-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Sociological Research
p-ISSN: 2166-5443 e-ISSN: 2166-5451
2017; 7(4): 109-116
doi:10.5923/j.sociology.20170704.02

Contraceptive Use, Method Choice and Discontinuation of Contraception in South Asia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMd Kamrul Islam
Department of Population Sciences, University of Dhaka, Bangladesh
Correspondence to: Md Kamrul Islam, Department of Population Sciences, University of Dhaka, Bangladesh.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Family planning programmes have received paramount importance in South Asia because of their large number of population and high fertility rates. The objective of this study was to examine differentials in contraception use, method choice and discontinuation of contraception among currently married women aged 15-49 in two countries of South Asia: Bangladesh and India. Using data from the 2014 Bangladesh Demographic and Health Survey and the 2005-2006 National Family Health Survey of India, it was found that significant variations existed in contraceptive use, method choice and discontinuation across women’s demographic, socioeconomic and cultural factors. Women in Bangladesh were more likely to use contraceptive than their counterparts in India. However, there was no significant difference in the use of modern methods of contraception between these two countries. Nevertheless, women in Bangladesh had much higher rate of discontinuation of contraception than their counterparts in India. Overall, findings suggest that emphasis should be given on improving socioeconomic conditions of women and greater investment in advocacy, information and communication for increasing contraceptive use, use of methods, and reducing contraceptive discontinuation.
Keywords: Contraceptive use, Modern method, Discontinuation, Bangladesh, India
Cite this paper: Md Kamrul Islam, Contraceptive Use, Method Choice and Discontinuation of Contraception in South Asia, American Journal of Sociological Research, Vol. 7 No. 4, 2017, pp. 109-116. doi: 10.5923/j.sociology.20170704.02.
Article Outline
1. Introduction
- Family planning programmes have received inordinate attention in developing countries with a widespread optimism that large scale distribution of contraceptives would help reducing population growth and high fertility and consequently contribute to improve standard of living, health status of women, and reduce unintended pregnancies and abortion [1-3]. South Asian countries including Bangladesh and India were not exceptions in this case. A large body of research has examined various aspects of the family planning programmes and contraceptive dynamics in South Asia [4-7]. Majority research found that women’s sociodemographic, economic, cultural and spatial characteristics were the major predictors of contraceptive use. Partner’s opposition to use, health concerns and fear of side effects were reported to be major obstacles in using modern methods of contraception. Modern methods of contraception include pill, injectables, condom, female sterilization, male sterilization, IUD, and Implants.Studies on contraceptive use and discontinuation of contraception in South Asia have given limited attention in multi-country analysis with few notable exceptions [8, 9]. Within this context this study draws on cross-sectional data from Bangladesh, and India to address these gaps in evidence and to answer the following questions: (1) to what extent use of contraceptives (any method), use of modern method, and discontinuation of contraception vary across women’s background characteristics in Bangladesh and India? and (2) to what extent use of contraception, use of modern method, and discontinuation of contraception vary between the two countries in South Asia. Addressing these research questions will contribute to generate effective policy interventions to increase contraceptive prevalence rate and to decrease discontinuation rate of contraception. The Demographic and Health Surveys (DHS) of Bangladesh and the National Family Health Survey (NFHS) of India are well suited for examining the dynamics of contraceptive use and contraceptive discontinuation in Bangladesh and India.
1.1. Determinants of Contraception Use and Method Choice
- Identifying the determinants of contraceptive use is complex because the decision to use contraceptive is influenced by wide range of issues including psychological, social and cultural factors [10]. Most research on the determinants of contraceptive use reveal that demographic and socioeconomic factors are strong predictors of contraceptive use. Among demographic factors women’s age, age at first marriage, and number of living children exert strong influence on the their decision to use contraceptives [11, 12]. On the other hand, socioeconomic factors, such as education, employment status, economic status, and place of living determine the extent to which women can take decision of contraceptive use and avail those [5, 13, 14]. With few exceptions, the findings of the previous research suggests that women with lower socioeconomic status are less likely to use contraceptives due to their lack of knowledge about sources and methods of contraceptive, lack of awareness about negative consequences of having more children on their health and career, lower role in decision making regarding using contraceptives, and lack of capability to purchase modern contraceptives [15, 16]. Hence, Richard Easterlin’s theory of fertility recognized the substantial cost of birth control which might work as a deterrent for using contraceptives [17, 18]. Concerning the role of media exposure, there is evidence that women who have access to newspaper, radio and television are more likely to use contraceptives [13, 19]. Some studies have separately looked at the determinants of modern contraceptive utilization. Majority of these studies found that women’s demographic (age, age at first marriage, number of living children, desire to have children after certain years) and socioeconomic factors (education, employment, income/wealth status, husband’s education, place of residence) were the major determinants of modern contraceptive utilization [12, 20]. For instance, monthly family income and number of living children were significantly associated with the use of modern contraceptives. Desire for more children, husband’s approval, and couple’s discussion about family planning issues exerted strong influence on the decision to use modern contraceptives [12]. Furthermore, favourable opening hours of the facilities and distance to health facilities influenced the use of modern contraceptives [21].
1.2. Determinants of Contraception Discontinuation
- The success of family planning programmes across developing countries facing new challenges due to higher rate of discontinuation of contraception among couples which has wide range of consequences on miscarriage, still birth or abortion, and untended pregnancy [22]. Findings from recent studies indicate that there are substantial variations in discontinuation rate across women’s demographic, socioeconomic and cultural factors. There are several causes of the discontinuation including reported failure, method-related reasons (e.g., dissatisfaction/inconvenient), side effects or health concerns, desire for pregnancy, no further need, partner opposed, higher cost, and access problem [23, 24]. In some cases many women were not prepared to endure the discomfort, inconvenience, and side effects of modem methods, and much need to try several of them before finding one that was suitable [4]. In addition, some studies indicate that discontinuation of contraceptive use is significantly influenced by contraceptive service availability, quality and community context [24, 25]. For example, household outreach in Bangladesh had a pronounced positive net effect on contraceptive continuation. The discontinuation rates vary across various methods of contraception [25].
1.3. Study Setting
- According to the United Nations (2015), 1.74 billion populations live in South Asia in 2015 which is equivalent to 23.7 percent of the World Population. Among the 1.74 billion population of South Asia, 1.47 billion populations live in Bangladesh and India. These two countries have total fertility rates above the replacement level (i.e., on average 2.1 children per woman) during 2010-2015 (2.23 in Bangladesh, and 2.48 in India) and a large number of younger population (ages 0-14) indicating that the total population of these countries will continue to grow even after achieving the replacement level of fertility due to the momentum effect. United Nations (2015) projection shows that the total population of these two countries will increase to 1.91 billion by 2050 comprising 19.6 percent of the projected world population (9.73 billion). Bangladesh and India introduced family planning programmes in 1950s to control the rapid population growth and ensure economic development. However, the success of the family planning programmes has not been identical across Bangladesh and India [4]. For instance, among currently married women in Bangladesh, the contraceptive prevalence rate was 61.2 percent, use of any modern method of contraception was 52.1 percent, and contraceptive discontinuation rate was 35.7 percent in 2011 [26]. In India, among currently married women the contraceptive prevalence rate was 56.3 percent, rate of using modern method was 48.5 percent, and discontinuation of contraception was 27.2 percent in 2005-06 [27].
2. Data and Methods
- This study draws data from the 2014 Bangladesh Demographic and Health Survey (BDHS) and the 2005-06 National Family Health Survey (NFHS) of India. These are nationwide sample surveys of men and women of reproductive age and contain wide range of information on family formation, fertility preferences, use of family planning methods. In the 2011 BDHS, 17,842 ever married women were interviewed with a response rate of 97.9 percent. In the 2005-06 NFHS of India, 124,385 women were interviewed with a response rate of 94.5 percent. However, for this study only currently married women age 15-49 were selected based on the objectives of examining the prevalence of using contraception (any method), using modern methods of family planning, and discontinuation of contraception. Hence, never married women, divorced, separated and widowed, and currently married women who are infecund were excluded from the analysis. Thus the final sample sizes for the study population were reduced to 16,795 for Bangladesh and 86,789 for India.
2.1. Dependent Variables
- There are three outcome variables of interest in this study: (1) whether currently using any contraception (i.e., using a family planning method at the time of the survey), (2) whether use modern method of contraception and (3) whether discontinued using the last method of contraception (12-month episode). The number of samples for the first outcome variable of interest, whether use contraception (any method), were 16,795 for Bangladesh, and 86,789 for India. For the second outcome variable, whether use modern method, those who did not use contraception were excluded from the analysis. Thus the numbers of respondents included in the analysis of second outcome variable were 10,451 for Bangladesh, and 50,056 for India. The third outcome variable of interest, discontinuation of contraception, includes all women who were using any method of family planning at the time of the survey. Hence, the number of selected respondents for examining the third outcome variable is similar to that of the second outcome variable of interest.
2.2. Independent Variables
- In this study, three demographic variables were included in the analysis: respondents’ age (in years), age at first marriage (in years) and number of living children (0, 1-2, and 3+). Among socioeconomic variables, respondents’ education (no education, primary, secondary and higher), employment status (employed and not employed), wealth index (poorest, poorer, middle, richer, richest), place of residence (rural or urban), whether read newspaper (yes or no) and whether watch television (yes or no), and husband’s education were included in the analysis. Finally, country (Bangladesh and India), and time (year of the survey) were also included in selected multivariate analysis. The outcome variables of interest in this study (whether use contraception, whether use modern, and whether discontinued use of contraception) are dichotomous variables (yes or no). As such, logistic regression estimates were applied to examine contraceptive uses, method choice and contraceptive discontinuation in Bangladesh and India. To take into account the wide geographic heterogeneity in sociodemographic and cultural factors that characterize South Asia, first, separate multivariate analyses were performed for the two countries, and then a separate analysis was conducted by including the two countries together. In the latter analysis, regression models were estimated by including country and time in the analysis along with the covariates mentioned above. Inclusion of country in the analysis would facilitate comparison of use of contraception, use of modern method, and discontinuation of contraception across the two countries of South Asia. Sampling weights were applied in all multivariate analyses. In addition, since the 2014 BDHS and the 2005-06 NFHS of India were conducted in different time points, time variable was included to generate unbiased estimate of the effect of selected predictors on contraception use, method choice and discontinuation of contraception.
2.3. Sample Characteristics
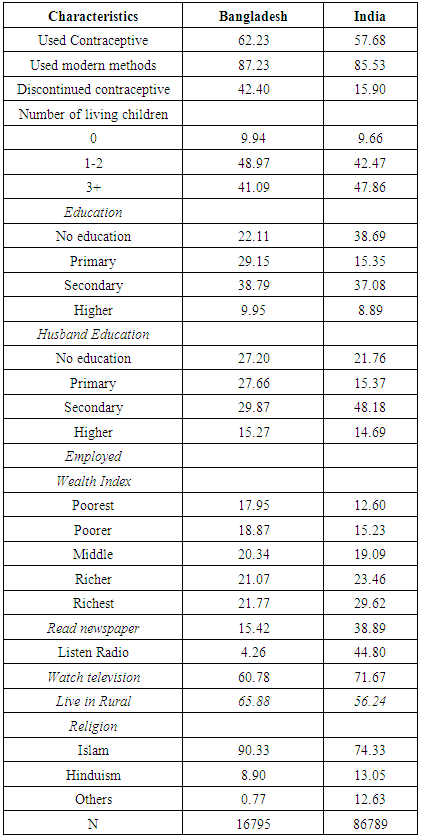
- In Bangladesh, 62.2 percent contraceptive prevalence rate, 87.2 percent use of modern methods and 42.4 percent discontinuation rate in 2014. The average age at first marriage was 15.9 years and 41.1 percent women had more than three children. More than half of the women had less than secondary education and only 30.2 percent women were employed. Exposure to television was much higher among women (60.7%) than exposure to newspaper (15.4%) and radio (4.3%). About third-women in Bangladesh lived in rural areas and more than 90.0 percent of all women were Muslims (Table 1).
|
3. Results
3.1. Bangladesh
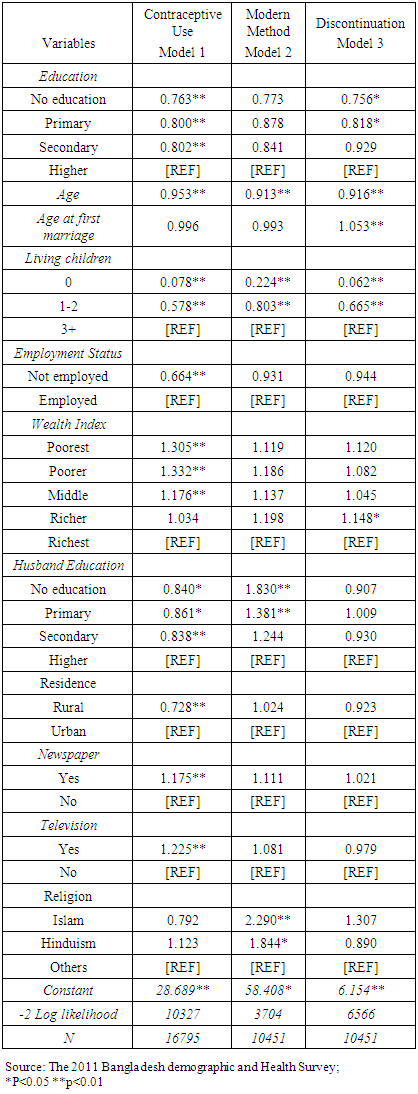
- The multivariate logistic regression estimates of contraception use (any method), use of modern method, and discontinuation of contraception in Bangladesh and India are presented in the form of adjusted odds ratios (AOR) in Tables 2-4. In Bangladesh, lower educated women were less likely to use contraceptive than higher educated women. For instance, women with no education had 34.7 percent lower odds of using contraception than women who had higher than secondary education. Women with no child or 1-2 children were less likely to use contraception than those who had 3+ children [AOR=0.078, 95% CI: 0.07-0.09; and AOR=0.578, 95% CI: 0.53-0.63 respectively]. Women who are not employed or living in rural areas were also less likely to use contraception. However, women with lower wealth index were found to be associated with higher rate of contraceptive use than the richest category. Part of the reason might be that greater awareness has been created among the women in lower wealth index categories by the Government and non-government organizations. Consistent with the expectation, exposure to newspaper and television was found to be associated with higher odds of contraceptive use [AOR=1.175, 95% CI: 1.05-1.31; and AOR=1.225, 95% CI: 1.13-1.33] (Table 2).
|
3.2. India
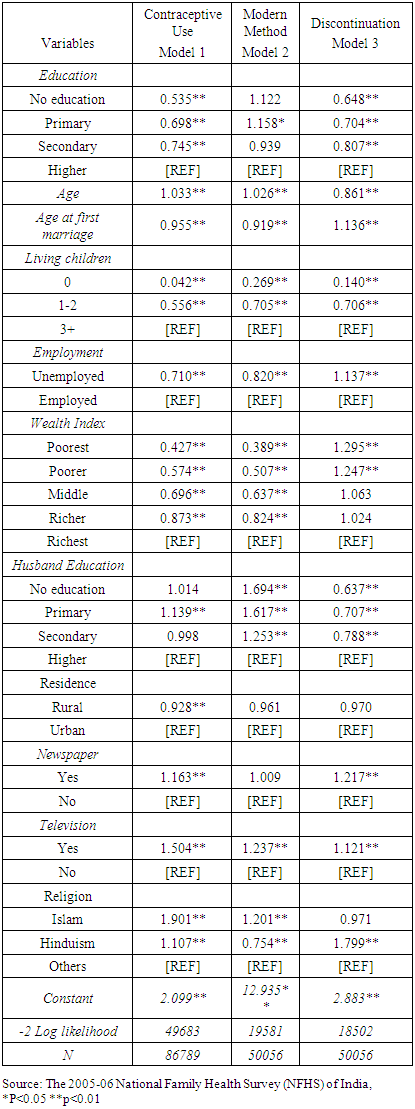
- In consistent with Bangladesh, it was found that lower educated women were less likely to use contraception than higher educated women in India. For instance, women with no education had 46.5 percent lower odds of using contraception than women who had higher than secondary education after controlling for the selected covariates. Higher age at marriage, and having no child or 1-2 children were found to be associated with lower contraceptive use. Not employed women were less likely to use contraception than employed women [AOR=0.710, 95% CI: 0.69-0.73].In contrast to Bangladesh, women with lower wealth index in India were less likely to use contraception than their counterparts with the richest wealth index. Rural women were also less likely to use contraception than urban women [AOR=0.928, 95% CI: 0.89-0.96] in India. However, women who read newspaper/magazine or watched television were more likely to use contraception than their respective counterparts of those who did not read newspaper/magazine or watch television (Table 3). Similar to the findings of Bangladesh, it was found that in India women with primary education were more likely to use modern method compared to women with higher than secondary education [AOR=1.158, 95% CI: 1.01-1.31]. In addition, in India, women having married at older ages or having no child, or not employed were less likely to use modern method than their respective counterparts. Women in the poorer wealth quintiles were found to have lower probability of using modern methods than their counterparts in the richer wealth quintiles after adjusting for the selected covariates. For instance, poorest women had 61.1 percent lower odds of using modern methods than the richest women. However, women who had exposure to television were more likely to use modern method than those who did not have exposure to television in India [AOR=1.237, 95% CI: 1.15-1.33]. Moreover, Muslims had 20.1 percent higher odds of using modern methods and Hindus had 24.6 percent lower odds of using modern methods than the followers of other religion (Table 3).
|
3.3. Variations between Bangladesh and India
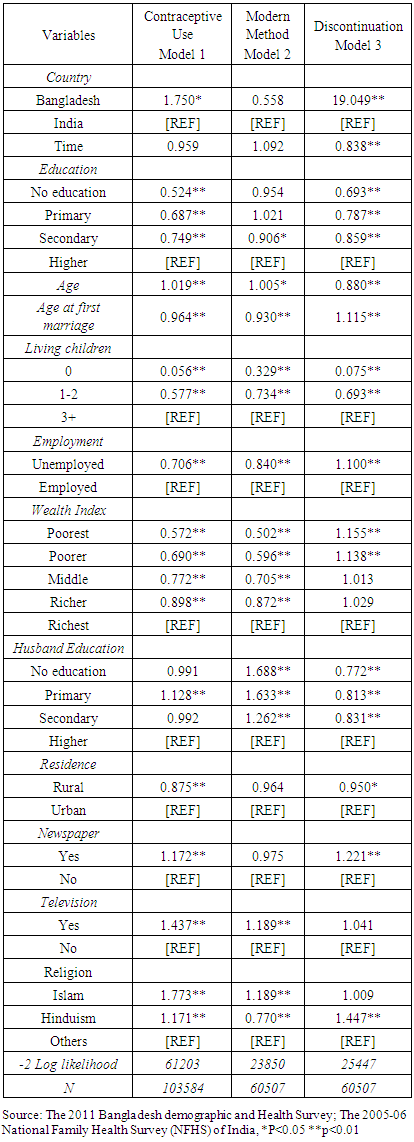
- Table 4 presents logistic regression estimates of contraceptive use (any method), use of modern method and discontinuation of contraception in Bangladesh and India. It was found that women in Bangladesh had 75.0 percent higher odds of contraceptive use than their counterparts in India.[AOR=1.750, 95% CI: 1.08-2.84] after adjusting for age, age at first marriage, education, employment status, wealth index, religion, place of residence, time and exposure to media. However, there was no significant difference in the use of modern methods among women in Bangladesh and India after adjusting for the selected covariates. Nevertheless, women in Bangladesh had much higher discontinuation of contraception than women in India after controlling for the selected covariates [[AOR=19.049, 95% CI: 8.59-42.22] (Table 4).
|
4. Discussion and Conclusions
- Although the use of contraceptives in general and modern methods in particular have increased considerably in Bangladesh and India over time, considering their large number of population further improvement is required to bring desired change in the fertility levels. The main objective of this study was to examine variations in contraception uses and discontinuation across women’s background characteristics, in Bangladesh and India. This study revealed significant variations in contraceptive use (any method) and use of modern methods across women’s education, employment status, wealth index, place of residence and exposure to newspaper/magazine and television in all three countries. Husbands’ lower education was found to be associated with lower contraceptive use (any method) but higher use of modern method in Bangladesh and India. Thus the findings of this study suggest that Governments should focus more on increasing women’s education, employment opportunities and economic status for increasing contraceptive prevalence rates and consequently reducing fertility rates. Further attention should be given in addressing the obstacles for using contraceptives by women. More specifically, various initiatives should be taken to increase contraceptive prevalence rate such as providing third and fourth generation contraceptives to women, addressing side effects adequately, creating awareness to address unmet need for family planning and eliminating social and cultural barriers. The DHS data shows that 34.1 percent women in Bangladesh and 42.6 percent women in India either unsure about using contraception or do not intend to use contraception in future. The reasons for not intending to use contraceptives also include fertility related (wants as many children as possible, up to God/fatalistic), methods related (health concerns, fear of side effects, inconvenient to use, and interfere with body’s normal process), opposition to use (respondents opposed, husband/partner opposed, religious prohibition), and lack of knowledge [26]. There are two principal obstacles to using a contraceptive: (1) woman’s perception that such behavior would conflict with her husband’s fertility preferences and his attitudes toward family planning and (2) her perception of the social or cultural unacceptability of contraception [7]. Consistent with the idea of the “diffusion of innovations”, emphasis should be given on creating awareness through media, advocacy and technology for increasing contraceptive prevalence rates in Bangladesh and India for increasing contraceptive prevalence rates [7]. The better effectiveness of modern methods over traditional methods of family planning in averting unwanted pregnancies is well established in the literature [28-30]. Among the users of modern contraceptives in Bangladesh, pill was the most widely used method, followed by injectables, male condoms, and female sterilization [26]. In India, female sterilization is the most common followed by condom and pill [27]. In Bangladesh, indicators of contraceptive evaluation (side effect and convenience of current modern method), contraceptive access (accessibility/availability of current modern method and cost of current modern method) and programmatic factors (visit of family planning workers/FWAs) significantly increased the likelihood of using modern methods of contraception [31]. In developing countries women faced many obstacles including lack of access to information and health care services, opposition from their husbands and communities, misperceptions about side effects, and cost [32]. Addressing these problems will increase the rate of using modern methods substantially. Concerning the discontinuation of contraception it was found that there were significant variations in contraceptive discontinuation across women’s background characteristics in Bangladesh and India with few exceptions. In Bangladesh, the most common reason for contraceptive discontinuation was side effect/health concerns followed by desire to become pregnant, other fertility related reasons, method failure, other method related reasons including lack of access/too far, costs too much, and inconvenient to use [26]. These reasons for discontinuation of contraception are also evident in India [27]. In addition, the discontinuation of contraception can also emerge from other sources such as lack of interpersonal communication and courtesy by providers. In Bangladesh, there remains a non-communicative, hierarchical attitude between clients and paramedics which contributed to poor understanding of potential side effects and incorrect method use. Hence they argued that by providing adequate counselling, supporting women to sustain use of more effective contraceptive methods, and helping to manage side effects and switching methods when they do have a problem would decrease the discontinuation of contraception to a large extent [32]. This study revealed significant variations in the use of modern method across women’s background characteristics in Bangladesh and India. Conducting separate analysis for the determinants of each of the modern methods (e.g., pill, injectables, condoms, female sterilizations, male sterilization, IUD, implants) provide better understanding about the dynamics of modern method selection which will also facilitate generating effective policy recommendations. Similarly, there are variations in discontinuation of different methods of contraception in each of these countries. The factors associated with the discontinuation of each method are also different in many respects. Therefore, analyzing trends and determinants of discontinuation for each methods separately would provide better insight about the dynamics of contraceptive discontinuation in Bangladesh and India. Finally, conducting decomposition analysis would better illuminate the relative contribution of each of the sociodemographic, economic, and cultural factors to the differentials in contraceptive use (any method), use of modern method and discontinuation of contraceptive in Bangladesh and India.