-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2013; 3(2): 46-50
doi:10.5923/j.sports.20130302.02
Physical Activity Improves Cognition in Elderly without Relation with Dominant Intelligence and Scholarity
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLElisangela Naves Vivas Corrêa1, Gustavo Ribeiro da Mota2, Natália Medeiros1, Moacir Marocolo2, Sérgio de Figueiredo Rocha1, 3
1Department of Sciences of Physical Education and Health, Federal University of São João del Rei, São João del Rei, MG, Brazil
2Post-Graduation Program in Physical Education and Sport, Federal University of Triângulo Mineiro, Uberaba, MG, Brazil
3Department of Music, Federal University of São João del Rei, São João del Rei, MG, Brazil
Correspondence to: Gustavo Ribeiro da Mota, Post-Graduation Program in Physical Education and Sport, Federal University of Triângulo Mineiro, Uberaba, MG, Brazil.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
The preservation of cognition function in the aging process is fundamental for the autonomy of the elderly. Thus, the aim of this study was to verify if physical activity improves cognition function in elderly and if the dominant intelligence and scholarity grade could influence this process. Sixteen elderly women sedentary (65.3 ± 3 years) participated of a physical activity program lasted three month. Aerobics exercises, stretching, strength activities and recreational were undertaken three times a week in alternate days. The results showed that Physical activity increased in ± 12.9% (α = 0.01) the cognition function (CAMCOG-R). Such development was not related with dominant intelligence neither with scholarity grade (α = 0.05). Therefore, we conclude that physical activity improves cognition function in elderly, without neither dominant intelligence nor scholarity grade influences.
Keywords: Exercise, Cognitive Function, Well Being
Cite this paper: Elisangela Naves Vivas Corrêa, Gustavo Ribeiro da Mota, Natália Medeiros, Moacir Marocolo, Sérgio de Figueiredo Rocha, Physical Activity Improves Cognition in Elderly without Relation with Dominant Intelligence and Scholarity, International Journal of Sports Science, Vol. 3 No. 2, 2013, pp. 46-50. doi: 10.5923/j.sports.20130302.02.
Article Outline
1. Introduction
- The worldwide increase in life expectancy has aroused considerable interest in the impact of physical activity (PA) on both quality of life and the aging process. There is no doubt that PA promotes beneficial effects on physical aspects, such as muscle strength/balance[1], and that these changes can improve quality of life, contributing positively to healthy and successful aging in later life[2],[3],[4]. In addition to improved physical capacity, regular PA can improve and preserve cognitive function and autonomy among elderly people[2]. Human autonomy is managed by the central nervous system, and preservation of cognitive function helps individuals maintain a good quality of life as they age. However, since the publication of the theory of multiple intelligences, the use of the term ‘cognitive function’ in the singular form makes us feel at least uncomfortable. It is known that there are various types of intelligences (musical, spatial, logical-mathematical, linguistic, bodily-kinesthetic, interpersonal, existential and naturalistic), all of which are expressed by different dominances that vary from individual to individual[5]. Regular PA in elderly adults contributes positively to cognitive functions[6], including the ‘intelligences’.Moreover, there seems to be a beneficial effect leading to an increase in neuronal connections (neuronal plasticity), which can optimize the process of maintaining cognitive functions. Thus, one might assume that PA, in theory, should contribute to the improvement of different intelligences by potentiating neuronal networks. Although the relationship between PA and cognition function is well documented[2],[6], the same is not true for the hypothesis that different types of ‘intelligences’, according to individual dominance, would contribute differently to the impact of PA on cognition function, in order to further increase the ‘cognitive reserve’ in later life[7]. Once that cognition evaluating tests depends, in part, on the scholarity and dominant intelligence, would be reasonable to speculate that higher cognition function scores would be obtained by people with better level education[8]. Additionally, to our knowledge, no study has investigated whether the level of education and/or a particular type of dominant intelligence would determine significant differences in cognitive performance in the elderly population. Thus, the objective of this study was to investigate whether regular PA can improve cognition function in previously sedentary elderly women and whether dominant intelligence and level of education may influence this process.
2. Materials and Methods
- This study was approved by local Ethics Committee and was performed in accordance with the provisions of the Declaration of Helsinki. All volunteers were informed of the procedures, objectives and potential risks, and written informed consent was obtained. Sample and subject selectionThe subjects were recruited (from April to October 2009) by advertising for volunteers at local community (São João del Rei, MG, Brazil). To participate the volunteers should attend the following inclusion/exclusion criteria: having a sedentary lifestyle (PA carried out no more than once a week), having no contraindications according to the Physical Activity Readiness Questionnaire (PAR-Q)[9], being physically independent – level III[10], being aged 60 to 70 years, having no acute or chronic diseases that could prevent PA, being authorized to perform PA (after medical examination by a qualified physician), being diagnosed as not having dementia[11], and having attended at least three years of elementary school, thus being able to read and interpret simple sentences (items of the cognitive test). Of 25 candidates, 20 met the eligibility criteria and were selected to participate, but only 16 completed the study (65.3 ± 3 years; 70.1 ± 11.2 kg of body mass and 1.59 ± 10.9 m of height). Tests for cognitive function and status The Mini-Mental State Exam was used to assess cognitive status[11]. The Brazilian version of the Cambridge Cognitive Examination-Revised (CAMCOG-R) was used to asses cognitive functions[12]. In brief, CAMCOG-R is a neuropsychological test battery to assess multiple cognitive functions consisting of 69 items, divided into nine sections and spend about twenty minutes to be completed. Physical fitness tests The following tests were performed: stationary walking, 30-second chair stand, hip flexibility, and static balance[13],[14]. At the end of the study period (three months), the same (cognitive and motor) tests were performed under the same conditions. Multiple intelligence test This test is based on the model of multiple intelligences proposed by Howard Gardner[5] to identify each individual’s dominant intelligence, aiming to detect the strengths and potential of the individual’s particular intelligence type. For this purpose, the answers for each of the 70 questions are scored from 1 to 4, where the highest score indicates the type of intelligence related to the question. Physical activity programThe PA program was designed to stimulate several physical and mental abilities. The elderly participated in a PA program consisting of 60-minute exercise classes, 3 times a week (on alternate days), as follows: aerobic activities – 20 to 30 minutes at 60 to 80% of maximum heart rate (HRmax); muscle strength activities – 8 exercises for large muscle groups, 2 to 3 sets of 8 to 12 repetitions, with a 90-seconds rest between sets; flexibility – stretching before and after exercise classes; and balance, coordination, spatiotemporal activity, and rhythm – various recreational and pedagogical activities. Level of education vs. performance on the CAMCOG-RTo assess the impact of the variable ‘level of education’, the sample was divided according to the median years of schooling in order to obtain a subgroup with ≤ 5 years and one subgroup with > 5 years of schooling, thereby allowing us to perform paired comparisons. Dominant intelligence vs. performance on the CAMCOG-RTo investigate whether PA would have a different impact on cognition function according to each individual’s dominant intelligence, two groups of 5 subjects each were formed for musical and interpersonal intelligences, whereas the remaining intelligence types were represented by at least two individuals. Statistical analysisThe Kruskal-Wallis test was used for statistical analysis because it is suitable for small samples with asymmetrical distribution. A one-tailed t test for dependent samples was used to analyze the impact of the PA program on cognition function, since the sample was monitored over three months and then retested. An unpaired t test was used for the comparison of two means of two paired samples. The level of significance was set at 1% (α = 0.01) with a critical t of 3.499 (calculated for 8 subjects per subgroup). The level of significance was set at 1% with a critical t of 2.60.
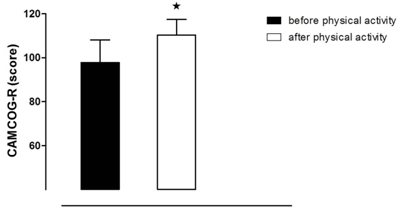 | Figure 1. Effect of physical activity program on CANCOG-R test in older women. Values are mean ± standard deviation.* P < 0.01 vs. before physical activity to the same group (N = 16) |
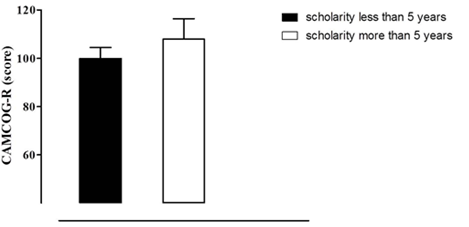 | Figure 2. Effect of scholarity on CANCOG-R test in older women. Values are mean ± standard deviation; N = 08 for each group |
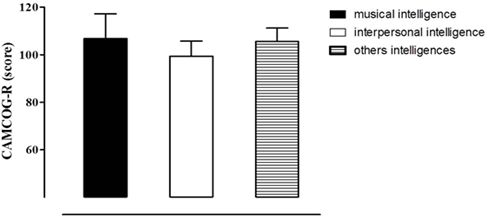 | Figure 3. Effect of dominant intelligence on CANCOG-R test in older women. Values are mean ± standard deviation; N= 05 musical intelligence; 05 interpersonal intelligence and 06 others intelligences |
3. Results
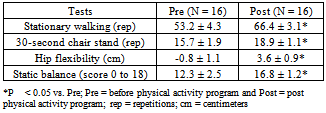
- Of 20 elderly women initially enrolled in the program, only 16 completed all three research phases (baseline assessment, PA program, and reassessment) and were therefore analyzed for this report. Motor performance (stationary walking, 30-second chair stand, flexibility, and static balance) improved significantly (p < 0.05) compared to baseline performance on motor tests (Table 1). The same was observed in the CAMCOG-R, with an approximately 13% improvement (Figure 1). Regarding the level of education and performance on the CAMCOG-R, there was no difference between higher and lower education (Figure 2). Likewise, no difference was detected between dominant intelligence groups in the CAMCOG-R (Figure 3).
4. Discussion
- The main finding of this study is that the PA program was able to improve cognition function (CAMCOG-R), without interference from dominant intelligence or level of education. Such an improvement in cognition has been found in the literature and is likely to be a result, among other factors, of greater functional connectivity between brain regions and increased efficiency of neural networks[6],[15],[16]. It is therefore reasonable to recommend PA programs, like the one described here, to maximize physical and mental performance as well as autonomy among elderly women.
|
 | Figure 4. Analogy to the system of communicating vessels |
5. Conclusions
- Our findings indicate that regular physical activity is able to improve cognition in previously sedentary elderly women, and such improvement may occur even without the influence of dominant intelligence or level of education. The mechanisms underlying these changes need to be further elucidated. However, the theory of multiple intelligences, together with neuronal plasticity, seems to provide a model that may explain the homogeneous trend of the results for our group, despite individual differences.
ACKNOWLEDGMENTS
- This study was supported in part by CAPES (Coordination for the improvement of higher level personnel).