-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Sociological Research
p-ISSN: 2166-5443 e-ISSN: 2166-5451
2013; 3(2): 30-35
doi:10.5923/j.sociology.20130302.03
Factors Associated with Adolescent Pregnancy and Fertility in Uganda: Analysis of the 2011 Demographic and Health Survey Data
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRutaremwa Gideon
Center for Population and Applied Statistics, Makerere University, Uganda
Correspondence to: Rutaremwa Gideon, Center for Population and Applied Statistics, Makerere University, Uganda.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Adolescent pregnancy and fertility are often discussed in literature as causes of health concern and as a social problem. Taking these accounts as a starting point, this paper uses the 2011 Uganda Demographic and Health Survey Data explore the factors related to adolescent fertility and pregnancy in Uganda. A total of 2,026 female adolescents are selected for this study. Logistic regression analyses adjusted for socioeconomic and demographic characteristics are estimated to predict the odds of an adolescent having borne a child in the 5 years preceding the survey, being currently pregnant and both having had a child in the 5 years preceding the survey or being currently pregnant at the time of the survey. Marital status is a strong predictor of the likelihood of both having a child in the 5 years preceding the survey and being currently pregnant at the time of the survey. Age equally appears to be an important predictor of the two outcomes, such that an increase in age was associated with increase in the odds of being pregnant and of having born a child. The discourse in this paper shows that adolescent pregnancy and childbearing is a serious policy intervention area that requires redress.
Keywords: Adolescent Pregnancy, Fertility, Uganda, Demographic, Health Survey
Cite this paper: Rutaremwa Gideon, Factors Associated with Adolescent Pregnancy and Fertility in Uganda: Analysis of the 2011 Demographic and Health Survey Data, American Journal of Sociological Research, Vol. 3 No. 2, 2013, pp. 30-35. doi: 10.5923/j.sociology.20130302.03.
Article Outline
1. Introduction
- There is growing evidence that associations between teenage motherhood and poor health outcomes can be explained by young mothers’ long-term socioeconomic disadvantage[1]. In spite of the recognition that teenage motherhood is a complex issue reflecting individual, familial and structural forces, the focus in medical related journals on health disparities due to maternal age makes teenage mothers visible as a certain class of person. Current constructions position teenage pregnancy as a sign of individual failure and deviance[2;3;4] and scientific interest in teenage mothers is justified on grounds of poor health and economic disadvantage[5]. The recent shift from representing teenage motherhood as a moral problem to being a psychological or health problem both reflects and further legitimizes early pregnancy as an issue for science [6;7].Teenage pregnancy and motherhood has remained a major health and social concern in Uganda because of its association with higher morbidity and mortality for both the mother and child. In addition to the physiological risks, there is a negative effect on the socioeconomic status of the mother, and hence the child, because current school policy is to have pregnant girls terminate their education.With 24 percent of adolescent girls becoming pregnant before the age of 19, Uganda has one of the highest rates of adolescent pregnancy in Sub- Saharan Africa[8] . The country’s high adolescent pregnancy rate has two distinct implications. First, the risk of maternal death is higher in adolescents than in older women. In addition, pregnant adolescent girls are more susceptible to pregnancy- and childbirth-related complications because they have not yet developed the physical maturity required for a healthy pregnancy. Other common medical problems associated with adolescent pregnancy include obstructed labour, eclampsia, fistula, low birth weight, stillbirths, and neonatal death.In Uganda evidence suggests that the proportion of teenagers who have started childbearing has declined over time, from 43 percent in the 1995 UDHS, to 31 percent in the UDHS 2000-01, to 25 percent in the 2006 UDHS, and finally, to 24 percent in 2011. As expected, the percentages of women who have started their reproductive life increases with age because of longer exposure, from 2 percent of women age 15 to 58 percent of women age 19. Furthermore, the socio-economic impacts of adolescent motherhood are devastating.Adolescent girls who become pregnant are often unable to complete a secondary education, a fact that diminishes their potential to find employment [9]. Education and economic status are factors that influence adolescent pregnancy. Adolescents who have completed secondary school tend to have low pregnancy rates (15%) compared to adolescents who have no secondary education (50 %). From an economic perspective, adolescents from poor households are more likely to become pregnant compared to adolescents from wealthier families. For the former, the pregnancy rate is 41 percent and for the latter the rate is 16 percent [10].
2. The Context of Adolescent Pregnancy and Fertility in Uganda
- Uganda’s National Adolescent Health Policy defines adolescents as people between the ages of 10 and 19 years. Twenty-five percent of Uganda’s population is comprised of adolescents. A 25 percent pregnancy rate among adolescents in a population of 30 million people is therefore a worrying issue for the government of Uganda[10]. The Uganda government has enacted policies to address adolescent pregnancy. These policies set definite targets and are aimed at protecting young girls from unplanned pregnancies. Traditionally, social, economic and cultural norms in Uganda encourage marriage and childbearing at an early age. As such, female adolescents in Uganda face cultural and social pressure from their families to marry young and begin child-bearing early [11]. However, adolescent pregnancy outside wedlock is frowned upon in Uganda. The social stigma associated with pregnancy outside wedlock is further compounded when adolescents are forced to terminate their studies and families feel compelled to send their pregnant daughters away[12]. The social stigma and the resultant stress often compromise the health and well-being of pregnant adolescent girls and their unborn babies. Stigma, coupled with lack of support from families and society at large, compels some unmarried pregnant adolescents to seek abortions [9].Statistics show that about 15 to 23 percent of female youths aged between 15 and 24 have had an abortion [13]. This is an issue of concern because abortion, which is illegal in Uganda, is performed by untrained midwives in unsafe conditions, greatly increasing the risk of disability and death for pregnant adolescents. Figures indicate that 13 percent of maternal deaths and 27.8 percent of deaths among adolescents in Uganda are primarily due to unsafe abortions[13].There are various policies designed to delay and protect young women from becoming pregnant during adolescence. These policies include the National Health Policy, the National Adolescent Health Policy, the National Policy on Young People and HIV/AIDS, the Sexual Reproductive Health Minimum Package, the Minimum Age of Sexual Consent Policy (set at 18 years of age), the defilement law and a Universal Primary Education – (UPE) policy[14]. These policies also serve the purpose of fostering a supportive environment to encourage adolescent reproductive health. Notable among these policies is the National Adolescent Health Policy, introduced in 2004 to address the specific needs of adolescents, including pregnant girls. The policy’s objective is to streamline adolescent health needs to national health and development policies. Additionally, Uganda released the National Policy Guidelines and Service Standards for Reproductive Health Services in order to provide direction for reproductive health service provision and set national rules and regulations [15].The guideline calls for increased access to contraception, adolescent-friendly services and post-abortion services, as well as support for unwanted pregnancies and services for single adolescent mothers. The Uganda government has also enacted laws to protect adolescent girls from pregnancy and sexual coercion. The minimum age of sexual consent was raised from 14 to 18 in the 1990s to help curb the spread of HIV/ AIDS [16]. Further, a law governing defilement makes it a criminal offence to impregnate a girl under the age of 18[12].One of the major shortcomings of Uganda’s health policies is the lack of full and proper implementation. This is mainly because of funding shortfalls that confound support for dissemination and implementation of these policies across the country [17;18]. For example, although maternal and child health is identified as a priority by the government, huge funding gaps prevent the health sector from achieving the goals outlined in the National Health Policy[18]. Health care centers in the country are underfunded, understaffed and overcrowded, which means adolescent-friendly services are few and far between.Furthermore, various stakeholders lack knowledge about the country’s health policies and awareness of individual roles and responsibilities in implementing these policies[17]. For instance, the National Adolescent Health Policy states that pregnant adolescent girls should be readmitted to school after they have delivered, but Uganda’s Education Policy is silent on this issue [19; 14]. As a result, researchers have noted that the school systems tend not to offer social support to pregnant girls, but rather send them away [12]. Terminating studies at adolescent age due to pregnancy and motherhood places these young persons in a precarious socio-economic situation given that it limits their future employment prospects. It is against this background that this study seeks to examine factors associated with adolescent pregnancy and fertility in Uganda.
3. Data and Methods
- In this analysis, we use data from the Uganda Demographic and Health Survey[8]. This data allows us to select individual females in the adolescent ages 15-19 years, and overall a total of 2,026 females were selected for this study. The survey traditionally collects information on socioeconomic characteristics of individual women in the reproductive ages; in addition information is available in the data set concerning various reproductive health issues including pregnancy and child birth. For this reason, the UDHS 2011 data for Uganda provides an opportunity to study adolescent pregnancy and fertility in the country. We use descriptive analysis, first, to compare the characteristics of adolescents across the different socioeconomic factors including: region, residence, marital status, wealth index, educational level attainment age, religion and ever use of family planning. At the second level of analysis, three logistic regression models are estimated predicting three outcomes: 1). whether the individual adolescent is currently pregnant; 2). whether the individual bore a child within the five years preceding the survey; and 3). whether the individual was either pregnant or had borne a child in the 5 years preceding the survey. In all the three models control variables were added to account for either mediation or confounding effects of these variables. Formally, these equations may be expressed as follows:
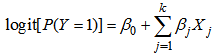 Where logit[P(Y=1)] refers to the natural log odds that a respondent will: be pregnant (Model I), borne a child in the 5 years preceding the survey (Model II), or be pregnant or had borne a child in the 5 years preceding the survey (Model III); β0 refers to the intercept of the regression model; and βjXj refer to regression estimates for the set of explanatory variables (numbered 1 through k) included in each of these models.
Where logit[P(Y=1)] refers to the natural log odds that a respondent will: be pregnant (Model I), borne a child in the 5 years preceding the survey (Model II), or be pregnant or had borne a child in the 5 years preceding the survey (Model III); β0 refers to the intercept of the regression model; and βjXj refer to regression estimates for the set of explanatory variables (numbered 1 through k) included in each of these models.4. Results and Discussion
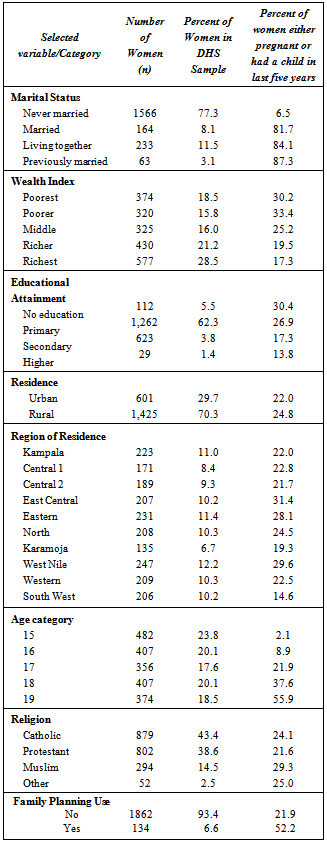
- The descriptive findings presented in Table 1 closely resemble those reported elsewhere, notably, the results show that the majority of the female adolescents (77%) were not yet married and that in this group as high as 6.5% were either currently pregnant or had already born a child. Among the female adolescent who were married, those living with their partner and the previously married, over 80 percent were either currently pregnant or had borne a child already. Similarly, the percentage of female adolescents who were either pregnant or had born a child was highest (30.4% among the poorest and 34.4 among the poorer female adolescent, respectively) among those in the poor and poorest categories. As expected the least proportions pregnant and those who had borne a child was among the richest category of female adolescents (17.3%).Furthermore, female adolescents with no education had the largest proportion either currently pregnant or having borne a child (30.4%), while those with post secondary education had only 13.8% percent of this category currently pregnant or having borne a child. Concerning rural/urban residential characteristics, the findings in Table 1 were as expected, with rural residence associated with a larger proportion (24.8%) either currently pregnant or having born a child, compared to 22 percent among those in urban areas.
|
5. Conclusions
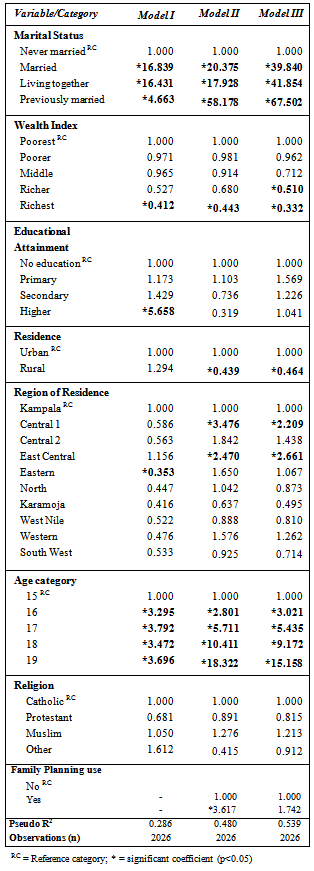
- Given that this study was an initial attempt to explore the factors that are associated with adolescent pregnancy and child bearing in Uganda;it may be difficult to suggest policy recommendations at this point. However, a few conclusions and policy recommendations can be harnessed from this study. First of all, marital status variable appears to be the single most important factor determining pregnancy and child bearing among the adolescent age category. Even education which often provides positive effects on delaying pregnancy and child bearing does not appear to provide significant positive outcomes. This suggests that targeted programmes aimed at sensitizing communities, households and adolescents themselves on behaviour change leading to delayed entry into marital unions could help reduce fertility and the negative outcomes of adolescent pregnancy and child bearing. Second, the analyses suggest that adolescents who cohabit (living together) had significant likelihood of being pregnant and having borne a child. Social policies designed specifically to mitigate this practice among adolescents could prove effective in reducing pregnancy and child bearing rates in Uganda. Third, the regional differences observed in Central and East Central suggest that targeted interventions for behavioral change should prioritize those areas where pregnancy and child bearing are significantly higher, notably the areas in Central region and East Central regions of Uganda. The factors associated with adolescent pregnancy and childbearing in Uganda are intriguing and important for both health, economic and social concerns. It is hoped that improved understanding of the factors associated with adolescent pregnancy and child bearing will lead to improved social policies, ultimately reducing adolescent pregnancy and childbearing in Uganda and elsewhere.Further research is necessary that infers on norms and behaviors of adolescents as they relate to pregnancy and childbearing across subgroups in Uganda. The strength of socioeconomic explanations for subgroup differences, and the link between norms and behavior should be adequately studied. Further studies should also measure the perceptions of negative social sanctions for pregnant adolescents, which relate to the presence or absence of norms against adolescent pregnancy. The improved understanding of these associations will lead to improved social policies, ultimately reducing adolescent pregnancy and childbearing in Uganda.
References
| [1] | L. B. Smith, “Reframing the risks and losses of teen mothering,” American Journal of Maternal Child Nursing, vol. 34, 2009. |
| [2] | M. Breheny and C. Stephens, “Youth or disadvantage? The construction of teenage mothers in medical journals.,” Culture, Health & Sexuality, vol. 12, no. 3, pp. 307–322, 2010. |
| [3] | J. Cherrington and M. Breheny, “Politicising dominant discursive constructions about teenage pregnancy: Re-locating the subject as social.,” Health: An Interdisciplinary Journal for the Social Study of Health, Illness and Medicine, vol. 9, pp. 89–111, 2005. |
| [4] | K. Luker, Dubious conceptions: The politics of teenage pregnancy. Cambridge, MA: Harvad University Press, 1996. |
| [5] | A. Wilson, H. and Huntington, “The construction of teenage motherhood in contemporary discourse,” Journal of Social Policy, vol. 35, pp. 59–76, 2005. |
| [6] | L. Gordon, “Teenage pregnancy and out-of-wedlock births: Morals, moralism, experts,” in Morality and Health, P. Brandt, A.M. and Rozin, Ed. New York: Routledge, 1997, pp. 251–70. |
| [7] | J. Wong, “The ‘making’ of teenage pregnancy,” International Studies in the Philosophy of Science, vol. 11, pp. 273–288, 1997. |
| [8] | UBOS and ICF International Inc, “Uganda Demographic and Health Survey 2011,” Kampala, Uganda, 2012. |
| [9] | A. Wallace, “Adolescent Pregnancy and Policy Responses in Uganda,” Backgrounder, vol. 14, 2011. |
| [10] | UBOS and Macro International Inc., “Uganda Demographic and Health Survey 2006,” Kampala, Uganda, 2007. |
| [11] | S. R. Sekiwunga, R. and Whyte, “Poor Parenting: Teenager’s Views on Adolescent Pregnancies in Eastern Uganda.,” African Journal of Reproductive Health, vol. 13, no. 4, 2009. |
| [12] | L. Atuyambe, F. Mirembe, A. Johansson, E. K. Kirumira, and E. and Faxelid, “Experiences of pregnant adolescents - voices from Wakiso district, Uganda,” African Health Sciences, vol. 5, no. 4, pp. 304–309, 2005. |
| [13] | F. Ssengooba, S. Neema, A. Mbonye, O. Sentubwe, and V. Onama, “Maternal Health Review Uganda. HSD Working Paper 04/03,” Kampala, Uganda, 2004. |
| [14] | L. Darabi, A. Bankole, K. Serumaga, S. Neema, R. Kibombo, H. Ahmed, and P. Banoba, “Protecting theNext Generation in Uganda: New Evidence on Adolescent Sexual and Reproductive HealthNeeds,” New York, 2008. |
| [15] | Republic of Uganda Ministry of Health, “The National Policy Guidelines and Service Standards for Reproductive Health Services,” Kampala, Uganda, 2001. |
| [16] | S. C. MacKian, “What the Papers Say: Reading Therapeutic Landscapes of Women’s Health and Empowerment in Uganda,” Health and Place, vol. 14, no. 1, pp. 106–115, 2008. |
| [17] | S. Neema, N. Musisi, and R. Kibombo, “Adolescent Sexual and Reproductive Health in Uganda: A Synthesis of Research Evidence. Occasional Report No. 14,” New York, 2004. |
| [18] | Republic of Uganda Ministry of Health, “Health Sector Strategic Plan III 2010/11-2014/15,” Kampala, Uganda, 2010. |
| [19] | Republic of Uganda Ministry of Health, “National Adolescent Health Policy for Uganda,” Kampala, Uganda, 2004. |
| [20] | J. Walker, “Early marriage in Africa--trends, harmful effects and interventions,” African Journal of Reproductive Health, vol. 16, no. 2, pp. 231–240, 2012. |
| [21] | R. Jensen and R. Thornton, “Early Female Marriage in the Developing World.,” Gender and Development, vol. 11, no. 2, pp. 9–19, 2003. |