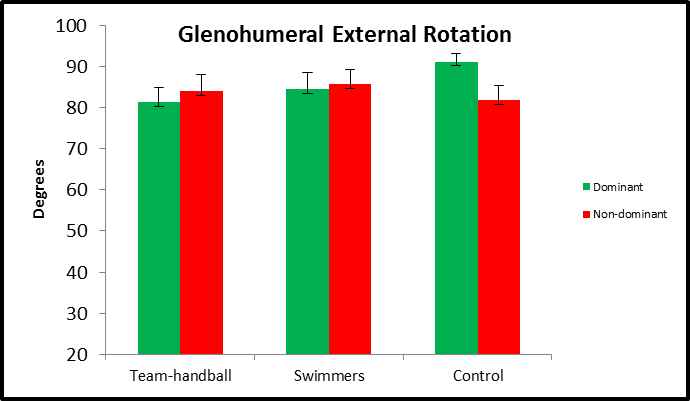 | Figure 2. Dominant and non-dominant Glenohumeral External Rotation (Mean, SEM)* values statistically significant |
|
|
|
4. Discussion
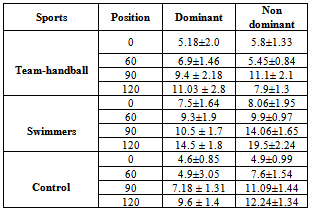
- We found differences between the studied groups concerning glenohumeral internal rotation. So, and according to literature, we found that team-handball players presented less range-of-motion when compared to control group or even when compared to swimmers[13, 14, 15, and 16]. Nevertheless and in opposition to literature, swimmers did not show any differences when compared to non-athletes[17]. None of the studied groups demonstrated glenohumeral internal rotation deficit (GIRD), besides the fact that team-handball players demonstrated less internal rotation than the other groups, they did not show any indicators of GIRD which may be shoulder protective[16, 18]. Concerning the total range-of-motion we found statistical significant differences between team-handball and control group in dominant shoulder. These athletes show less internal rotation but and in opposition to literature they did not demonstrate external rotation gain[13].Scapular upward rotationScapular dyskinesis is usually associated to shoulder dysfunction in overhead throwing athletes[7]. A reduced scapular upward rotation seems to shorten the subacromial space and may be related to impingement at highest glenohumeral abduction degrees. Using a digital inclinometer, several investigators started to objectively measure upward scapular rotation in overhead throwing athletes. Our results did not reveal differences between the three groups. Scapular protractionScapular protraction is important for the athlete performance. During acceleration and follow-through phases scapula should protract to dissipate forces applied to glenohumeral joint[3]. Recent studies[19] showed that an increase in scapular protraction induces less strength in rotator cuff muscles. This decrease occurs because scapula cannot act as a stable base for the rotator cuff function increasing injury risk of the glenohumeral joint. In our study, team-handball players were the ones who showed a more protracted scapula which seems to increase the risk of injury. In these athletes we found alterations which are common in high level overhead throwing athletes, the same was not found in swimmers or even in control group.
5. Conclusions
- Team-handball players present less internal rotation than swimmers or control group, but did not show external rotation gain.Swimmers were the ones who presented higehst values of scapular upward rotation in both shoulder. clinically this data may indicate that these athletes may no be developing adaptations on scapular stabilizers due to sports practice.Team-handball players were the ones who presented a scapula more in protraction which seems to predispose to injury be inhibiting a proper scapular function.