-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Science and Technology
p-ISSN: 2163-2669 e-ISSN: 2163-2677
2013; 3(3): 74-84
doi:10.5923/j.scit.20130303.02
A Study on Infant and Under-five Mortality in Bangladesh: Life Table Approach
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRafiqul Islam, Mahfuzar Rahman, Obaidur Rahman
Department of Population Science and Human Resource Development, University of Rajshahi, Rajshahi, 6205, Bangladesh
Correspondence to: Rafiqul Islam, Department of Population Science and Human Resource Development, University of Rajshahi, Rajshahi, 6205, Bangladesh.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
The purpose of this study is to identify the level of infant and under-five mortality in Bangladesh employing abridged life table technique utilized data from Bangladesh Demographic and Health Survey-2004. The results of life table indicate that the survival function decreases smoothly throughout the period both the rural and urban areas of Bangladesh and these changes are little after the neonatal period. The nqx function is higher for not working mothers than that of working mothers excepting the age 48-59 months. Life expectancy at each age are higher for literate mother, working mother and urban area than that of illiterate mother, not working mother and rural area respectively. It is observed that the ASDRs are high for the overall country level and it is low in urban areas than the rural areas. The ASDRs are also seen to be lower among urban male child than the rural male child. These rates are higher among illiterate and not working mothers than the literate and working mothers correspondingly. Furthermore, it is found that estimated under-five mortality is higher for not working mothers, rural areas, illiterate mothers and male child than that of working mothers, urban areas, literate mothers and female child respectively.
Keywords: Infant, Child and Under-Five Mortality, Life Table Technique, Bangladesh Demographic and Health Survey, Bangladesh
Cite this paper: Rafiqul Islam, Mahfuzar Rahman, Obaidur Rahman, A Study on Infant and Under-five Mortality in Bangladesh: Life Table Approach, Science and Technology, Vol. 3 No. 3, 2013, pp. 74-84. doi: 10.5923/j.scit.20130303.02.
Article Outline
1. Introduction
- Infant and under-five children are the most important demographic phenomena of a population and their growth and development has strong reflection on the future of a country[1]. The mortality of infant and child is a reflection of the care, health and nutritional status of infant and children as well as nation’s health and also indicates the socio-cultural and economic progress in the country. Because of their association with a variety of factors such as maternal health, quality of medical care, socio-economic conditions and public health practices, under-five mortality is an important measure of a nation’s health as well as important for monitoring progress towards the United Nations Millennium Development Goal-4 (MDG-4) to abate child mortality by two-thirds by the year 2015. These rates especially infant mortality rate (IMR) in developed countries showed a rapid decline during the last 50 years, while it is still a problem in developing nations like Bangladesh. In every day, 16652 infant deaths occur in the world of which 211 in more developed and 16441 in less developed countries, for instance, IMR is 44, 5 and 76 per 1000 live births in world, more developed and least developed countries respectively[2]. It was reported that an estimated 29000 children die in every day before the age of five in the world[3]. In 2007, 9.2 million children born alive across the world died before their fifth birth day[4]. But after one year, there were 8.8 million children died before reaching the age of five in the world, of which, 41% of deaths occurred in neonates[5,6]. In spite of decreasing childhood mortality, it still remains high in some vulnerable groups and areas. The child mortality in the poorest households and in hard to reach areas is approximately 50% higher than those in the wealthiest areas[7]. In underdeveloped countries, there is high death rate, birth rate is bound to be very high. Most of these children lived in developing countries and died from a disease or a combination of diseases or illnesses[8]. It was reported that the highest rates of mortality in under-five children continue to occur in Sub-Saharan Africa and South Asia has the second highest rate of under-five mortality in the world[6]. Many countries, especially in South Asia and Sub-Saharan Africa, are not on track to meet the target of MDG-4 (You et al., 2010). In India, yearly child mortality rates have fallen between 1.7%[9] and 2.3%[10] in the past two decades. But this figure corresponds to more than 20% of all deaths in children younger than 5 years worldwide, which is more than in many countries[5]. In Bangladesh, the IMR barely dropped from 168 infant deaths per 1,000 live births to 161 deaths during the two decades between 1951 and 1971. In the immediate aftermath of the independence of Bangladesh, the IMR actually increased to 173. But since then, the rate has fallen secularly and rapidly, reaching a level of 125 by 1984-85, 80 in 1994-95[11]. While there has been an appreciable drop in under-five death rates from 151 deaths per thousand live births in 1990 to 87 in 1999, the rate has since slowed considerably, with the figure standing at 82 in 2001[12]. The under-five mortality rate for the most recent five-year period (which roughly corresponds to the period 1999-2003) is 88 deaths per 1,000 live births, and infant mortality is 65 deaths per 1,000 life births. This means that 1 in 11 children born in Bangladesh dies before reaching the fifth birthday, while 1 in 15 children dies before reaching the first birthday[13]. Various studies have recently reported that IMR is 45 per 1000 live births[2] and under five mortality is 71[14] and 65[15] in this country. Neonatal and perinatal causes contribute to near half of all under five deaths[16] and most of deaths occur in the neonatal period[17]. One neonate dies in every three to four minutes, making 14 neonates deaths every hour in Bangladesh[7]. Although the recent decline in child mortality in Bangladesh is remarkable[18], but under-five mortality still remains high in Bangladesh due to high prevalence of malnutrition and childhood diseases. Since one third of the population is under 15 years age[2, 19], the infant and under-five mortality are sensitive indices of the level of development in every sector of Bangladesh. The target for Bangladesh related to MDGs is to reduce under five mortality from 151 per 1000 live births in 1990 to 50 in 2015[20]. For these reasons, under-five mortality in Bangladesh has long been a topic of interest to population and health researchers because of its apparent relationship with fertility and indirectly with acceptance of modern contraception[21]. Several studies have shown that various socio-economic, demographic, biological, cultural and environmental factor affects infant and under-five mortality. But the causal relationship and differentials between infant and under-five mortality through life table approach and its socio-economic and other covariates is not well established. Thus, the purpose of this study is to investigate the infant and under-five mortality level in Bangladesh through life table technique.
2. Sources of Data
- The data utilized in this study were extracted from Bangladesh Demographic and Health Survey (BDHS) 2004[13], for the ten year period preceding the survey (with a total sample size 7427, of whom 5004 from rural and 2423 from urban areas), having an eligible woman (ever married and aged 10-49) with at least one or more children, which were conducted by Mitra and Associates under the authority of the National Institute of Population Research and Training (NIPORT), Ministry of Health and Family Welfare, Bangladesh. The study is executed separately for the overall country level, rural level and urban level of Bangladesh.
3. Methodology
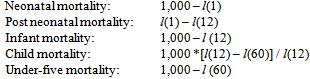
- Abridged life table techniques which are principally used to measure the level of mortality of the population involved have been performed to fulfill the objectives of this study. One of the main advantages over other methods of measuring mortality is that these does not reflect the effects of the age distribution of an actual population and does not require the adaptation of a standard population for acceptable comparisons of levels of mortality in different population. An abridged life table contains data by interval of 5 or 10 years of age. But, in this study, life-table computation uses age intervals of 0 month, 1–2 months, 3–5 months, 6–8 months, 9–11 months, 12–17 months, 18–23 months, 24–35 months, 36–47 months, and 48–59 months. Here, at first, it has been calculated probabilities of survival (lx) values in conventional life-table notation) at ages 1, 3, 6, 9, 12, 18, 24, 36, 48, and 60 months in terms of the number of survivors per 1,000 births (i.e., the l(0) is set to 1,000). Age-specific cohort mortality measures (deaths per 1,000) can then be computed from these probabilities of survival as follows:
 However, in this study, abridged life tables have been constructed using the number of deaths (xdn) in the interval x to xn based for the overall country level, rural level, urban level, male child, female child, literate mother, illiterate mother, rural male child, rural female child, urban male child, urban female child, currently working and currently not working mothers. It is to be noted that life tables, described in above, are called single decrement life tables as well as period life tables too. Life table age specific death rates, probability of dying and life expectancy are estimated using the formula ASDRs = dx/Lx, qx = dx/lx and ex = Tx/lx respectively, where the symbols are indicating as usual meanings.
However, in this study, abridged life tables have been constructed using the number of deaths (xdn) in the interval x to xn based for the overall country level, rural level, urban level, male child, female child, literate mother, illiterate mother, rural male child, rural female child, urban male child, urban female child, currently working and currently not working mothers. It is to be noted that life tables, described in above, are called single decrement life tables as well as period life tables too. Life table age specific death rates, probability of dying and life expectancy are estimated using the formula ASDRs = dx/Lx, qx = dx/lx and ex = Tx/lx respectively, where the symbols are indicating as usual meanings. 4. Results and Discussion
4.1. Patterns of Survival Function (lx) at Exact Age x
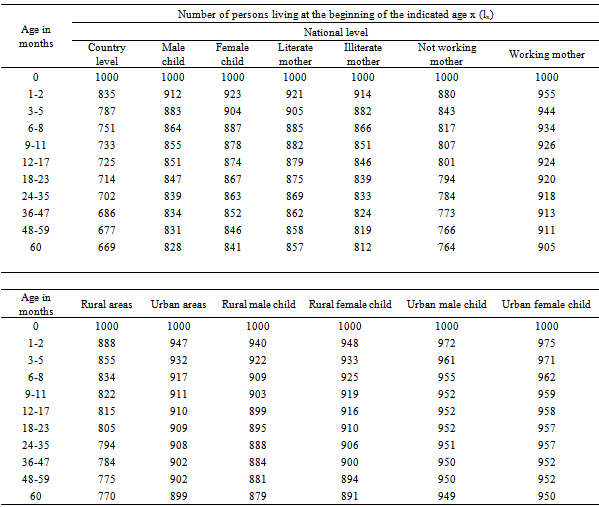
- The number of persons living at the beginning of the indicated age x out of the total number of births assumed as the radix of the table for the overall country level, male child, female child, literate mother, illiterate mother, currently not working mother, working mother, rural areas, urban areas, rural male child, rural female child, urban male child and urban female child have been calculated to selected ages and the results are presented in Table 1. To see the patterns, these surviving functions have been plotted in the graph paper and depicted in Figure 1- Figure 4.
|
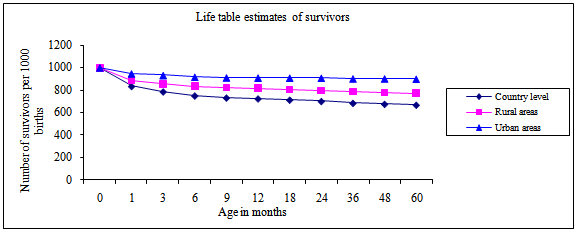 | Figure 1. The number of survivors for the overall country level, rural level and urban level |
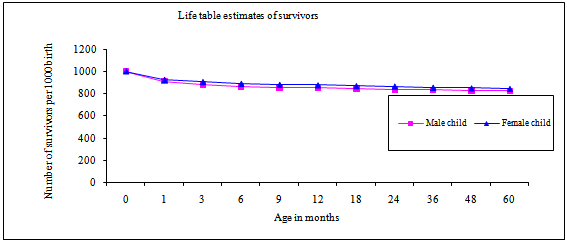 | Figure 2. The number of survivors for the male and female child |
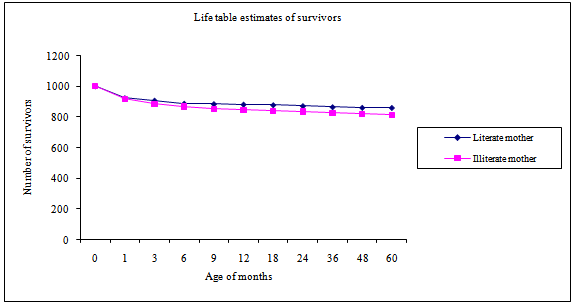 | Figure 3. The number of survivors for the literate and illiterate mothers |
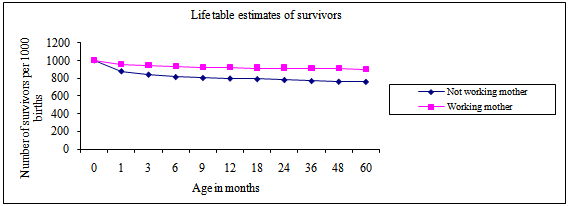 | Figure 4. The number of survivors for the not working and working mothers |
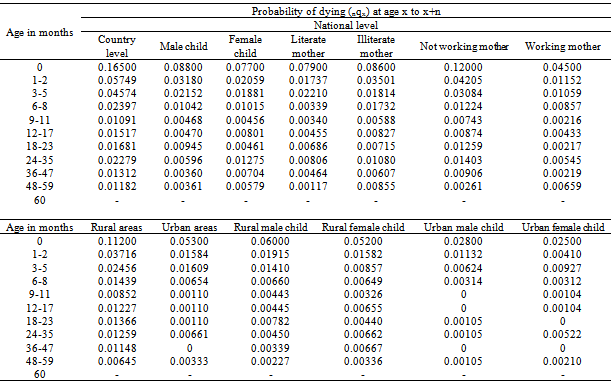
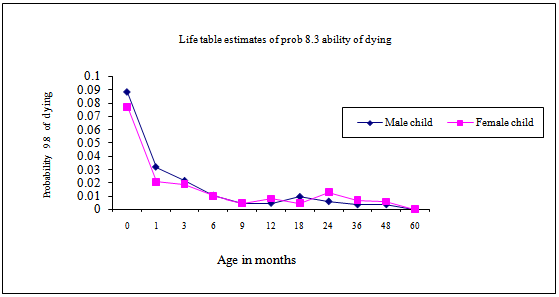
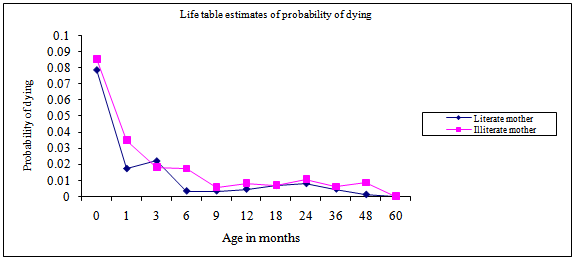
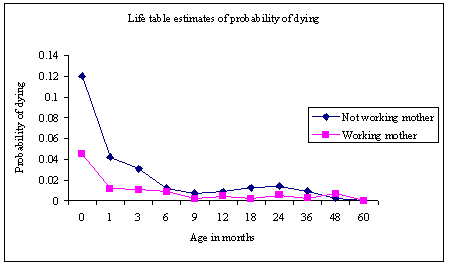
4.2. Patterns of Probability of Dying (nqx) between Age x to x+n
- The proportions of the persons in the cohort alive at the beginning of an indicated age x who will die before reaching the end of the age x+n have been calculated for the overall country level, male child, female child, literate mothers, illiterate mothers, currently not working mothers, working mothers, rural areas, urban areas, rural male child, rural female child, urban male child and urban female child and presented in Table 2. To observe the patterns of it for the overall country level, rural areas and urban areas, these have been plotted in the graph paper and depicted in Figure 5. From the figure, it is seen that the nqx function are decreasing with the increase of age. The pattern of the probability of dying of rural areas is higher due to ages than that of the urban areas of Bangladesh.In case of male and female child, the results are plotted in Figure 6 and it is seen that the probability of dying is higher in rural areas than the urban areas. The graph of nqx is higher for illiterate mothers than the literate (Figure 7). Moreover, it is seen that the probability for dying of not working mothers is more than that of the working mothers excepting last age group 48-59 (Figure 8).
|
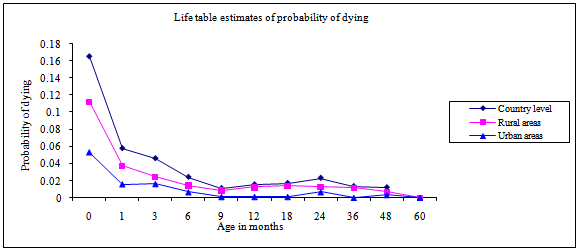 | Figure 5. The probability of dying for the overall country level, rural level and urban level |
 | Figure 6. The probability of dying for the male and female child |
 | Figure 7. The probability of dying for the illiterate and literate mothers |
 | Figure 8. The probability of dying for the currently not working and working mothers |
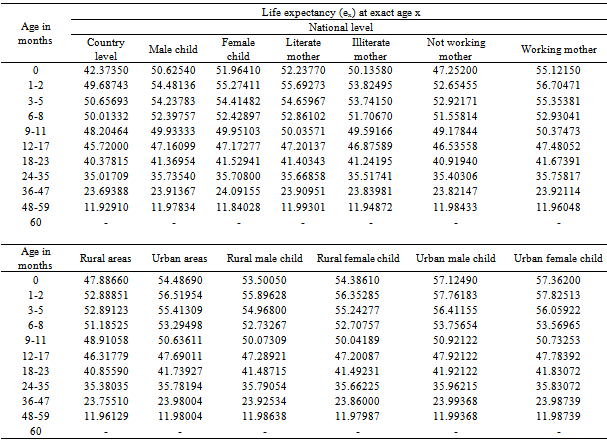
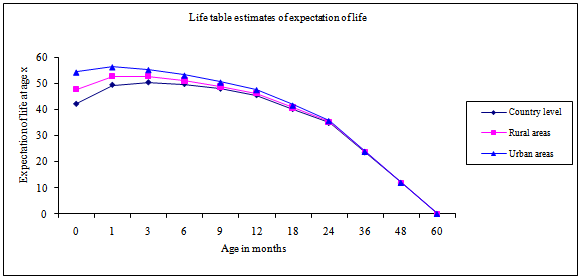
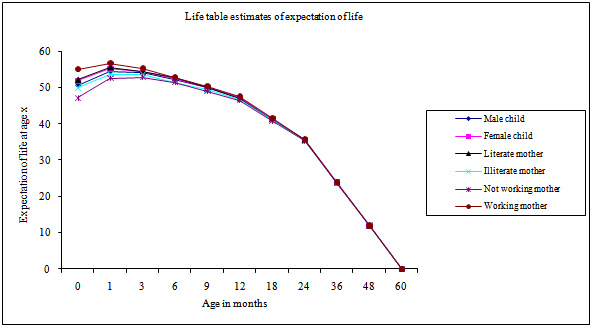
4.3. Patterns of Life Expectancy (ex) at Exact Age x
- The expectation of life (ex) at exact age x have been calculated corresponding to the selected ages for the overall country level, male child, female child, literate mother, illiterate mother, currently not working mother, working mother, rural areas, urban areas, rural male child, rural female child, urban male child and urban female child and the results are presented in Table 3. The results indicate that the life expectancy is higher for male child, literate mothers and currently working mothers than that of the female child, illiterate mothers and currently not working mothers respectively. To see the patterns, these expectation of life have been plotted in the graph paper and depicted in Figure 9 and Figure 10. From these figures, it is seen that the expectation of life for all the mentioned indicators exhibit same and traditional pattern. The expectation of life at birth for the overall country level is 42.37, for the male child is 50.62, for the female child is 51.96, for the literate mother is 52.24, for illiterate mother is 42.38, for currently not working mother is 47.25, for working mother is 55.12, for rural area is 47.89, for urban area is 54.49, for rural male child is 53.50, for rural female child is 54.39, for urban male child is 57.12 and for urban female child is 57.36 respectively. It is observed that the pecks of the curves of the expectation of life are showing increasing up to 1-2 age group and then start to decline with passing of time. It is also observed that the expectation of life are gradually increasing in the age interval[0, 5] and smoothly decreasing in the age interval[6, 59] for the overall country level and rural area of Bangladesh. But for the urban area, the expectancy of life are increasing in the age interval[0, 2] and smoothly decreasing in the age interval[3, 59]. It is also found that the maximum life expectancy for the overall country level and rural area are 50.66 and 52.89 respectively at age 3 months whereas it is 56.51 for the urban area at age 1 month.
|
 | Figure 9. The life expectancy for the overall country level, rural level and urban level |
 | Figure 10. The life expectancy for the male, female, literate, illiterate, working and not working mothers |
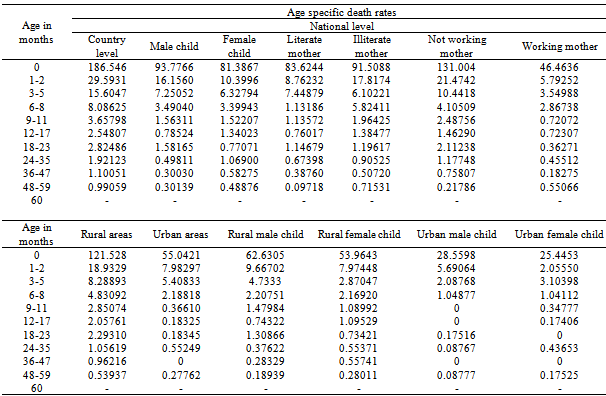
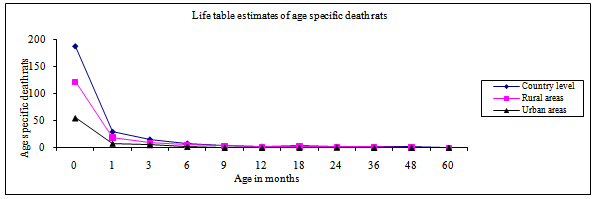
4.4. Patterns of Life Table Age Specific Death Rates (ASDRs)
- The life table age specific death rates for the overall country level, male child, female child, literate mother, illiterate mother, currently not working mother, working mother, rural areas, urban areas, rural male child, rural female child, urban male child and urban female child have been calculated to selected ages and the results are presented in Table 4. The results indicate that the ASDRs are higher among female child than the male child. But these rates are lower among the literate mothers than the illiterate mothers.To see the patterns of it for the overall country level, rural and urban areas of Bangladesh, these rates have been plotted in the graph paper and depicted in Figure 11. From the figure, it is seen that the ASDRs are high for the overall country level and it is low in urban areas than the rural areas. The ASDRs are also seen to be lower among urban male child than the rural male child. These rates are higher among illiterate and not working mothers than the literate and working mothers (Table 4) correspondingly.
4.5. Life Table Estimates of Mortality
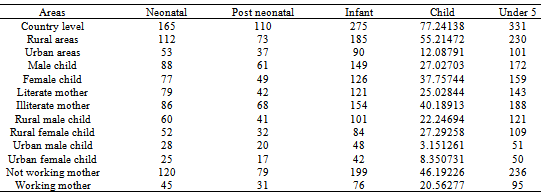
- Table 5 shows the mortality for selected age intervals estimated by abridged life tables for Bangladesh and for other characteristics. Under-five mortality is quite high in Bangladesh as a whole during the ten-year period before the survey, 331 per 1000 live births are estimated to have died before age five. Among the selected characteristics, estimated under-five mortality is higher among not working mother, rural areas, illiterate mothers and male child than working mothers, urban areas, literate mothers and female child respectively. Figure 12 shows the estimated infant (0-11 months) and under five mortality for Bangladesh and for the other selected characteristics.
|
 | Figure 11. The ASDRs for the overall country level, rural level and urban level |
|
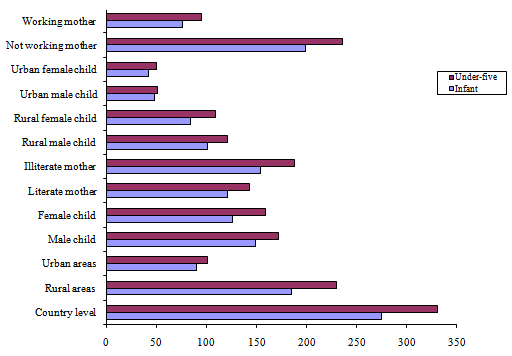 | Figure 12. Life table estimates of infant and under-five mortality |
5. Conclusions and Recommendations
- In the light of the study, it may conclude that the patterns of mortality vary due to ages and the mortality differences between rural and urban areas of Bangladesh are much larger at older ages than at younger ages. Also, the survival function decreases steeply throughout the period in both the rural and urban areas and these changes are little after the neonatal period. The probability of dying at ages is higher in rural areas than that of the urban areas. This study indicate that the life expectancy at ages of child under age five months is higher for literate mothers, working mothers and for female child at national level of Bangladesh than the illiterate mothers, not working mothers and male child respectively. Moreover, the life expectancy at each age of urban child is higher than the rural child but the pecks of the curves of the expectation of life are at 1-2 months for all the study areas and then start to decline with passing of time. Besides these, it is seen that the ASDRs among illiterate mothers, not working mothers and rural areas are higher than the literate mothers, working mothers and urban areas respectively. Also, it is higher among urban male child than rural male child. Furthermore, it is found that estimated under-five mortality is higher for not working mothers, rural areas, illiterate mothers and male child than that of working mothers, urban areas, literate mothers and female child correspondingly. It is recommended that education and employment status for women and planned urbanization should be boosted for reducing infant and under-five mortality in Bangladesh as well as in case of attaining MDG-4. Hope this study would be helpful for achieving MDGs as well as for policy makers, program designers/ planners to design or redesign program(s) or existing program(s) for reducing infant and under-five mortality.