-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Sports Science
p-ISSN: 2169-8759 e-ISSN: 2169-8791
2012; 2(5): 61-67
doi: 10.5923/j.sports.20120205.03
Power-based Resistance Training Reduced Serum Oxidized Low-Density Lipoprotein in Athletes
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-Text HTML
Full-Text HTMLYunsuk Koh, Joshua Miller
Department of Health and Kinesiology, Lamar University, Beaumont, TX 77710, USA
Correspondence to: Yunsuk Koh, Department of Health and Kinesiology, Lamar University, Beaumont, TX 77710, USA.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Power-based resistance training (PRT) allows athletes to improve athletic performance by enhancing both strength and power simultaneously. However, it is unclear whether athletes who participate in PRT can positively alter serum lipid and lipoprotein parameters. Thus, the current study investigated the effects of 6-weeks of PRT on serum lipid and lipoprotein parameters in male and female collegiate athletes. Twenty one collegiate athletes (12 female soccer players and 9 male football players) participated in PRT (4 days/week) for 6 weeks. The PRT program was composed of a variety of Olympic-style and traditional weightlifting movements along with plyometrics. Overnight fasting blood samples were collected before and after 6-weeks of power-based resistance training to analyze serum lipid and lipoprotein parameters including TG, TC, VLDL-C, LDL-C, HDL-C, Lp(a), and ox-LDL. All serum lipid and lipoprotein parameters remained unchanged, except ox-LDL which significantly (p = 0.036) decreased by 3.81% or 1.87 U·L-1 (from 49.05 ± 9.17 to 47.18 ± 9.78 U·L-1) following 6 weeks of power-based resistance training. The 6-weeks of PRT, designed to improve strength and power, can provide cardioprotective health benefits for male and female collegiate athletes by lowering ox-LDL.
Keywords: Blood Lipids, Cardioprotective Benefits, Weight Training, Complex Training
Cite this paper: Yunsuk Koh, Joshua Miller, "Power-based Resistance Training Reduced Serum Oxidized Low-Density Lipoprotein in Athletes", International Journal of Sports Science, Vol. 2 No. 5, 2012, pp. 61-67. doi: 10.5923/j.sports.20120205.03.
Article Outline
1. Introduction
- Cardiovascular disease (CVD) has been recognized as a major leading cause of death in America for more than 10 decades, and approximately 2,200 Americans die of CVD everyday[1]. Abnormal blood lipids and lipoproteins known as dyslipidemia are considered one of the primary risk factors for development of CVD and characterized by elevated total cholesterol (TC), triglycerides (TG), or low-density lipoprotein cholesterol (LDL-C) and lowered high-density lipoprotein cholesterol (HDL-C)[2]. In addition, a strong body of evidence suggests that elevated serum oxidized LDL (ox-LDL) is a key factor that accelerates the incidence of CVD by promoting the atherosclerotic progression of plaque[3]. Physical activity, as a non-pharmacological treatment, is often recommended for sedentary individuals or patients with CVD to positively modify blood lipids and lipoproteins[2]. According to the meta-analysis, aerobic exercise can decrease TC (2.0%), LDL-C (3%), and TG (5.0 – 9.0%) and increase HDL-C (2.0 – 3.0%) in adults[4,5]. However,the effects of anaerobic exercise such as resistance training on blood lipids and lipoproteins are equivocal[6-8]. One meta-analysis has recently reported that resistance exercise may decrease TC (2.7%), LDL-C (4.6%), and TG (6.4%), but not HDL-C, in adults[6], whereas another review study has reported no strong evidence of beneficial effects of resistance exercise on modification of blood lipids and lipoproteins[7]. Moreover, only a few studies have previously examined the responses of ox-LDL to exercise training, and the results are inconsistent[9-12]. American Heart Association and American College of Sport Medicine recommend moderate intensity resistance exercise to be part of the main exercise program for sedentary or untrained individuals because it helps prevent CVD and promote muscular strength and endurance, functional capacity, health, and fitness[7,13,14]. Unlike sedentary or untrained individuals whose main goal of resistance training is to improve their health or fitness, most trained athletes usually participate in relatively higher intensity resistance exercise to promote athletic performance rather than health or fitness. Power-based resistance training (PRT) is often recommended by many strength and conditioning professionals because it allows athletes to enhance athletic performance by gaining both strength and power simultaneously[15]. The recommended form of PRT is a combination of a variety of Olympic-style and traditional weightlifting movements and plyometrics[16]. Several studies have previously reported the positive effects of PRT on improvement in strength and performance in athletes [17-20]. However, it is unclear whether athletes participating in high intensity resistance training such as PRT can obtain cardioprotective health benefits as well. To date, no study has examined the effects of PRT on serum lipids and lipoproteins including ox-LDL in athletes. Thus, the current study investigated whether 6-weeks of PRT can provide male and female collegiate athletes with cardioprotective health benefits.
2. Method
2.1. Participants
- Twenty one collegiate athletes (12 female soccer players and 9 male football players), between 18 and 23 years of age, participated in the study during the off-season. All participants were physically active (defined as a regular physical activity performed more than 4 days a week), free of any self-reported injury and cardiovascular or metabolic diseases, and not taking any medications known to alter blood lipids and lipoproteins. The participants provided written informed consent and the medical history forms prior to performing any study protocols. All study procedures were reviewed and approved by the Institutional Review Board. The participants were encouraged to maintain a normal dietary regimen, and refrained from any types of strenuous exercises other than PRT throughout the study period. In addition, no competitive football or soccer games were scheduled during the study period.
2.2. Procedures
- The participants were tested for one-repetition maximum (1-RM) in clean, incline press, and Olympic-style back squat (angle of knee < 90°) on a separate day to determine the lower and upper body strength. The initial weight for the 1-RM test was determined by the participant’s training history. Once the participants successfully lifted the first weight, additional resistance (2.5 – 5.0 kg) was added until the participants were not able to successfully complete a lift. The participants rested for 3 minutes between each 1-RM attempt to recover from the previous attempt, and the last successful lift was recorded as 1-RM. The 1-RM for other upper and lower body movements was estimated by pre-determined 1-RM of clean, incline press, or squat. For instance, the 1-RM for the following Olympic - style weightlifting movements was estimated by the clean 1-RM; snatch – 60% of clean 1-RM, clean pull – 120% of clean 1-RM, hand clean and Romanian deadlift (RDL)–90% of clean 1-RM, jerk variations – 90% of clean 1-RM, snatch pull – 72 % of clean 1-RM (equivalent to 120% of snatch 1-RM), and hang snatch – 54% of clean 1-RM (equivalent to 90% of snatch 1-RM). The 1-RM for the traditional horizontal bench press was estimated to be 120% of incline press 1-RM. The Olympic-style back squat 1-RM was used to estimate the 1-RM for the front squat (80% of squat 1-RM) and lunge variations (25% of squat 1-RM).
2.3. Power-based Resistance Training (PRT) Program
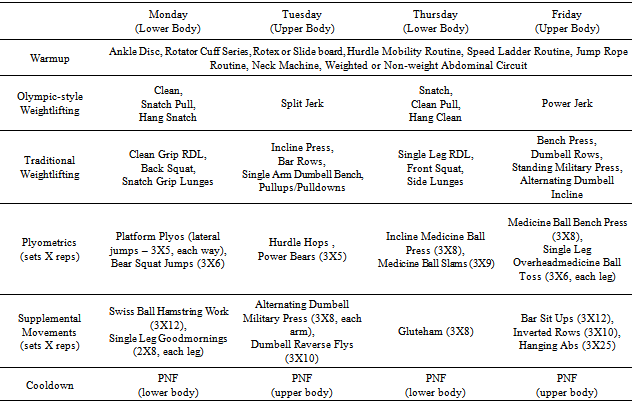
- The PRT program consisted of a combination of various Olympic-style and traditional weightlifting movements along with plyometrics as shown in Table 1. The participants performed PRT for 4 days per week (Monday, Tuesday, Thursday, and Friday) for 6 weeks. After performing a series of selected warm-up activities for 15 minutes, the participants performed each PRT session around 60 minutes. In the current study, following weekly undulating periodization was used; week 1 – 70% 1-RM, week 2 – 80% 1-RM, week 3 – 75% 1-RM, week 4 – 90% 1-RM, week 5 – 80% 1-RM, and week 6 – 95% 1-RM. For a cool-down, a variety of proprioceptive neuromuscular facilitation stretches targeting upper (chest, rotator cuff,deltoids, and upper back) or lower (hamstrings, hips/glutes, lower back, and quadriceps) body muscle groups were performed for 10 minutes after each workout. All PRT sessions were supervised and led by a certified strength and conditioning professional to ensure maximum compliance.
2.4. Analyses of TC, TG, and Ox-LDL
- The participants reported to the laboratory for blood draw between 07:00 and 08:00 AM after 10 – 12 hours of overnight fasting. Blood samples were collected at pre- (week 0) and post-PRT (week 7). After 15 minutes of resting in a chair, venous blood was drawn from the antecubital vein. Immediately after blood draw, blood samples remained at room temperature for 20 minutes to be clotted, and then were centrifuged at 1,800g for 15 minutes to separate serum. Serum samples were then immediately frozen at -80 °C for the further analysis of serum lipid and lipoprotein parameters. Serum samples in duplicate were assayed for TC (Kit# 85430, Cliniqa, San Marcos, CA) and TG (Kit# 85460, Cliniqa, San Marcos, CA) by an enzymatic colorimetric method, and ox-LDL was analyzed by an enzyme-linked immumosorbent assay (Cat# 10-1143-01, Mercodia, Uppsala, Sweden). Optical density was measured by the Spectra Max Plus 384 microplate spectrophotometer (Molecular Devices, Sunnyvale, CA). Each assay was performed as instructed by the manufacture’s assay procedure. To minimize inter- and intra-assay variability, all serum samples for each assay were analyzed at one time in a single plate.
2.5. Analyses of Serum Lipoprotein-cholesterol
- Serum lipoprotein-cholesterol including VLDL-C, LDL-C, HDL-C, and Lp(a) were analyzed by electrophoresis (Cat. # 3438 SPIFE Vis Cholesterol, Helena Laboratory, Beaumont, TX) using the SPIFE 3000 electrophoresis system (Helena Laboratory, Beaumont, TX). The lipoprotein-cholesterol analysis was performed as instructed by the manufacture’s assay procedures, using a commercially available control (Cat. # 3218, Helena Laboratory, Beaumont, TX). In brief, 80 μL of serum samples, in duplicate, were applied to an agarose gel followed by 20 minutes of electrophoresis at 16 °C with 400 volts. After applying a staining regent (Cat. # 3438, Helena Laboratory, Beaumont, TX), additional electrophoresis was performed at 30 °C for 15 minutes. The gel was washed and dried at 70 °C for 20 minutes, and the density of stained lipoprotein-cholesterol bands were measured in a scanning densitometer (Epson Perfection V 700, Long beach, CA) using Quick Scan 2000 software (Helena Laboratory, Beaumont, TX). To minimize inter- and intra-assay variability, all serum samples were analyzed at one time in a single gel.
2.6. Statistical Analyses
- The sample size was calculated by G*Power 3.1.0 software[21], given an alpha level at 0.05, an effect size of 0.40, and power at 0.80. The appropriate sample size was estimated to be 16 participants for the current study design. All statistical analyses were performed using the IBM Statistical Package for the Social Sciences 19.0 (IBM SPSS, Armonk, NY) and reported as mean ± standard deviation (SD) unless stated otherwise. The Shapiro-Wilk test was employed to test the normality of data, and indicated that data were normally distributed. An independent-Samples T test was used to examine the baseline differences in anthropometrical and physiological variables between males and females. A 2 (group; males and females) X 2 (time; pre- and post-PRT) repeated measures analysis of variance (ANOVA) was employed to determine the significant changes in serum lipid and lipoprotein parameters. If the main or interaction effects were significant, Bonferroni pairwise comparisons were conducted to examine the significant mean differences. A p-value < 0.05 was considered to be statistically significant.
3. Results
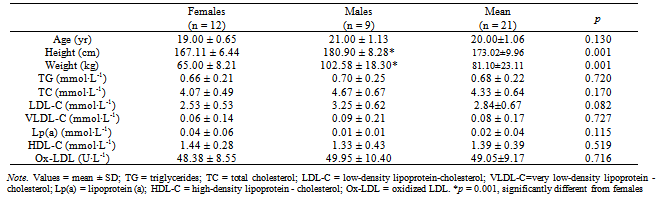
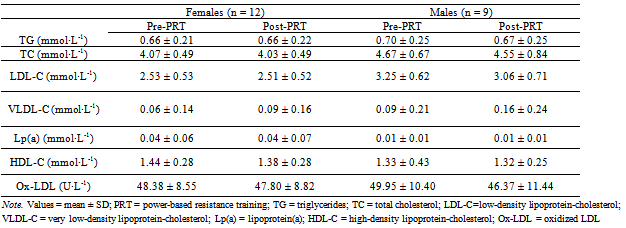
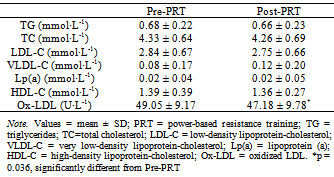
- The demographic and physiological characteristics of participants at baseline are presented in Table 2. No serum lipid or lipoprotein parameters at baseline were significantly different between groups, whereas height (males: 180.90 ± 8.28 vs. females: 167.11 ± 6.44 cm) and weight (males: 102.58±18.30 vs. females: 65.00±8.21 kg) were significantly different (p=0.001).However, these anthropometric variables were not significantly altered within each group following 6-weeks of PRT.The main effects for group and time on changes in serum lipids and lipoproteins are presented in Table 3 and 4, respectively. There were no significant main effects for group and time or the group X time interaction for any of the serum lipid or lipoprotein parameters, except ox-LDL which had a significant main effect for time, indicating that ox-LDL significantly (p = 0.036) decreased by 1.87 U·L-1 or 3.81% (from 49.05 ± 9.17 to 47.18 ± 9.78 U·L-1) following 6 weeks of PRT (Table 4).
|
|
|
4. Discussion
- This study was the first to examine the effects of PRT on cardioprotective health benefits in male and female collegiate athletes. Although we do not discuss about the results of PRT-induced strength gain in this paper, our unpublished data have shown that the participants significantly improved upper and lower body strength up to 15.0% following 6-weeks of PRT.In the current study, no serum lipid or lipoprotein parameters, except ox-LDL, significantly changed following 6-weeks of PRT. This result was consistent with other previous studies reporting that resistant training lasting for up to 16 weeks improved upper and lower body strength, but did not significantly alter serum lipids and lipoproteins in a variety of subject groups including untrained men[22] and women[23], patients with type 2 diabetes[24], obese individuals with CVD risk factors[25], or postmenopausal women[26]. Some studies that examined the effects of different intensities or repetitions of resistance training on serum lipids and lipoproteins in men or women have also found no beneficial effects of resistance training[27-29]. Moreover, several studies have reported an exercise-induced increase in Lp(a) or TG following 24 weeks of low-intensity resistance training or a single session of circuit-resistance exercise[27,29]. In contrast, other studies have reported a favorable effect of resistance training on serum lipids and lipoproteins including a decrease in TC, LDL-C, and TG and/or an increase in HDL-C[30-32]. For instance, sedentary women who participated in 3-days of non-consecutive resistant training (85% 1-RM) for 14 weeks decreased TC, LDL-C, and the TC to HDL-C ratio, increased HDL-C, but did not change TG[32]. Similar results have also been observed in obese women who participated in 9-weeks of resistance training; however, the TG concentration in obese women significantly increased following resistance training[30]. Another study examining the effects of high intensity resistance training (3 sets of 8 repetitions) has reported an increase in HDL-C and a decrease in TG without changing body weight or diet in healthy, active postmenopausal women[31]. Based on the previous studies, it is difficult to conclude whether resistance training can positively alter serum lipids and lipoproteins. One of the recent review papers has suggested that if resistance training could positively influence on serum lipids and lipoproteins, the primary outcome would be a reduction of LDL-C for both men and women, with a reduction of TC being a secondary outcome for only women[33]. One of the possible explanations for the lack of significant changes in serum lipids and lipoproteins in the current study may be our participants’ good training background. All participants in the current study were physically active (performed physical activity more than 4 days per week) and trained for many years. Most studies that have reported a significant change in serum lipids and lipoproteins investigated in sedentary or untrained individuals. Additionally, the initial serum lipid and lipoprotein parameters at baseline for our participants were within the normal range.Only a few studies have previously examined the effects of exercise training on ox-LDL metabolism, and most of the studies employed aerobic exercise training as an intervention [9-12]. Furthermore, the results of these studies are inconsistent. The concentration of ox-LDL decreased after acute prolonged or moderate intensity aerobic exercise training in healthy[10] and obese[9] individuals. However, individuals with some types of metabolic diseases such as untreated mild hypertension with atherogenic lipid profiles[11] or type II diabetes[12] increased ox-LDL following acute resistance exercise. The authors have speculated that one of the possible explanations for an increase in ox-LDL following resistance training observed in patients with metabolic diseases could be a compensatory mechanism to preventing free radical tissue damage[12]. In the current study, the serum ox-LDL concentration was significantly reduced by 3.81% (or 1.87 U·L-1) following 6-weeks of PRT. Similar to the current study, only serum ox-LDL, but no other lipid or lipoprotein parameters, significantly decreased after high-intensity strength training in obese adults[9] that performed lower body strength training for 12 weeks at 90% of 1-RM along with several abdominal and back exercises consisting of 3 series of 30 repetitions[9]. According to several studies that examined the relationship between physical training status and ox-LDL levels in young female[34] and veteran endurance male[35] athletes, the trained athletes tend to have lower ox-LDL than their untrained counterparts, suggesting that atherogenic risk can be favorably influenced by participation in exercise training and affected as early as in adolescents[34].
5. Conclusions
- Our study suggests that 6-weeks of PRT consisting of a combination of Olympic-style and traditional weightlifting movements and plyometrics can provide collegiate athletes with cardioprotective health benefits by lowering ox-LDL. Although the exact mechanism by which exercise decreases ox-LDL has not been fully understood, high-intensity resistance training such as PRT may prevent risk for atherosclerosis and CVD in individuals without atherogenic risk factors.