-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Sociological Research
p-ISSN: 2166-5443 e-ISSN: 2166-5451
2013; 3(3): 67-72
doi:10.5923/j.sociology.20130303.03
Anxiety among Chinese Older People Dwelling in Traditional Family versus Nursing Home: A Meta-analysis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLFeng Tong1, Hongbo Li2, Chenggang Yang1
1Southwestern University of Finance and Economics, Chengdu, 610074, China
2Nankai University, Tianjin, 300192, China
Correspondence to: Feng Tong, Southwestern University of Finance and Economics, Chengdu, 610074, China.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Background: In the aging china, there are two main supporting models for elderly, traditional family support, nursing home support. Objective: to investigate the influence of anxiety statue in different resident places by combining the existing demographic variables researches. Methods: totally 11 literatures selected in the Meta-analysis, demography background and health-related conditions data was extracted. Anxiety was measured with SAS and STAI-Y respectively. Results: for the whole sample, there is no significant difference on the level of Anxiety between the two groups. But the older age individuals reported higher level of anxiety in traditional family rather than in nursing home. Furthermore, different demographic characteristic reported different anxiety levels within age, gender, educational experience, marital situation and so on. Conclusion: to benefit elderly mental health, higher age windowed individuals might be more suitable to live in nursing home, and there are some suggestions for elders living in traditional family.
Keywords: Anxiety, Meta-analysis, Traditional Family Support, Nursing Home Support
Cite this paper: Feng Tong, Hongbo Li, Chenggang Yang, Anxiety among Chinese Older People Dwelling in Traditional Family versus Nursing Home: A Meta-analysis, American Journal of Sociological Research, Vol. 3 No. 3, 2013, pp. 67-72. doi: 10.5923/j.sociology.20130303.03.
Article Outline
1. Introduction
- A study in late 2012 found that there were 178 million people over 60 years-old in China, taking up 13.26% of the total population[1]. Some authors estimated that this proportion would increase to 20% by 2025 and 25% by 2050[2]. Thus, China is a rapidly aging country both in terms of the over all proportion of elderly in the population and in terms of the rate of increase in the proportion of elderly. At the same time the one-child-policy has led to a rapid decrease in the size of urban families, so the traditional method of supporting the elderly is not the only way can solve. More and more institution supporting was accepted. But so far most the Chinese elderly willing to choose living on a traditional family support in the their own home or in their son’s and daughter’s home rather than nursing home or institution, because nursing home or institution are considered to be a poor condition living, less support and may lead more mental problems. In this view, elderly have psychological resistance to enter the nursing home.Anxiety disorders in later life are very highly prevalent[3,4,5]. Prevalence estimates in later life range from 1.2% to 14.2%[6,7] depending on sampling procedure, age cut-offs for classification as old and exclusion of anxiety cases due to general medical conditions. A Chinese research reported Chinese elderly thought that the nursing home can not meet their psychological needs[8], and may lead to even worse mental health and fewer positive emotions and so on. Some studies based on western data also found that the elders in institutions have higher incidence of depression and anxiety disorders than which in the community and traditional family[9, 10, 11]. There is a new research reports that the elders in Nursing home presented 28.1% depression prevalence rate, 27% anxiety disorders, much higher than the elders in community and traditional family[12, 13].In the late life, the medical disease is very frequent and several physical conditions such as respiratory, cardiac and vestibular problems may both be a source of anxiety and be exacerbated by anxiety[7]. And many previous studies reported various factors would affect the elderly mental health status, such as age[14, 15], gender[16], health[17], marriage status[16, 8, 18], economic status[16, 19], anxiety symptoms, chronic illness. functional limitations[20,21,22] as well as the social support models[19]. And of course there are many obvious significant differences between traditional family support and the nursing home support for elders in many aspects, which could lead to different elderly mental health status. The elderly average age is generally higher which in the nursing home than in home[23] and the prevalence of various diseases is also worse than living traditional family support[24, 10], but it may cause by the age of elder rather than the hygienic conditions of living. However in a direct contrast research between the traditional family support and the nursing home support, reported that the difference was not significant[15]. And many researches about elderly anxiety symptom in different demography background reported very different consequences. Some factors result in vulnerability to disease and increased medication use[25, 26]. So to properly appraisal the mental health status, the demography factors should be considered inevitably.In this study we review current relevant research and integrate the outcomes to evaluate the relationship between demography variable and mental health status in different social support, as well as appraisal the existing research by systematic review as well as quantity Meta-analysis, in order to reduce the research bias, and find out general reason of diverse mental health status between traditional family support and the nursing home support, help decision makers.
2. Methodology
- The first use of the concept of "meta-analysis" is an American scholar named Glass. His definition of meta-analysis is: to integrated discovery the already researches by comprehensive statistical analysis on the results of every single study[27]. Thus meta-analysis is a scientific, standardized and efficient secondary research methods, which can be largely overcome the limitations of traditional literature review exists. In this paper the meta-analysis method is trying to apply in this research to analyze the anxiety intervention research, planning to use a descriptive analysis on existing researches and study, as well as quantity integrate those researches and study which match the Meta-analysis condition, in order to provide useful evidence for the elderly anxiety and psychological intervention by different support models. Meta-analysis is a way of merging the results of multiple independent studies into a single effect size (effect size, ES), which uses a combined statistic reflects the combined effect of multiple independent studies. Meta-analysis do not based on the original information, but by the existing statistical research results. There are two types of such results, one is test of hypothesis research, such as the t, ,2,P , etc.; Another one is the statistical values in each report, including the measurement data (continuous variables) and count data (discrete categorical variables) The indicators of count data include: odds ratio(OR)、relative risk(RR)、risk difference( RD)、hazard ratio(HR),etc. The indicators of measurement data include: correlation coefficient (r)、mean difference、weighted mean difference(WMD)、standardized mean difference(SMD),etc. The values used in this study is the weighted mean difference (WMD), Mark as‘d’.
3. Search Strategy
- In the research of elderly mental health, we have to control the research background for reducing the research bias, so the literatures we chose are based on a same criterion: same age, gender, education level, marital status and other factors. Because the elderly in nursing home always have higher age and higher widowed rate, and those two key risk factors effecting elderly mental health[28], may create bias to the research of the supporting models on the elderly mental health.Studies were identified by searching the Cochrane Central Register of Controlled Trials (CENTRAL), Porquest, CNKI and WanFang databases from 1970 to 2013. We used a search string involving the MeSH term for anxiety disorders and combinations of ‘elderly anxiety disorder ’and ‘Traditional Family support’ or ‘Nursing home’ or ‘family support’ or ‘community support ’ or ‘long term care’ or ‘dwelling support’ and the MeSH term for ‘support’ and combination of terms (‘care’ or ‘support’ or ‘interruption’ or ‘behaviors therapy’ or ‘feedback’ or ‘intervention’ or ‘counselling’) to maximize identification of relevant studies. Additional papers were identified from reference lists. We did not use studies in press or unpublished studies in this research. For this meta-analysis we included (a) published randomized controlled trial (RCTs);(b)case-controlled studies;(c) quasi-experimental studies (d)descriptive studies (e)single case experimental (f) experts opinion. Search criteria as following were tailored according to the database. Citation tracking was used to identify additional studies from the reference lists of previous relevant systematic reviews.
4. The Meta-analysis of Anxiety
- Consistent with the aim of reviewing the effectiveness of support, comparative, experimental studies were selected. There are two highest frequency used scales in anxiety study: Zung's self-rating anxiety scale (SAS) and the State-Trait Anxiety Inventory (the STAI-Y). SAS contains 20 items reflect the subjective feelings of anxiety, each item is divided into four rated in accordance with the frequency of symptoms, the Standard cut-off value is 50 points, 50-59 of which are divided into mild anxiety, 60-69 moderate anxiety, severe anxiety more than 69 points. STAI-Y has state anxiety and trait anxiety subscales, each of them has 20 questions, the former described a short-term unpleasant emotional experience, such as stress, fear, anxiety, often accompanied by autonomic nervous system hyperthyroidism; latter is used to describe a relatively stable in mood, as a personality characteristic and tendency of individual differences in anxiety. Each topic scoring by four points, and the minimum of each subscale is 20 points, the highest score is 80 points. As different health contexts, the experimental designs are often not possible or feasible, so study eligibility for inclusion in the review was assessed by two reviewers (Li and yang), with disagreements being resolved by consensus. And studies were categorised as having a theoretical basis if they cited a specific theory underlying their intervention design, or reported that the intervention was based on a broad theoretical approach. The Meta-analysis result of existing researches basing on those two questionnaires in three aspects as follows.
4.1. The Rate of Elderly Anxiety under Differences Support Models
- There are 11 relevant literatures of the SAS Scale measurement results of traditional family support elders, referring to 3163 people, and 887 people’s the standard points are over 50, calculating the elderly anxiety overall detection rate was 28.04%. there are five relevant literatures of the SAS Scale measurement results of nursing home elderly, referring to 2321 people, and 483 people’s the standard points are over 50, calculating the elderly anxiety overall detection rate was 29.87%. The whole percentage of anxiety disorder rates are very high among Chinese elderly, actually in the same level in those two supporting models, but a little better in traditional family elders. The better outcomes in the traditional family support group compared to those in the nursing home group might be due to the stronger social support network by family members. However, more prospective studies would be done as following to confirm that the results are not only due to circumstances bias and reveal more correlation factors between those two models.
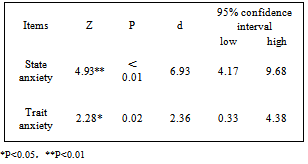
4.2. The Distinction of Elderly Anxiety under Differences Support Models
- Because those SAS outcome measurements were not sufficient as literatures limitation, so the outcome of the STAI-Y measurement is adopted to measure elderly anxiety. Literature inclusion criteria: ① STAI-Y Scale as a measurement tool; ② the state and trait anxiety under different support models were to be measured; ③ the report provides each number of different support group, and the mean score and standard deviation. A total of 6 studies matched the inclusion criteria, referring to 2356 people. We set the nursing home support as "Treatment", setting the traditional family support as "control". Firstly we tested the homogeneity of the input data, when P over than 0.05 using a fixed effects model, when P less than 0.05 using a random effects model (the same way for the following data). And test of homogeneity of the two sets of data reports P less than 0.05, which means the study is heterogeneity, suggesting using the random effects model.
|
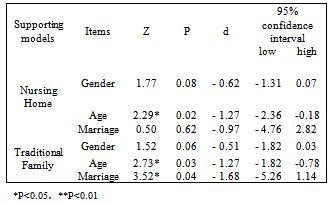
4.3. The Correlation between Demographic Variables and Anxiety Levels in Different Support Models
- The presence or absence of significant correlation between demographic variables and anxiety levels cause many researchers’ attentions, with many arguments. We select three most frequently used variables: gender (male, female), age (<75, >75) and marriage (married, single), analyze the STAI-Y results. Literature inclusion criteria (gender as an example): ① STAI-Y Scale as a measurement tool; ② state anxiety of men and female were to be measured; ③ The report provides the number of men and female groups, as well as the mean and standard deviation of the score. There are five literatures matched the standards of gender comparison, and two each of age and marriage. The Meta-analysis results of state anxiety and trait anxiety score are shown in Table 2 and Table
|
5. Limitation
- This study has several limitations. To the first, although this meta-analysis included a relatively large number of studies, we did not have sufficient analysis to examine more specific subgroups, such as studies with windowed groups in which subjects were recruited from very different circumstance. For the second, the quality of several studies was not optimal, and for some influence factors we only conducted describe analysis instead of intention to impact analyses. Thirdly, the correlation factors in this study considered and controlled is limited, In addition to elderly age, sex, marital status, social interaction, social support and so on[11,14], may also affect elderly mental health to some extent. Thus the conclusion of this study has some limitations in application and promotion process, look forward to a deeper and more comprehensive study to test this conclusion. Despite these limitations, the present meta-analysis illustrates the influence and relationships between nursing home support and traditional family support, analyze both advantages and disadvantages by demographic characteristics in those two group, and proposal that some multi-supporting model to remain stable to follow-up and may even improve somewhat.
6. Conclusions and Suggestion
- By comprehensive analysis in above study, some suggestions could be discussed in final part, as the traditional family support model is the most common supporting so far in China, the suggestion mainly focus on improving this model by adapting more community supports, in order to develop a range of services to meet the different types of elderly needs; however, the nursing home support model, the research reports it is not so worse as people’s thinking and maybe suitable for some elderly population, such as widowed. According to advantages both in traditional family support and nursing home support, there are six target criteria may application for better mental health and providing high-quality life for the elder: 1) provide financial support for all elderly who have on or less resource of support in order to make them can choose dwelling what they want. 2) provide home meals services, mental care, day care centers, community cultural activity centers, and similar institutions that promoting elderly essential social communication. 3) provide diverse cultural and recreational collective activities to promote elderly social participation, especially for widowed elderly. 4) provide local health services to establish a medical record for all elderly citizens and provide regular follow-up of chronic conditions 5) create retired administrative network form an aging services for the elder with dedicated full time staff 6) establish a legal consultation service for the elderly which is free of charge for those who can not afford the service in each local community or in nursing home.Although large number of studies about supporting models refer to elderly anxiety disorder is relatively high, more research and clinical samples is definitely needed. Preferably, these should be high-quality studies with large sample sizes. Our data suggests that providing more service options by demographic characteristic for the elderly which can improve their support networks and decrease some of their psychological symptoms, but much more work is needed refine these methods, to test their efficient, and to determine how best to adapt effective models to other communities, particularly rural communities. Most importantly, the extent to which social supporting models can actually improve social support, psychological health and the quality of life in elderly individuals will remain uncertain until more and more long-term prospective studies in relatively large samples are conducted.