-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Research in Obstetrics and Gynecology
p-ISSN: 2326-120X e-ISSN: 2326-1218
2017; 5(1): 10-20
doi:10.5923/j.rog.20170501.03

Use of Mobile Phone Short Text Message Service to Enhance Cervical Cancer Screening at Thika Level 5 Hospital, Kiambu County, Kenya: A Randomised Controlled Trial
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML1Kenyatta University, Department of Obstetrics & Gynecology, Kenya
2Kenyatta University, School of Public Health, Kenya
Correspondence to: Wanyoro A. K., Kenyatta University, Department of Obstetrics & Gynecology, Kenya.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Cervical cancer is a major public health problem among adult women especially in developing countries hence its control is of paramount importance. Organized screening programs have led to a large decline in cervical cancer incidence and mortality in developed countries. In Kenya, very few women at risk of the disease have regular repeat screening and there exists no effective recall mechanism to enhance scheduled screening. The Short Message Service (SMS) Text may be used as a recall tool to enhance cervical cancer screening in developing countries such as Kenya, where other communication means may not be easily available. A blinded randomized controlled trial was conducted where participants were recruited from among screening naïve patients at Thika Level 5 hospital. The participants were randomly allocated to an intervention (Short Message Service (SMS) text reminders) and a control (no SMS) arm. The study aimed to determine the influence of using SMS text reminders in enhancing adherence to scheduled repeat screening for cervical cancer. The mean age of the participants was 38.8 ± 10.8, most were married and of low socio- economic status. It was found that 67.1% of participants in the intervention arm and 20.3% in the control arm re-attended to rescreening making those who received SMS reminders 8 times more likely to adhere to scheduled rescreening than those who did not receive reminders (OR 8.02; CI 95% 4.69-13.73; p-<0.001). The study recommended that the Short Text Message Service (SMS) reminders should be integrated into the cervical cancer screening programs in resource constrained countries like Kenya.
Keywords: Cervical, Cancer, Screening, Adherence, SMS
Cite this paper: Wanyoro A. K., Kabiru E. W., Use of Mobile Phone Short Text Message Service to Enhance Cervical Cancer Screening at Thika Level 5 Hospital, Kiambu County, Kenya: A Randomised Controlled Trial, Research in Obstetrics and Gynecology, Vol. 5 No. 1, 2017, pp. 10-20. doi: 10.5923/j.rog.20170501.03.
Article Outline
1. Introduction
- Cervical cancer is a malignant condition of the cervix; the lowermost part of the uterus. Most of this cancer arises from the transformation zone with the commonest histological type being squamous cell carcinoma [1]. It is the second most common cancer among women worldwide, with an estimated incidence of over 500,000 and an annual mortality of over 250,000 [2]. Cervical cancer deaths rank fifth among all cancer related deaths in women worldwide [3] with almost 90% of the deaths occurring in developing countries [4-6].A close relationship has been observed between the incidence and mortality of cervical cancer in various geographical locations; with Africa and especially Eastern African region carrying the highest burden of the disease [7, 8]. Medical records from various hospitals in Nairobi, Kenya reveal that cervical cancer accounts for 70–80% of all cancers arising from the female reproductive tract with 10-15 new cases of cervical cancer being diagnosed weekly [9, 10]. This situation of high national incidence has been confirmed by data from the World Health Organization (WHO) [11]. Unless innovative ways are developed to address barriers to cervical cancer screening and early diagnosis among women at risk, the WHO has projected an increase of 50% cervical cancer cases by the year 2020 [12].Introduction of cervical cancer screening to women who has never undergone it before has been shown to drastically reduce cervical cancer incidence and mortality within less than three years of starting such services [13]. Globally, cytological screening tests using the Pappanicolou test (Pap test) have been shown to be one of the most successful cancer screening procedures. With a well-organized and timely screening of women at risk, deaths as a result of cervical cancer have been shown to be avoidable [12]. Availability of resources for cervical cancer screening and ensuring women at risk are regularly screened and remain in the cervical screening programs reduces the burden of cervical cancer significantly [14]. Kenya, like most Sub Saharan African countries, lacks effective well organized cervical cancer screening programs and hence the high rates of the disease.According to the World Health Organization (WHO), an organized system of calling women for screening and reminding them of scheduled screening when next due is key to making cervical cancer screening programs effective [15]. In the developed countries where screening programs are effective, women due for scheduled screening are informed of the next screening date through the mail, email or telephone calls. In the developing countries where the morbidity and mortality related to cervical cancer is very high, sending mail is difficult and most of the population has no access to computers or the fixed telephones. Recent introduction of the mobile phone has dramatically improved communication in many developing countries. Kenya has a wide coverage of the mobile phone network with many phones being used in small businesses and money transfers. The mobile phone subscription has continued to grow [16]. This fast evolving communications platform has been highly accepted across Africa giving the medical field a great and novel opportunity of integrating such platform in improving key health indicators [17]. The mobile phone has been used in 5 key areas of health including health care information, monitoring of compliance to treatment, health promotion, as a support tool to health workers for prevention of diseases and surveillance of diseases as well as in emergency medical response systems. The Short Text Message Service (SMS) is the primary feature of mobile phones that has been significantly documented to have good results especially when used for reminders [18-20]. The utility of the SMS reminders have not been tested as a reminder tool to enhance adherence to scheduled cervical cancer screening.
2. Methods
- This was a facility based single blind Randomized Controlled Trial (RCT) with an intervention arm of using 4 SMS reminders and a control arm where no SMS reminders were sent. Women who had never been screened for cervical cancer before and who were attending the General Out-patient Clinic at Thika Level 5 Hospital were randomly assessed for eligibility to the study. They were screened at baseline for cervical cancer and all those with normal cervical smears and consenting to the study were recruited. A data base was created using the participant’s mobile phone numbers. To improve access, the participants were also requested to provide an alternative mobile number of a significant other person such as a husband or a friend where reminder messages could be re-routed in case their phones were not working. Using their mobile phone numbers, the recruited participants were then randomly allocated to the intervention arm where four Short Message Service (SMS) Texts reminders were sent and a control arm, where no SMS text reminders were sent. Randomization was conducted using a computer based randomization program which helped to control for confounders and to allow homogeneity of the two arms.
3. Participants
- The study population was composed of eligible consenting women attending the general female outpatient’s clinics at the Thika hospital, Kenya. The inclusion criteria included women attending the general outpatient clinic, above 25 years of age, had never had cervical cancer screening before, who consented to the study, owned a mobile phone and consented to receive SMS through their mobile phones during the study period and had normal cervical smear after the initial baseline screening. Those who did not consent to the study or were unwilling to receive SMS as well as those with abnormal cytological smears, who had previous hysterectomies, who did not own a mobile phone, too sick and needed hospital admission, those with vaginal bleeding and those who were pregnant were excluded from the study. The sample size was calculated according to the formula developed by Chan for comparison of 2 proportions (two-sided) at 5% level of significance and 90% power [21]. In Kenya less than 5% of women have regular repeat Pap smear as scheduled and in this study it was assumed that the intervention would raise the percentage of women attending scheduled cervical cancer screening as per the pre-set schedule from 5% to 20% thus having an intervention effect of 15%. A minimum sample of 143 was needed in each arm making a total of 286 participants.
4. Recruitment
- Women attending the female outpatient clinic at the Thika Level 5 Hospital were assessed for eligibility at the outpatient clinic by the principal investigator and a research assistant. Eligible women who consented to participate signed an informed consent form and were then screened for cervical cancer after their outpatient care. To get a representative sample for inclusion into the study, systematic random sampling was employed. As per the hospital records approximately 20 women aged above 25 years attend the general outpatient clinic daily. To recruit 286 participants in 8 weeks we aimed to recruit 8 study participants each working day until the sample size was acquired. Hence a sampling interval of 2 was employed. The first 8 women attending the general outpatient clinic were presented with 8 opaque folded papers. Each paper was marked from 1 to 8. Each of the 8 women picked one piece of paper. The woman who picked the paper marked with number 1 was considered as the first in the sequence and from then every second eligible woman who consented was invited and recruited for the study. If the sampled woman was not eligible, the next eligible woman was recruited. Those recruited had their baseline data recorded. They were then screened for cervical cancer using the Pappanicolou cytological. This process was followed until the sample size was saturated.
5. Randomization and Blinding
- A database of the study participant’s mobile phone numbers was developed. Using the participant’s mobile phone numbers, a 1:1 computer generated random allocation was performed allocating participants into an intervention arm (4 SMS reminders) and control arm (no SMS reminders). This allocation was concealed and blinded to the principal investigator and his assistant. A software expert developed and administered the system and was not blinded to the study. The system was set to automatically randomly allocate the study participant’s by their mobile phone numbers to either the intervention or control arm. The system subsequently sent the SMS text reminders automatically as per the pre-determined schedule to those 143 participants in the intervention arm while the 143 participants in the control arm did not receive reminders. If the participant’s mobile phone number was unreachable the SMS was automatically routed to the alternative number through the computer program. The system first put the mobile phones data in clusters so as to prevent a skewed selection of participant’s to receive reminders as participants were registered and registered chronologically. To determine the number of blocks the following function was used: B = P*i*logN: Where B……optimum number of blocks, P……proportion determined by data size (Number of participants)/Number to be selected, i……average interval size, N……Data size (Number of participants). For this study, the optimum number for 286 participants and 50% selection was 7 blocks. Data was then divided into the blocks to get the block size of each block. Using the seven blocks and dividing 286 by 7 blocks, the size if each block was 40 participants. Therefore for every 40 participant’s clustered together, 20 were randomly allocated into the intervention group while the rest were allocated to the control group.
6. The Intervention
- The participants in the intervention arm received reminders via Short Message Service (SMS) texts to remind them of the next scheduled cervical cancer screening. This was set to be done in a period of 2 weeks, which was exactly one year after the baseline screening. For this study four (4) Short Service Messages (SMS) Texts were automatically sent using a computer program to the intervention group at three months, two months, a month and a week before their next repeat screening. If the study participant’s mobile phone number was unreachable the SMS text was automatically routed to the alternative numbers. This allocation was blinded to the investigator until un-blinding was done. For participants in the control group, the date of next scheduled repeat screening was verbally given and noted on the participant’s card as is the routine standard of care in cervical cancer screening program.
7. Follow up
- The study participants were followed up with subsequent re-screening for cervical cancer using cytological smears at end line. The 286 study participants with initial normal Pap tests were scheduled for rescreening exactly 12 months after the baseline screening. The screening was to occur over a two weeks period. A participant was deemed adherent to scheduled re-screening if she was screened for cervical cancer at the same site (Thika Level 5 Hospital) during the two weeks rescreening period.
8. Statistical Analysis
- Data verification, cleaning and analysis was conducted using STATA version 11 (STATA Corp, College Station, Texas, USA). Analysis was done on Intent to Treat (ITT) analysis principle [22]. Categorical variables were summarized by frequencies and proportions while continuous variables were summarized by means and standard deviations. Uni-variable descriptive analysis was used to describe the characteristics of the sample population. Chi square test was used to establish the relationship between various categorical variables. Bi-variable analysis was used to determine the relationship between the independent variables and dependent variable. Logistic regression was conducted to determine the influence of the SMS text reminders on repeat scheduled screening. Multiple logistical regressions were conducted to determine the influence of various independent variables on adherence to scheduled screening. The study findings were presented as per the Consolidated Standards of Reporting Trials (CONSORT) guidelines [23].
9. Ethical Considerations
- Ethical approval was sought from the Kenyatta University Biomedical Research Ethics Review Committee. The participant’s with abnormal cervical lesions and overt cervical cancer were given the standard care such as colposcopy, surgery or radiotherapy. The study was registered with the Pan African Clinical Trials Registry (PACTR20130500052 6384).
10. Results
10.1. Summary of the Trial Reporting
- During the period between 15th April to 14th June 2014, 964 eligible women attended the general female outpatient’s clinic and were assessed for recruitment. Out of this, 193 women were excluded as they had been screened for cervical cancer before. The rest (771) were consented and systematically randomly sampled to get the study sample.
10.2. Comparative Analysis of Socio-demographic Characteristics of the Trial Arms
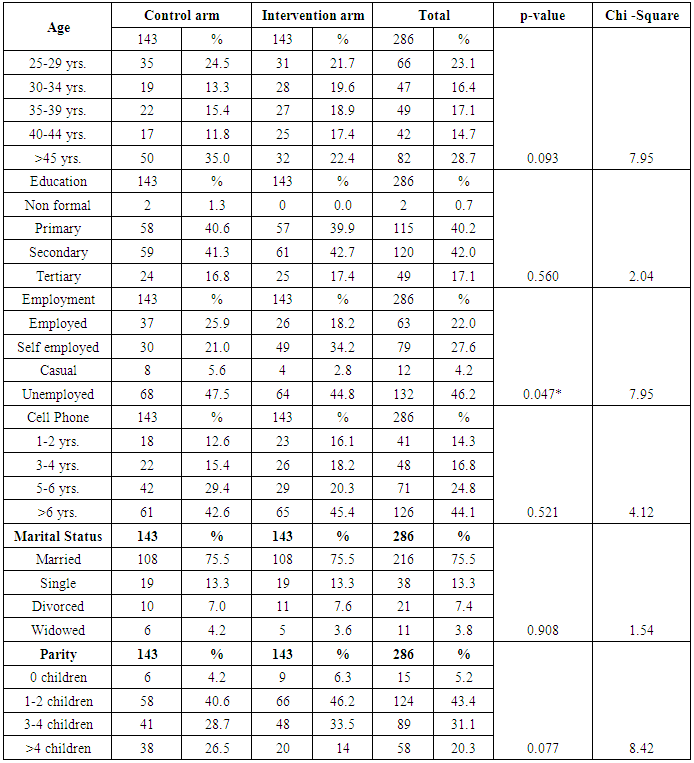
- Table 1 compares socio-demographic characteristics of the two study arms which were done after unmasking the study. When age, education level, marital status and parity of the study participants in the two arms were compared, there was no statistical difference confirming that the two arms were the same. Only the employment status showed a significant difference. (p<0.05)
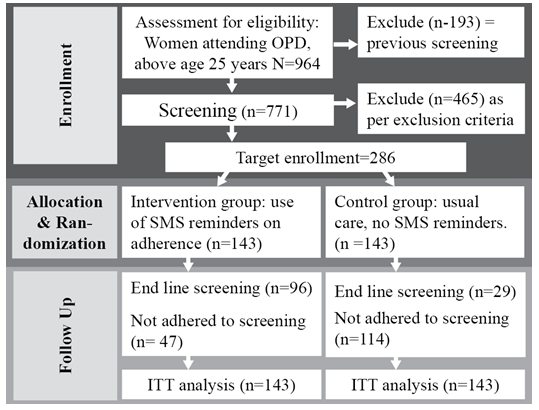 | Figure 1. Study Consolidated Standards of Reporting summary |
|
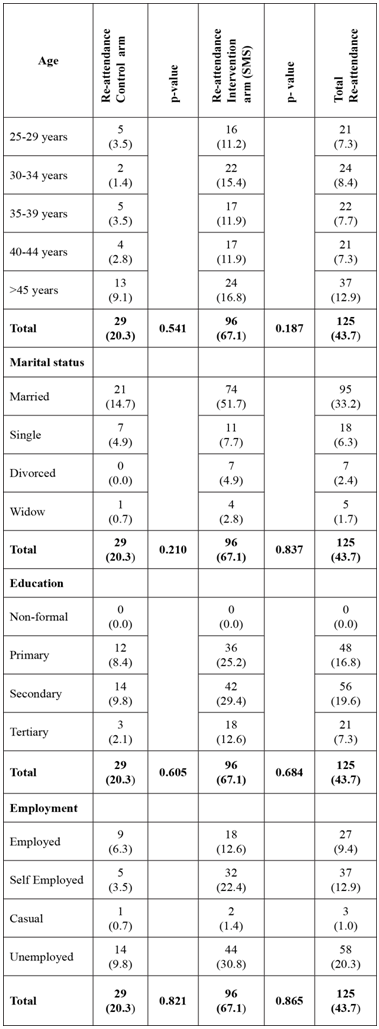
10.3. Socio-demographic Characteristics of the Study Participants
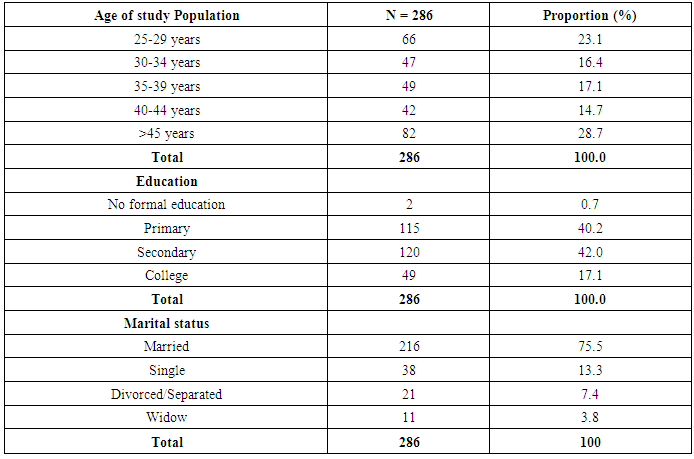
- Table 2 shows the socio-demographic characteristics of the study participants. The mean age of the participants was 38.8 ± 10.8. The youngest participants were 25 years old and the oldest were 70 years old. Most of the study participants (82.2%) had primary or secondary school education with (75%) of them being married.
|
10.4. Socio-economic Characteristics of the Study Participants
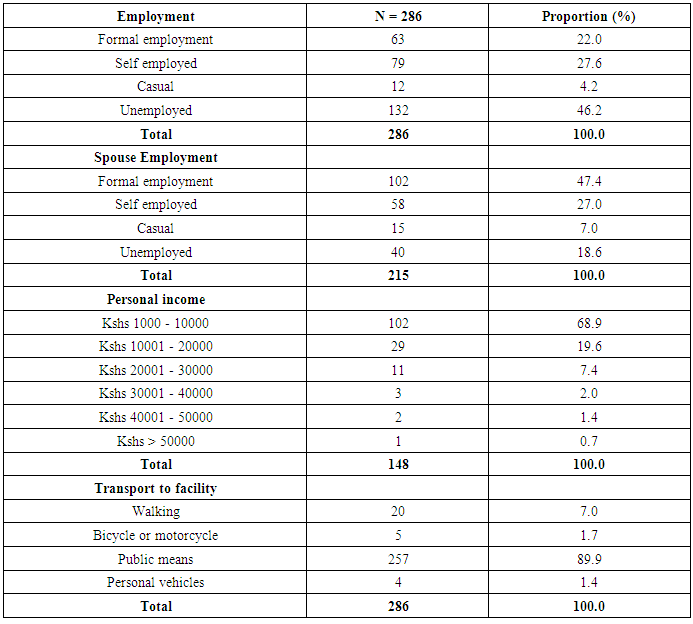
- Table 3 shows the socio-economic characteristics of the study participants. It was found that almost half (46.2%) of the participants were unemployed. Only 22% of the participants were formally employed whereas 27.6% were self-employed. Majority of the participants (84%) earned less than 10,000 Kenya Shillings per month. Out of the 248 participants who were married, only 47.4% of the husbands were formally employed. Majority of the study participants (90%) used public transport to access the hospital.
|
10.5. Impact of the using the SMS Reminders on Re-attendance to Scheduled Cervical Cancer Screening
- Figure 2 shows the repeat cervical cancer screening re-attendance of the study population from the two study arms as per schedule one year after the baseline screening. The overall re-attendance rate to scheduled screening of the entire study participants was 43.7% (125/286). More than half of the study population (56.3%) (161/286) did not attend the scheduled screening. Out of the interventional group, 96/143 (67.1%) re-attended as scheduled while only 47/143 (32.9%) did not re-attended. From the control arm, only 29/143 (20.3%) re-attended whereas 114/143 (79.7%) did not re-attend as scheduled for rescreening. This shows that if women are not reminded only a fifth are likely to attend regular screening as scheduled even with counselling on the need to have regular screening. On the other hand if women are reminded of the next scheduled screening using four short messages, 2 out of 3 would likely re-attend as scheduled. This would translate to attaining the World Health Organization recommendation of having 70% of women at risk being kept in the screening cycle; a fact that would lead to a significant impact in reducing cervical cancer.
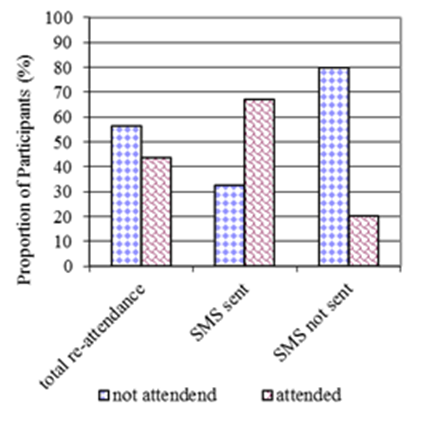 | Figure 2. Re-attendance to scheduled cervical cancer screening of the study population at end line |
10.6. Influence of Socio-demographic Characteristics on Re-attendance
- In order to determine the influence of the socio-demographic factors on the re-attendance, bi-variable analysis was conducted. Table 4 shows that none of the socio-demographic factors; age, marital status, level of education and employment levels influenced re-attendance in either arm (p>0.05).
|
10.7. Influence of SMS Text Reminders on Re-attendance to Scheduled Re-screening for the Study Participants
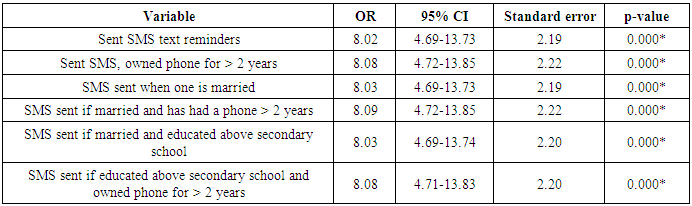
- In order to determine the influence of sending four SMS reminders on adherence to scheduled repeat screening of participants who had a normal Pap smear at baseline simple regression analysis was conducted. As Table 5 shows, the participants who received SMS text reminders were 8 times more likely to adhere to the scheduled rescreening than those who did not. The difference was highly statistically significant (OR 8.02; CI 95% 4.69-13.73; p<0.001).
|

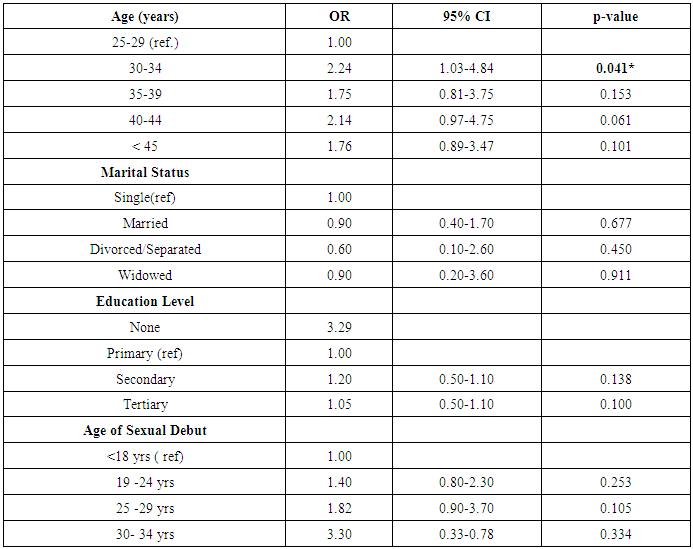
10.8. Influence of Individual Socio-demographic on Adherence to Repeat Scheduled Screening after using SMS Reminders
- As shown in Table 6 on the influence of individual socio-demographic factors on adherence to scheduled screening, participants aged 30-34years were more likely to adhere to re-attendance after being sent SMS text reminders (OR 2.24 CI 1.03-4.84 p<0.05) compared to the reference age 25-29 years. All the other age groups did not show a significant influence. When regression analysis was conducted, education status did not seem to have any influence on adherence to attendance to scheduled screening after reminders. Although the adherence to scheduled screening seemed to increase with age of sexual debut for participants who received the SMS text reminders (OR 1.4 in age 19-24 years, 1.82 in age 25-29 years and 3.3 in those aged 30-34 years), the difference was not statistically significant (p>0.05).
|
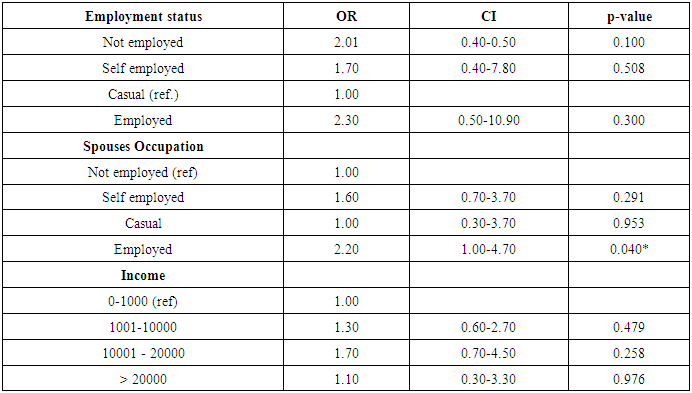
10.9. Influence of Individual Socio-economic Factors on Adherence to Repeat Scheduled Screening after using SMS Text Reminders
- As shown in Table 7, participants who were not employed were more than 2 times likely to adhere to rescreening as scheduled, compared to those in casual employment after SMS text reminders. Those who were employed were 2.3 times likely to adhere to scheduled screening after SMS text reminders. However these differences in re-attendance were not statistically significant (p>0.05). Participants whose spouses were employed were 2.2 times more likely to adhere to scheduled rescreening after being sent SMS text reminders. This difference was statistically significant (OR 2.2 CI 1-1.47 p<0.05).
|
10.10. Multi-variable Regression Analysis
- Table 8 shows the outputs of multiple variable regression analysis. It was found the participants who received SMS text reminders and had owned a mobile phone for more than 2 years were 8.08 times more likely to adhere to the scheduled rescreening; a difference that was found to be highly statistically significant (OR 8.08 CI 95% 4.72-13.85, p<0.001). Those sent SMS text reminders and were married were 8.03 times more likely to re-attend as scheduled (OR 8.03 CI 95% 4.69-13.73, p<0.001). Those sent SMS and were married and had owned a mobile phone for more than 2 years were 8.09 times more likely to re-attend (OR 8.09 CI 95% 4.72-13.85, p<0.001). There was also a very slight increase in the odds for adherence to rescreening (OR 8.03) if one was sent an SMS and was educated above secondary school level and was married.
|
10.11. Influence of access Factors on Adherence to Repeat Scheduled Screening after using SMS Reminders
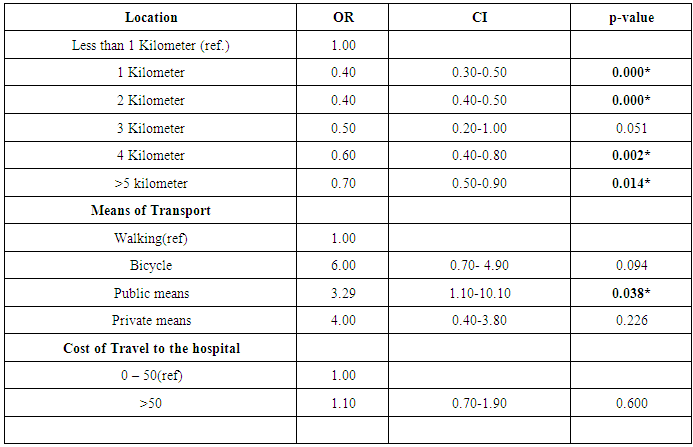
- Table 9 shows the influence of access factors on adherence to repeat scheduled screening after using SMS reminders. The closer the person was to the hospital, the less the likelihood that they re-attended. This difference was statistically significant for those who lived within one to two kilometers from the hospital (OR 0.3 and 0.4, p<0.001). It was found that those participants who used public transport to access the hospital had a 3.29 chance of adhering to scheduled rescreening after being sent SMS text reminders (OR 3.29 CI1.1-10.1 p<0.05). When regression was conducted to compare those who used less than 50 shillings for transport and those who used more, there was no statistical difference (OR 11; CI 0.7-1.9; p >0.05).
|
11. Discussion
- For a program of cervical cancer screening to have a significant impact in reducing the morbidity and mortality associated with the disease, at least 70% of women at risk should be put in the cervical cancer screening cycle [24]. Many studies have looked at methods of trying to increase the number of at risk women entering into and remaining in the cervical cancer screening cycle [25-27]. In the United Kingdom a call system evaluation study found that using such a system was able to raise the percentage of women in the cervical screening cycle from 58 to 84% [28]. In their meta-analysis Seng and his colleagues [29] found that sending letter reminders on screening for cervical cancer significantly improved the screening rate by 64% compared to the non-interventional group. Even in countries like Belgium where screening programs are well attended the effect of inviting non attendees using letters significantly increases attendance to screening [30]. However, the above studies did not look at the efficacy of using the mobile phone platform. The fast growing mobile phone platform has offered new opportunities by placing tools and information in the hands of people seeking health related services. Acceptability of the mobile phone has led to an increased interest in the use of the SMS platform of a GSM phone to solve many social problems. Many studies conducted in the developed countries have shown benefits on the use of the mobile phones devices in enhancing access to health care and provision of medical education [17], promotion of health [19, 20, 31], adherence to treatments regiments [32] as well as for management of clinic appointments [33-35]. The platform has also been shown to be useful in disease surveillance, collection of health information, improving adherence to treatment of chronic illnesses as well as in promotion of health [19]. Application of the mobile phone SMS platform in improving behavior change for health promotion has proved to be a very efficient tool [35, 36]. The few studies that have been done in countries like Kenya have investigated use of mobile phone platform for appointment reminders in the management of infectious diseases such as Tuberculosis (TB) as well as for Antiretroviral (ARV) treatment compliance for HIV management where there is proof that use of mobile phone technology is feasible and acceptable in diverse settings [37, 38]. The SMS simplicity and cost effectiveness compared to telephone calls has also been proved beyond any doubt in its application to health care [38]. In this study the intervention was four (4) SMS remainders on the next scheduled cervical cancer screening dates compared to a control group where no SMS reminders were sent. It was found that of those participants in the interventional group 67.1% re-attended the scheduled repeat cervical cancer screening while only 32.9% did not. This was in contrast to what was found in the control group where it was found that only 20.3% re-attended as scheduled while 79.7% did not. The re-attendance for cervical cancer screening as scheduled was found to be 8 times more likely when SMS reminders were sent compared to not sending an SMS. This was found to be statistically significant (p<0.001 95% CI 4.69-13.73). The results clearly demonstrate that the SMS reminders as a tool to enhance adherence to cervical cancer screening is as efficacious in women attending the general outpatients’ clinic just as it has proved successful in other areas of health care [38, 39]. It also underscores the fact that many other studies have found that calling and recalling women for cervical cancer screening increases the screening re-attendance [25-27]. Socio-demographic factors such as low socio-economic status, age and education status have been found to influence re-attendance to screening for cancer of cervix. For example women of low socio-economic status and women who are elderly have been found to be less likely to be regularly screened [40, 41]. In this study, age of the participants, their spouses’ employment status and means of transport were found to have a positive influence on re-attendance after using the SMS reminders. Participants aged between 30 to 34 years had a more than 2 times likelihood to re-attend for rescreening compared with others after sending the SMS reminders (OR 2.24 CI 1.03-4.84 p<0.05). Spouse’s employment was also found to have a positive influence. After sending the SMS reminders, those participants whose spouses were employed were found to have a significant re-attendance rate of more than two times compared to those whose spouses were not employed (OR 2.2 CI 1-1.47 p<0.05). This may be due to the support that an employed spouse may give to a wife who needs to re-attend screening. Among access factor the use of public means was also found to have a significant influence on re-attendance after sending an SMS reminder (OR 3.29 CI1.1-10.1 p<0.05). Other socio-demographic factors like income, education level, marital status, location, cost of travel and time taken to travel did not have significant influence and in fact the nearer the person came to the screening site and the less money spent to travel was seen to have a negative influence to screening re-attendance when using the SMS. The re-attendance after sending an SMS reminder in participants who have never been screened did not seem to depend on health beliefs perceptions such as those of susceptibility, seriousness, risks, benefits or barriers. This is unlike many studies that have been conducted in the developed countries where reasons of women not been regularly screened included perception that the test is not beneficial, women not considering themselves at risk and considering the test being unnecessary [42-44]. However there was a clear trend when perceptions of seriousness and benefits were considered. This is unlike what is predicted in the health belief model which predicts that if belief of being more susceptible to a particular disease is high; and that the disease is severe and the benefits of being screened are high, chances of that person being screened are increased compared to those with lesser perception [45, 46]. The trend observed in influence of perceptions on repeat screening in this study could be attributed to the fact that participants who had low perceptions on their risks and seriousness as well as lower risk of benefits could have been influenced more by the SMS reminders and counseling with a possible increase in perception and hence re-attendance. However when the differences were subjected to significance testing, they did not show any statistical significance.
12. Limitations and Strength of Study
- The study was a facility based study. This may limit the generalizability of the study to other areas.
13. Conclusions
- Using 4 SMS reminders to remind women of the date of the next scheduled screening increases the chances of re-attendance up to 8 times compared to those not reminded. Women aged between 30-34 years, those whose spouses are employed and those who use public means of transport were more likely to return after being reminded using the SMS texts. Other socio-demographic factors as well as health beliefs to cervical cancer screening did not seem to significantly influence re-attendance to scheduled screening when using the SMS reminders. To enhance adherence to scheduled screening, the government through Public Private Partnership should explore ways to incorporate the Short Message Service (SMS) Texts as a reminder tool for next scheduled screening into the National Cervical Cancer Screening Program. Majority of the study participants had high acceptance on the use of the SMS for reminders and therefore this platform should be utilized to educate women at risk of developing cancer of the cervix on the need for regular screening.The SMS reminders should therefore be integrated into the cervical cancer screening in countries with increased burden of cervical cancer like Kenya where other means of reminders are not available. This would eventually lead to reduction of incidences of cervical cancer as well as increase early diagnosis for improved treatment outcomes.
ACKNOWLEDGEMENTS
- The researcher appreciates the efforts of Prof. Kabiru and Prof. Bukusi who supervised this work, Ann Mbula for helping in the filling of baseline information, Raphael and Ndiaga for helping with analyzing the cytology smears. Appreciation also goes to Mr Mungai for helping in the creation of the IT system and Rono for typesetting the document. Much appreciation also goes to the hospital administration and the staff for allowing the study to be conducted in the facility as well as to all the study participants for giving consent to participate in the study.